All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
AACR 2017 | ZUMA-1 trial: immune signatures of CRS and neurologic events in subjects with refractory Diffuse Large B-Cell Lymphoma treated with KTE-C19
On Sunday 2nd April, during the “CTSY02 - Immuno-oncology Biomarkers in Clinical Trials” session, Frederick L. Locke, MD, of the H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, gave a talk titled “Immune signatures of cytokine release syndrome and neurologic events in a multicenter registrational trial (ZUMA-1) in subjects with refractory diffuse large B-cell lymphoma treated with axicabtagene ciloleucel (KTE-C19).”
Dr. Locke began the talk by explaining what Cytokine Release Syndrome (CRS) and neurologic events are. They are two potentially serious AEs that are associated with treatment with Chimeric Antigen Receptor (CAR) T-cells. CRS is mediated by high levels of IL-6 and other inflammatory cytokines, and symptoms include hypoxia, hypotension, tachycardia, and fever. Neurologic events are linked to high levels of cytokines or CAR T-cells, and symptoms include seizures, aphasia, tremor, encephalopathy, and confusion. The anti-IL-6 receptor antagonist, tocilizumab, and/or corticosteroids to suppress the immune system are used to manage neurologic events and CRS.
Following this, a brief overview of the ZUMA-1 prospective biomarker analysis, based on 101 treated patients, was given:
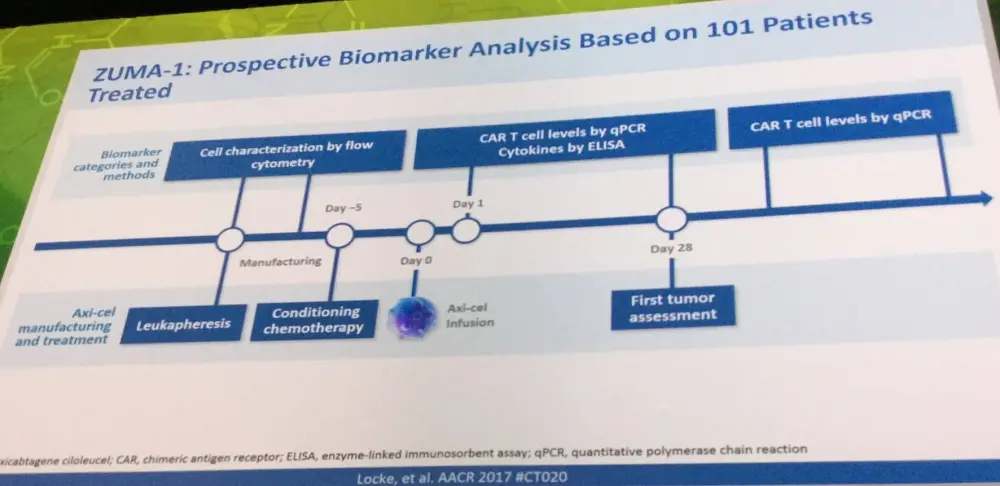
The manufacturing success rate of axi-cel was 99%, despite heterogeneity in starting apheresis material (14% naïve, 15% effector, 27% central memory, and 38% effector memory).
Dr. Locke went on to state that levels of CAR T-cells were reported to peak within 7–14 days of treatment with Axi-cel. It was also reported that CAR T-cell expansion is associated with objective response (P = 0.0002) as well as ≥grade 3 neurologic events (P = 0.0028).
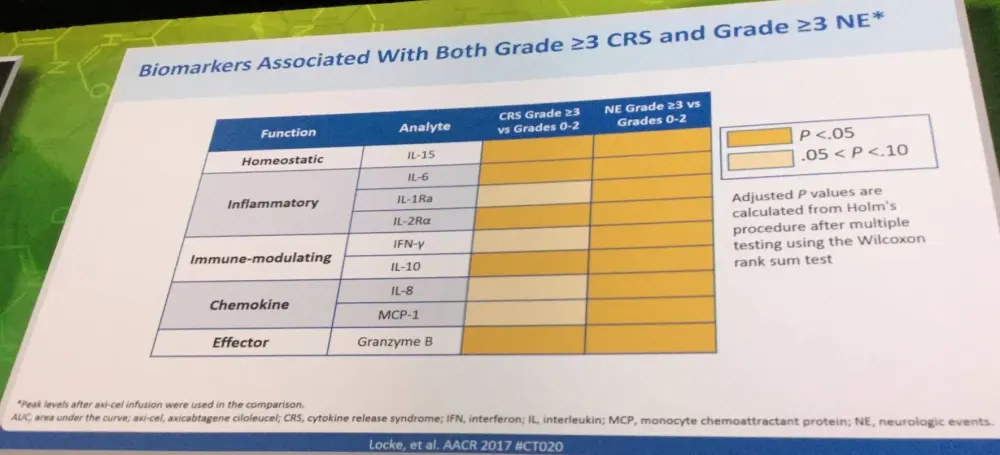
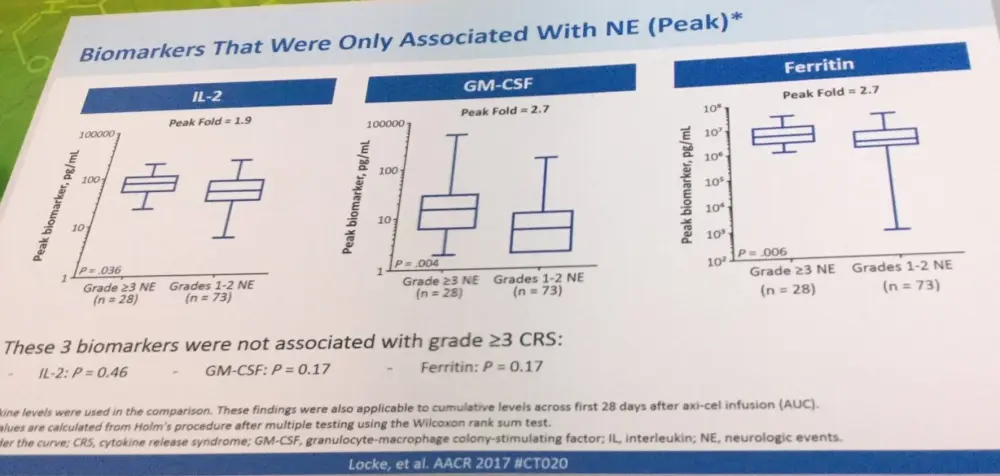
Distinct biomarkers also peaked within 7 days of treatment with Axi-cel. Analytes were elevated in ≥50% of patients with ≥2-fold induction above baseline out of a panel of 44 measured. Biomarkers found to associate with ≥grade 3 CRS and neurologic events included, but were not limited to, IL-15, IL-10, and granzyme B. However, IL-2, GM-CSF, and ferritin were found to only associate with neurologic events.
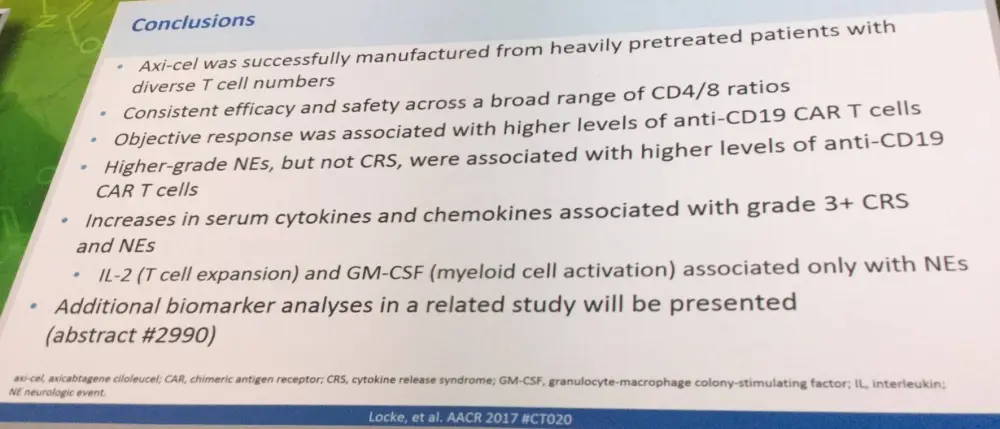
Dr. Locke concluded the talk with a concise summary slide:
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?