All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub uses cookies on this website. They help us give you the best online experience. By continuing to use our website without changing your cookie settings, you agree to our use of cookies in accordance with our updated Cookie Policy
Introducing

Now you can personalise
your Lymphoma Hub experience!
Bookmark content to read later
Select your specific areas of interest
View content recommended for you
Find out moreThe Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.









ASH 2016 | Durable responses with single-agent ibrutinib in treatment naïve or R/R CLL/SLL – 5-year follow up of Phase Ib/II PCYC-1102 trial
Bookmark this article
On 3–6 December 2016 in San Diego, CA, the 58th Annual Meeting & Exposition of the American Society of Hematology (ASH) took place. On Saturday 3rd December, an oral abstract session was held between 4:00pm and 5:30pm in the “CLL: Therapy, Excluding Transplantation Program” category. This session was moderated by Tait D. Shanafelt, MD, of the Mayo Clinic, and John F. Seymour, MB, BS, PhD, FRACP, of the Peter MacCallum Cancer Centre and Royal Melbourne Hospital.
Abstract #233 was presented during this session, titled “Five-Year Experience with Single-Agent Ibrutinib in Patients with Previously Untreated and Relapsed/Refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Leukemia” by Susan M. O’Brien, MD, of the Chao Family Comprehensive Cancer Center, University of California, Irvine, Orange, CA, and colleagues.
In this abstract, efficacy and safety results of the longest-follow up to date for ibrutinib treated patients in the phase Ib/II PCYC-1102 trial were presented. Patients were either administered with 420 or 840mg ibrutinib QD until disease progression or unacceptable toxicity. Thirty-one treatment naïve and 101 R/R patients with CLL were enrolled with a median age of 68 years (37–84). R/R patients had a median number of 4 prior treatments (1–12). For all patients, median time on study was 46 months (0–67). For treatment naïve patients, median time on study was 60 months (0–67.4) and for R/R patients was 39 months (0–67).
- Per investigator, ORR for all patients = 86% (CR = 14%)
- ORR for treatment naïve patients = 84% (CR = 29%)
- ORR for R/R patients = 86% (CR = 10%)
- Median PFS for treatment naïve patients and R/R patients not reached and 52 months, respectively
- 5-year PFS for treatment naïve and R/R patients were 92% and 43%, respectively
- 5 year OS for treatment naïve and R/R patients were 92% and 57%, respectively
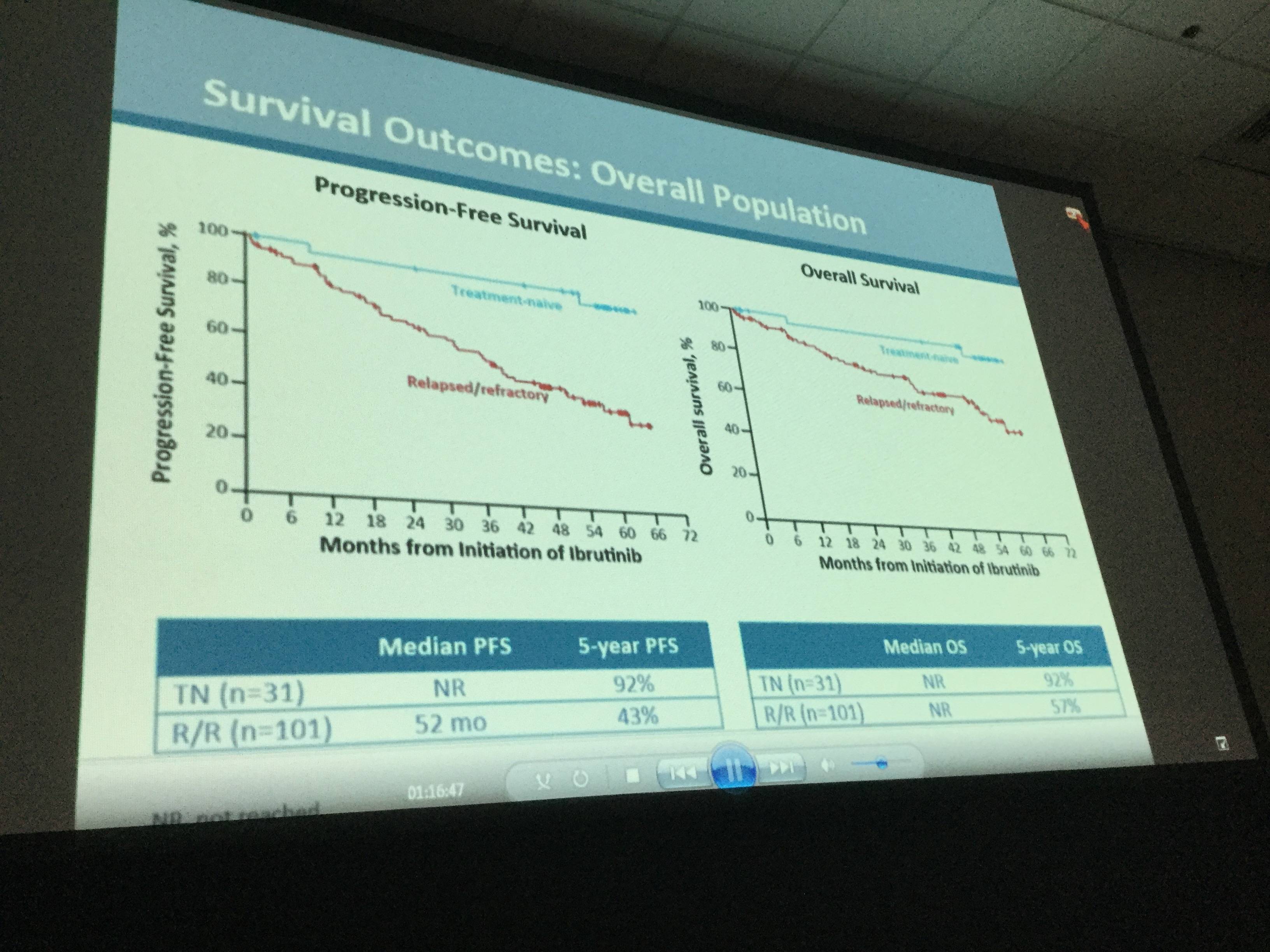
- Median DoR for treatment naïve and R/R patients was not reached and 45 months, respectively
- Among all patients who were treated, occurrence of ≥ grade 3 AEs was highest in the first 12 months of treatment and decreased during the subsequent years
- After approximately 5-years of follow-up, the most common ≥ grade 3 AEs were hypertension (26%), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%)
- Treatment was discontinued in 27 patients (20%) due to AEs and in 34 patients (26%) due to disease progression
- Of all patients treated, 38% are still on ibrutinib therapy, including 30% of R/R patients and 65% of treatment naïve patients
This talk concluded by stating that single-agent ibrutinib continues to show durable responses in patients with CLL, either treatment naïve or R/R.
Abstract
Background: Ibrutinib (ibr), a first-in-class, once-daily Bruton’s tyrosine kinase inhibitor, is approved by the US FDA for treatment of patients (pts) with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) including pts with del17p. The phase 1b/2 PCYC-1102 trial showed single-agent efficacy and tolerability in treatment-naïve (TN; O’Brien, Lancet Oncol 2014) and relapsed/refractory (R/R) CLL/SLL (Byrd, N Engl J Med 2013). We report efficacy and safety results of the longest follow-up to date for ibr-treated pts.
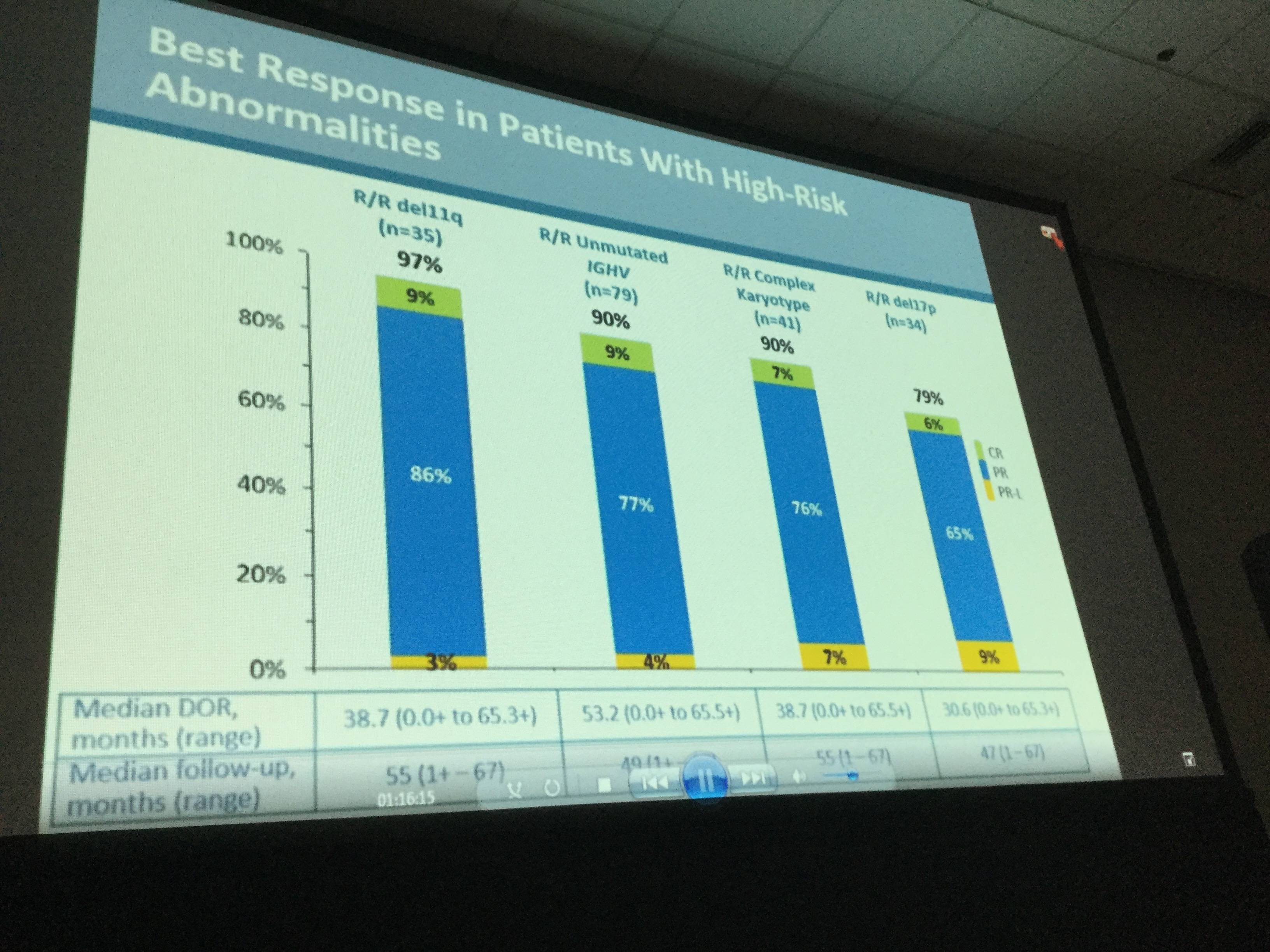
Methods: Pts received 420 or 840 mg ibr QD until disease progression (PD) or unacceptable toxicity. Overall response rate (ORR) including partial response (PR) with lymphocytosis (PR-L) was assessed using updated iwCLL criteria. Responses were assessed by risk groups: unmutated IGVH, complex karyotype (CK; ≥3 unrelated chromosomal abnormalities by stimulated cytogenetics assessed by a reference lab), and in hierarchical order for del17p, then del11q. In the long-term extension study PCYC-1103, grade ≥3 adverse events (AEs), serious AEs, and AEs requiring dose reduction or discontinuation were collected.
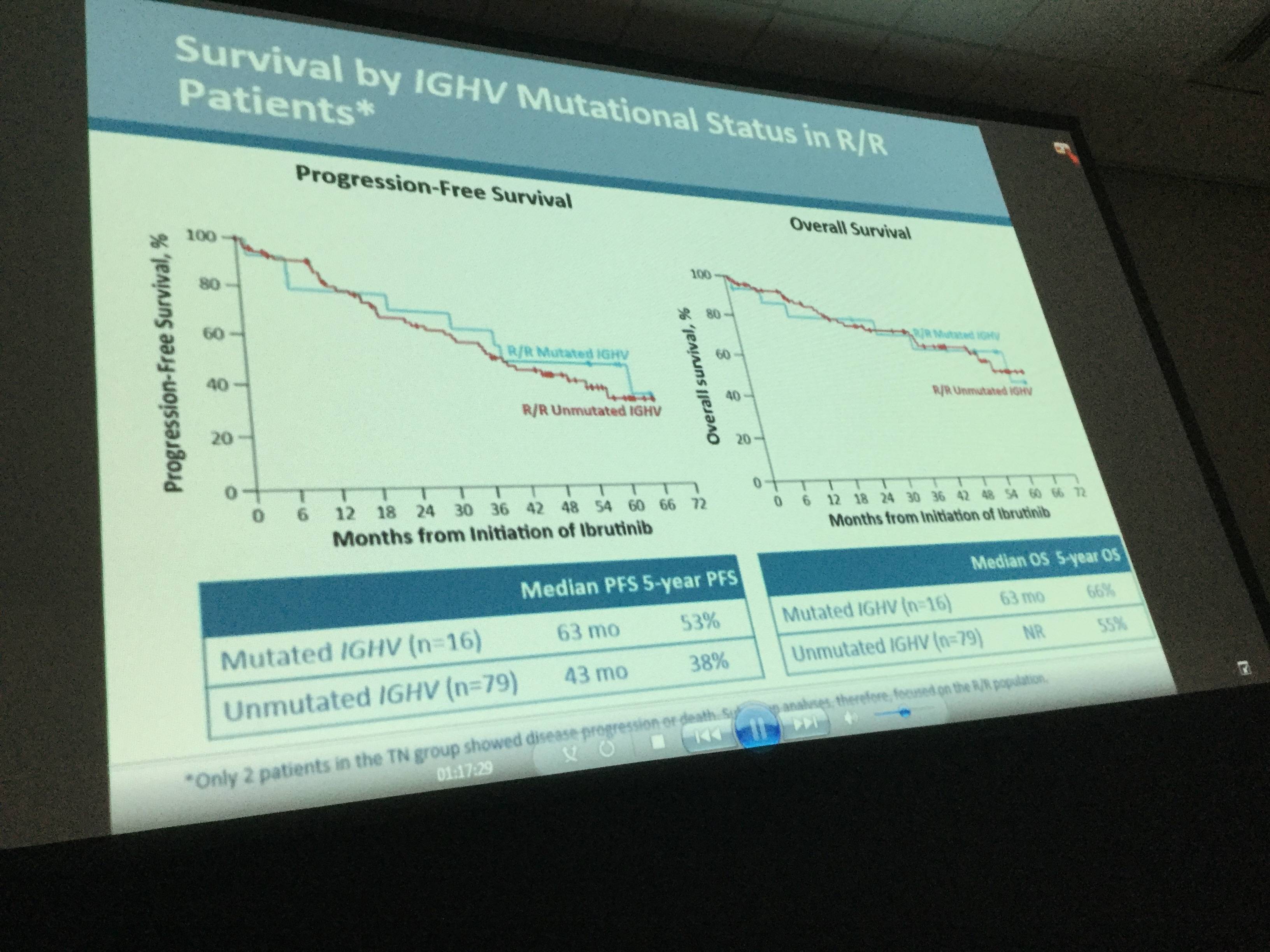
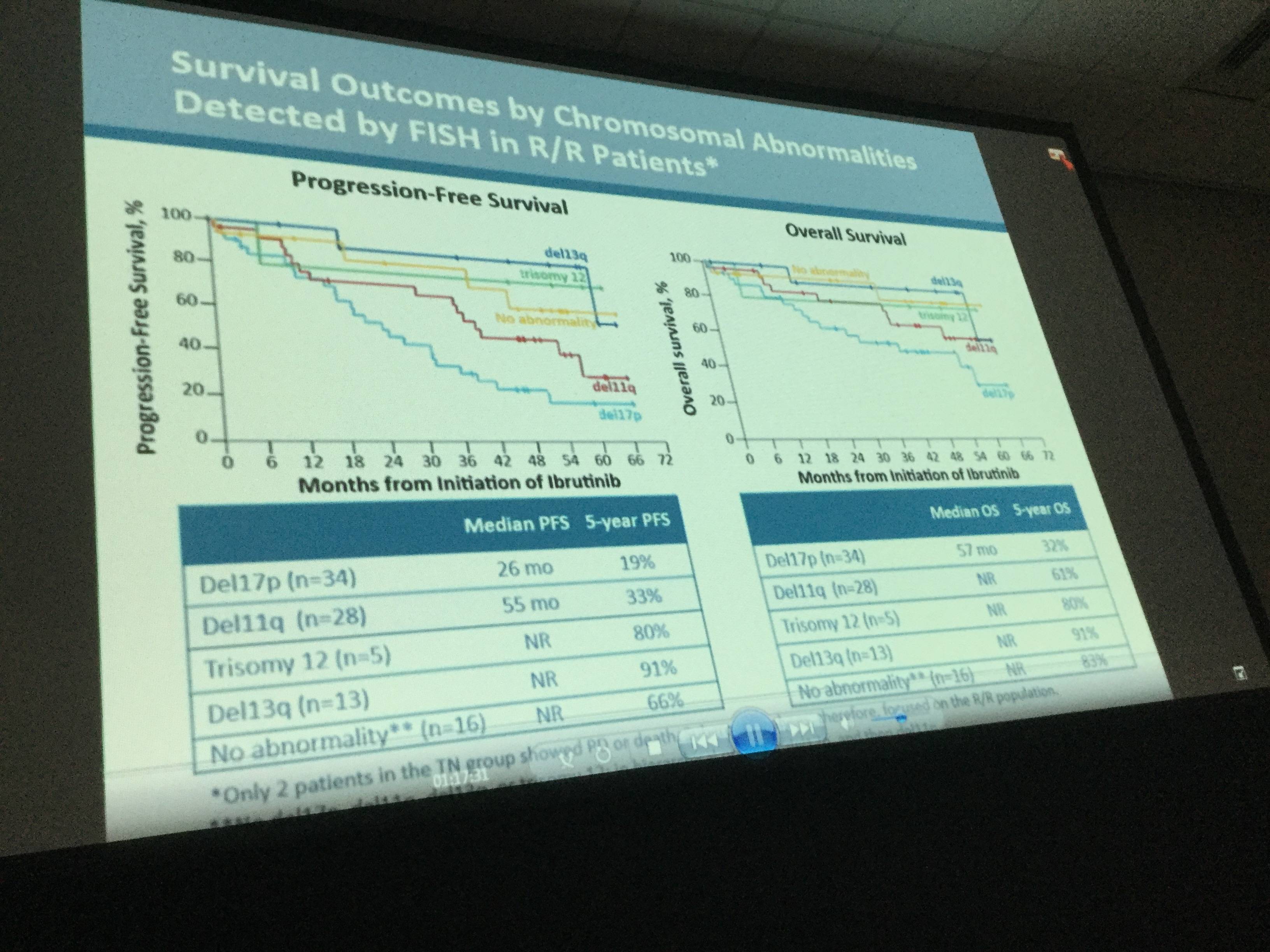
Results: Median age of the 132 pts with CLL/SLL (31 TN, 101 R/R) was 68 y (range, 37–84) with 43% ≥70 y. Baseline CK was observed in 41/112 (37%) of pts. Among R/R pts, 34 (34%) had del17p, 35 (35%) del11q, and 79 (78%) unmutated IGVH. R/R pts had a median of 4 prior therapies (range, 1–12). Median time on study was 46 m (range, 0–67) for all-treated pts, 60 m (range, 0–67.4) for TN pts, and 39 m (range, 0–67) for R/R pts. The ORR (per investigator) was 86% (complete response [CR], 14%) for all-treated pts (TN: 84% [CR, 29%], R/R: 86% [CR, 10%]). Median progression-free survival (PFS) was not reached (NR) for TN and 52 m for R/R pts with 60 m estimated PFS rates of 92% and 43%, respectively (Figure 1). In R/R pts, median PFS was 55 m (95% confidence intervals [CI], 31–not estimable [NE]) for pts with del11q, 26 m (95% CI,18–37) for pts with del17p, and NR (95% CI, 40–NE) for pts without del17p, del11q, trisomy 12, or del13q. Median PFS was 33 m (95% CI, 22–NE) and NR for pts with and without CK, and 43 m (95% CI, 32–NE) and 63 m (95% CI, 7–NE) for pts with unmutated and mutated IGVH, respectively (Figure 2). Among R/R pts, median PFS was 63 m (95% CI, 37–NE) for pts with 1-2 prior regimens (n=27, 3 pts with 1 prior therapy) and 59 m (95% CI, 22–NE) and 39 m (95% CI, 26–NE) for pts with 3 and ≥4 prior regimens, respectively. Median duration of response was NR for TN pts and 45 m for R/R pts. Pts estimated to be alive at 60 m were: TN, 92%; all R/R, 57%; R/R del17p, 32%; R/R del 11q, 61%; R/R unmutated IGVH, 55%. Among all treated pts, onset of grade ≥3 treatment-emergent AEs was highest in the first year and decreased during subsequent years. With about 5 years of follow-up, the most frequent grade ≥3 AEs were hypertension (26%), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%). Study treatment was discontinued due to AEs in 27 pts (20%) and disease progression in 34 pts (26%). Of all treated pts, 38% remain on ibr treatment on study including 65% of TN pts and 30% of R/R pts.
Conclusions: Single-agent ibrutinib continues to show durable responses in pts with TN or R/R CLL/SLL including those with del17p, del11q, or unmutated IGVH. With extended treatment, CRs were observed in 29% of TN and 10% of R/R pts, having evolved over time. Ibrutinib provided better PFS outcomes if administered earlier in therapy than in the third-line or beyond. Those without CK experienced more favorable PFS and OS than those with CK. Ibrutinib was well tolerated with the onset of AEs decreasing over time, allowing for extended dosing for 65% of TN and 30% of R/R pts who continue treatment.
- O’Brien S.M. et al. Five-Year Experience with Single-Agent Ibrutinib in Patients with Previously Untreated and Relapsed/Refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Leukemia. Oral Abstract #233: ASH 58th Annual Meeting and Exposition, San Diego, CA.

Understanding your specialty helps us to deliver the most relevant and engaging content.
Please spare a moment to share yours.
Please select or type your specialty
 Thank you
Thank youRelated articles
Newsletter
Subscribe to get the best content related to lymphoma & CLL delivered to your inbox