All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub uses cookies on this website. They help us give you the best online experience. By continuing to use our website without changing your cookie settings, you agree to our use of cookies in accordance with our updated Cookie Policy
Introducing

Now you can personalise
your Lymphoma Hub experience!
Bookmark content to read later
Select your specific areas of interest
View content recommended for you
Find out moreThe Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.









EHA-SWG 2017 | Rare Lymphomas: Biology of WM
Bookmark this article
On March 11th, at the EHA-SWG Rare Lymphomas Scientific Meeting 2017 in Barcelona, Spain, Marie José Kersten chaired a scientific session on ‘Waldenström’s Macroglobulinemia’. The first presentation of this session was by Roger Owen, from the St. James’s Institute of Oncology, Leeds, UK, on the topic of ‘Biology of WM’. Below are the key highlights from this presentation:
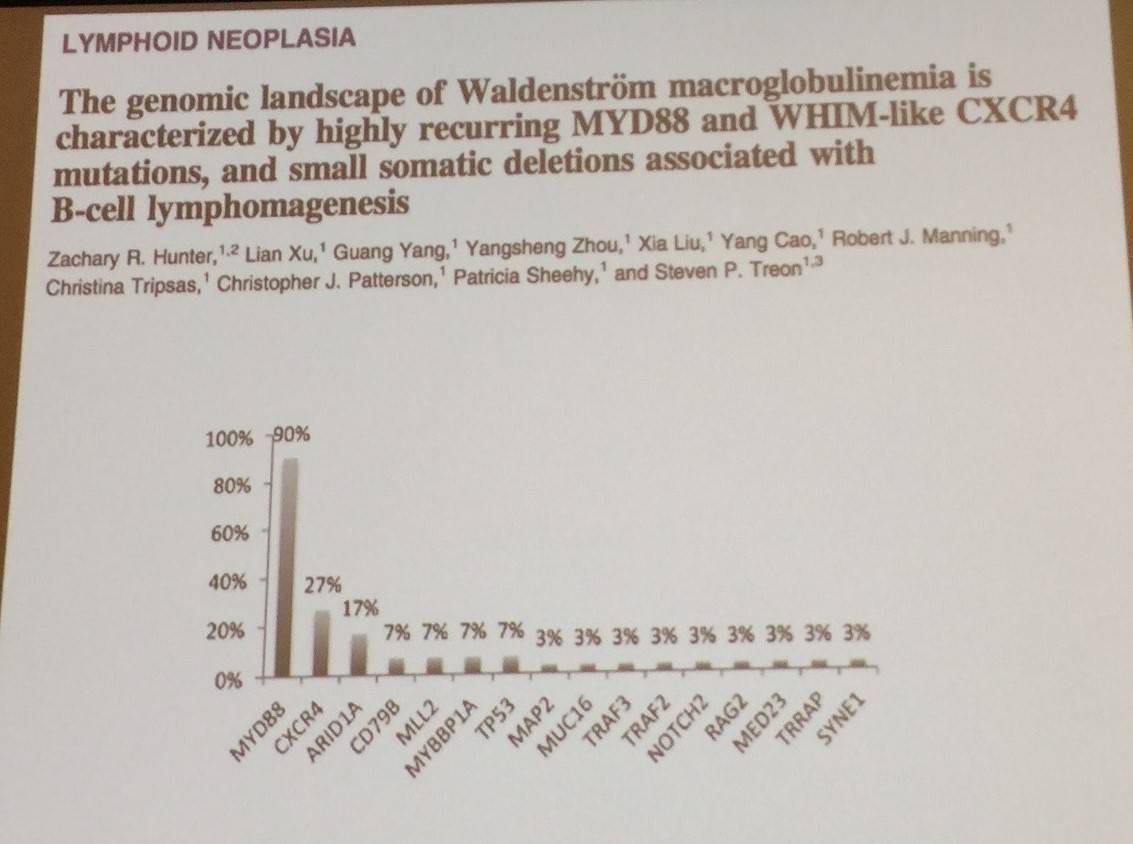
- WM patients frequently have mutations in key genes such as MYD88 and CXCR4
- MYD88
- MYD88 L265P mutation was identified in 91% of WM patients initially
- Not all WM patients have the MYD88 L265P mutation
- MYD88 L265P mutation results in activation of IRAK and BTK, leading to NFkB signaling and tumor cell growth
- Other mutations have been found to be recurring within WM patients e.g. CXCR4, ARID1A, etc. suggesting subclonal mutations within WM patients
- CXCR4
- CXCR4 mutations in ~30–40% WM pts with MYD88 mutation
- C-terminus of CXCR4 ligates with SDF1a (CXCL12) and is involved in signaling
- Nonsense and frame-shift mutations in CXCR4 are similar to those seen in WHIM syndrome
- CXCR4 mutations also present in ~33% of IgM monoclonal gammopathy of undetermined significance (MGUS)
- Both MYDS88 and CXCR4 are markers of poor clinical prognosis in WM
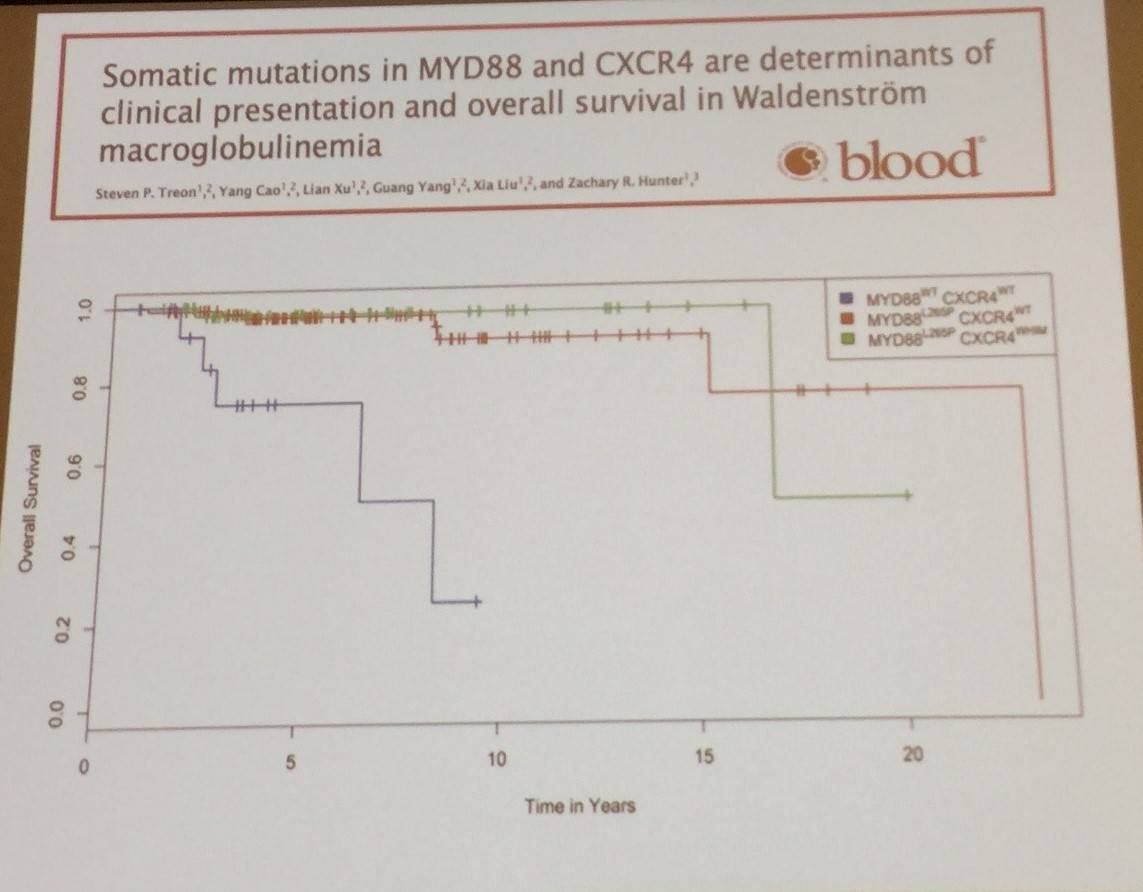
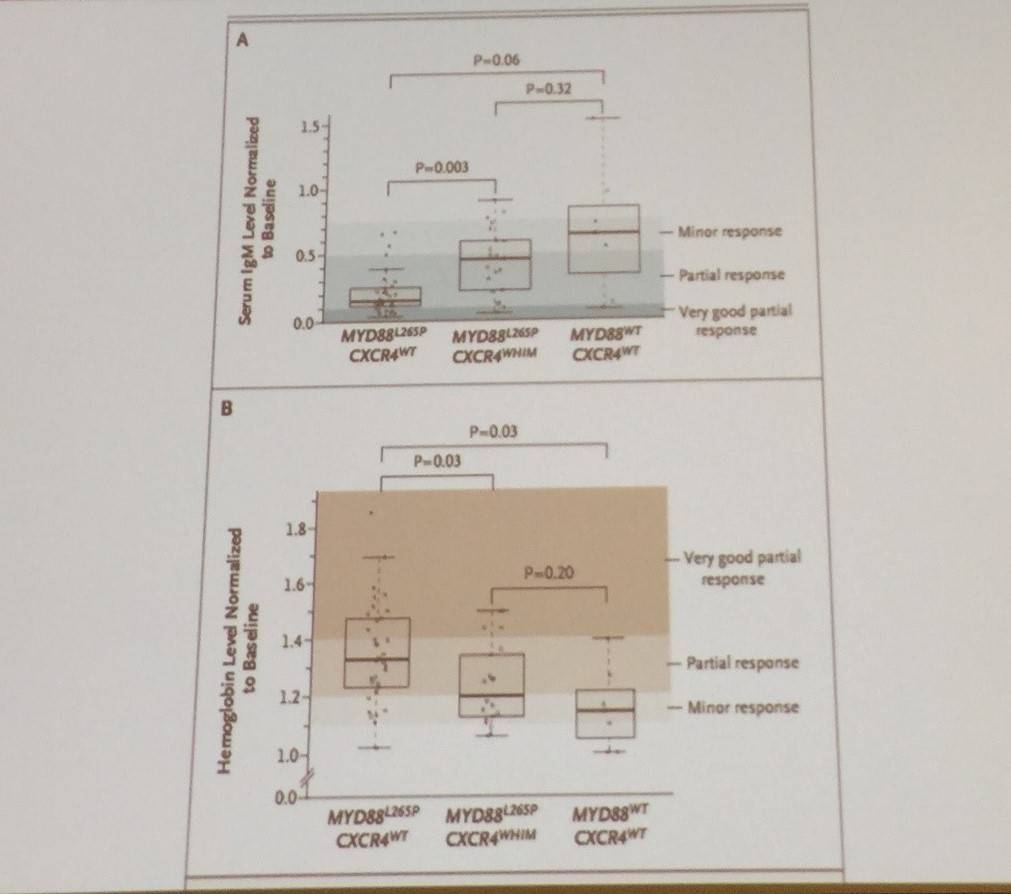
- WT MYD88 L265P pts have lower IgM and a poorer response to ibrutinib
- Other MYD88 mutations include BTKCys481 mutations, associated with ibrutinib resistance and CXCR4 mutations in WM
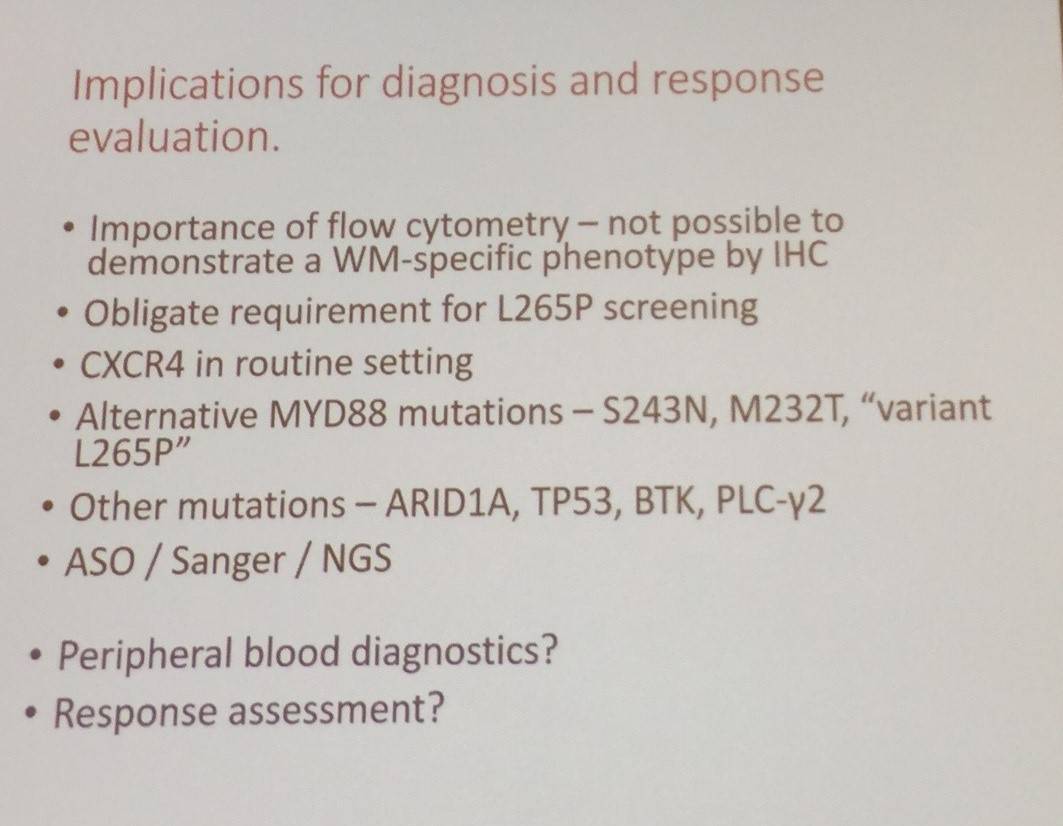
- WM B-cells have been shown to have a specific immunophenotype
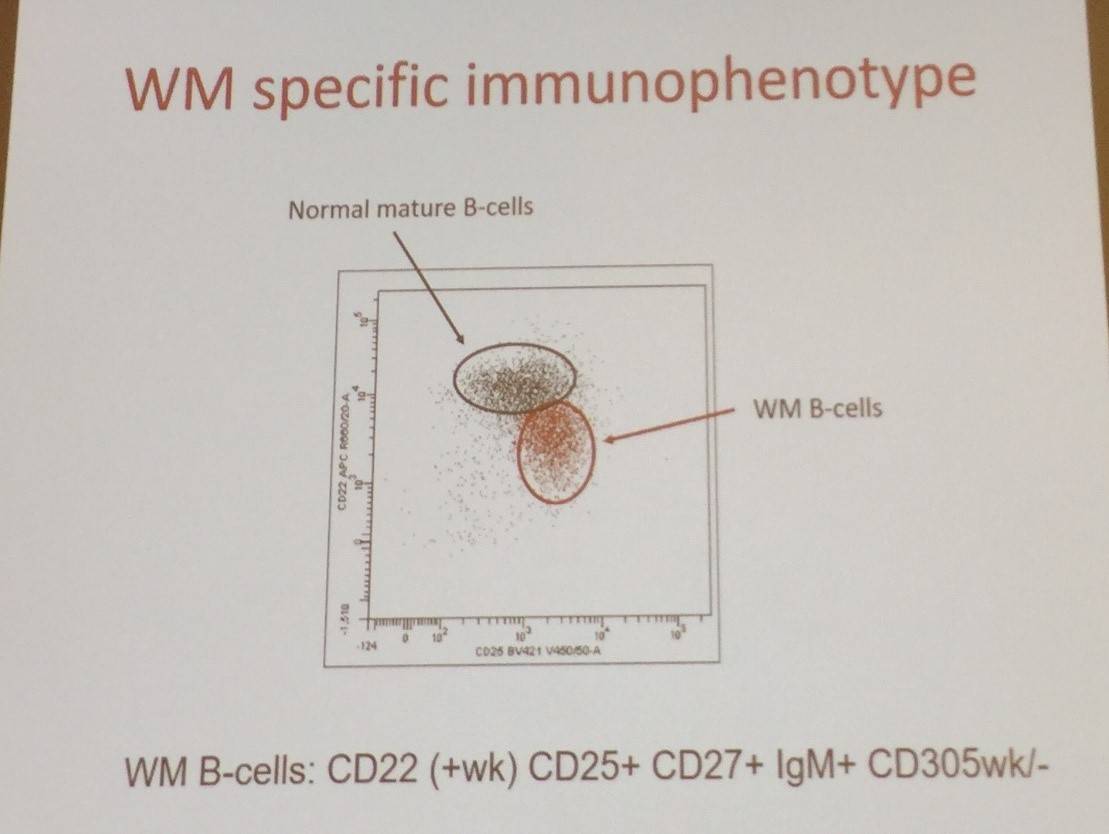
- Conclusions included the importance of flow cytometry to define WM, and the role of MYD88 point mutation screening
- Owen R. Biology of WM. 2017 Mar 11. EHA-SWG Rare Lymphomas. Barcelona, Spain.

Understanding your specialty helps us to deliver the most relevant and engaging content.
Please spare a moment to share yours.
Please select or type your specialty
 Thank you
Thank youRelated articles
Newsletter
Subscribe to get the best content related to lymphoma & CLL delivered to your inbox