All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Beacoppescalated Followed By Radiotherapy of Initial Bulk or Residual Disease in Advanced Stage Hodgkin Lymphoma: Long-Term Follow up of the HD9 and HD12 Trials of the German Hodgkin Study Group
The 58th Annual Meeting & Exposition of the American Society of Hematology’s (ASH) took place in San Diego, CA, and on December 5th, Bastian von Tresckow, MD, from the Department of Internal Medicine and German Hodgkin Study Group (GHSG), University Hospital of Cologne, Germany, presented data from the long-term follow up with patients from the HD9 and HD12 trials into BEACOPPescalated treatment followed by radiotherapy (RT) in patients with newly diagnosed advanced Hodgkin Lymphoma (HL). Their goal was to record the long-term safety of this therapy, and the necessity of RT following BEACOPPescalated.
Highlights:
- 1,282 pts treated as part of HD9, 1670 pts treated as part of HD12
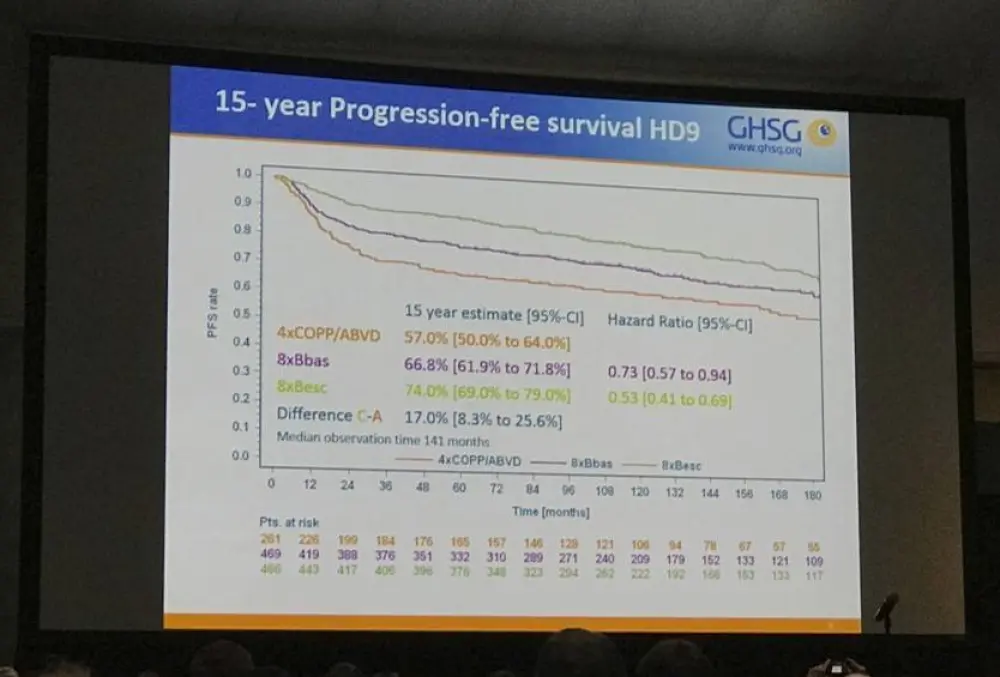
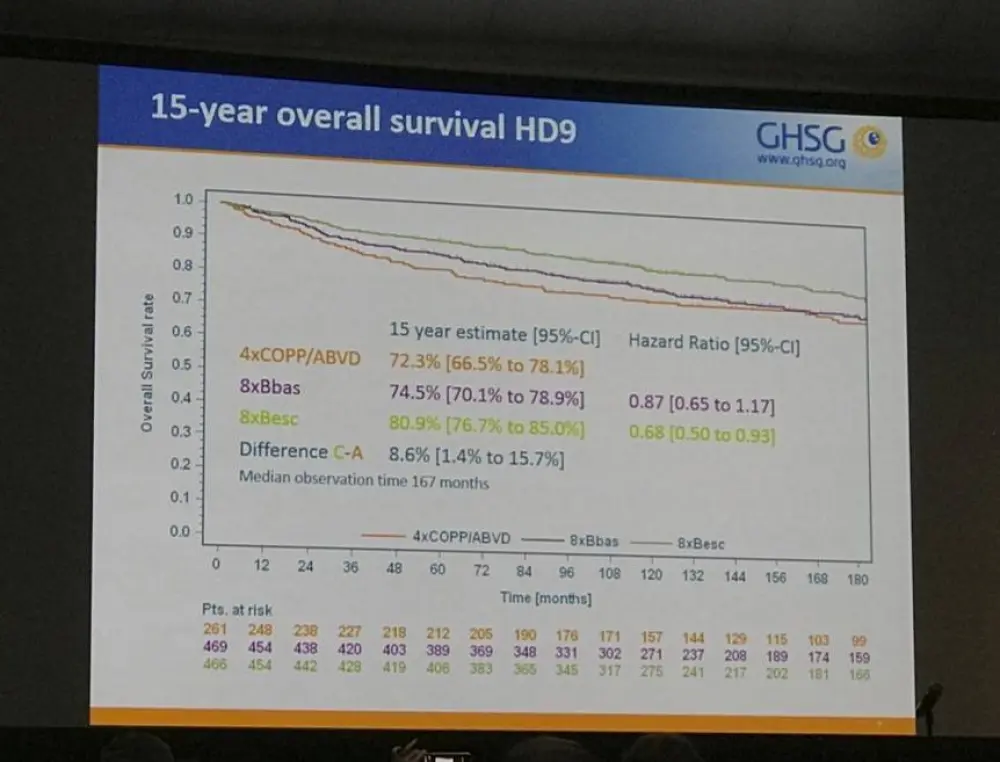
- HD9 results- 15-year Progression Free Survival (PFS) and Overall Survival (OS):
- COPP/ABVD = 57% (OS =72.3%)
- BEACOPPbaseline = 66.8% (OS =74.5%)
- BEACOPPescalated = 74% (OS =80.9%)
- HD12 results:
- No difference in OS or PFS between 8 cycles BEACOPPescalated or 4+4 group (4 cycles BEACOPPescalated, 4 cycles BEACOPPbaseline)
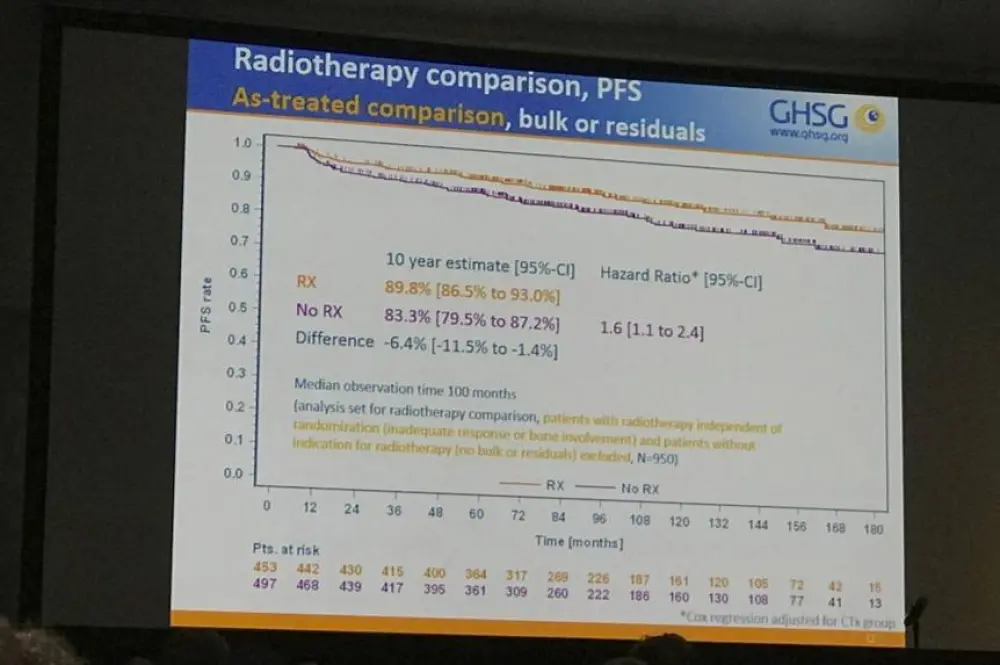
- 1% pts with bulk or residual disease randomized to either +RT or no RT
- No RT group had significantly lower PFS at 10 year follow up than +RT group (83.3% vs 89.8%)
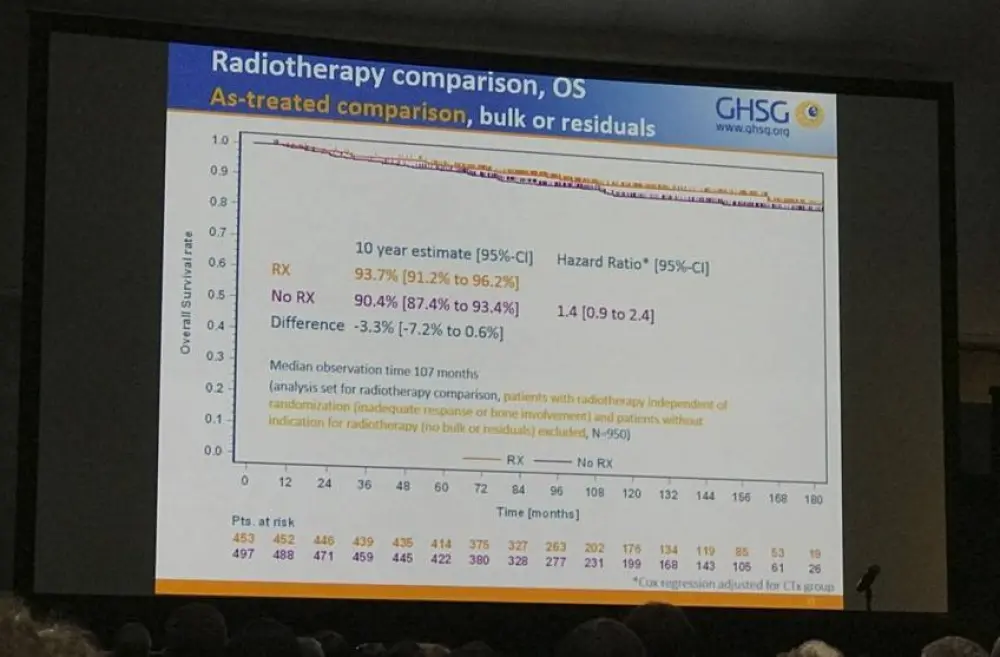
- Trend to lower OS in no RT vs +RT group (90.4% vs 93.7%)
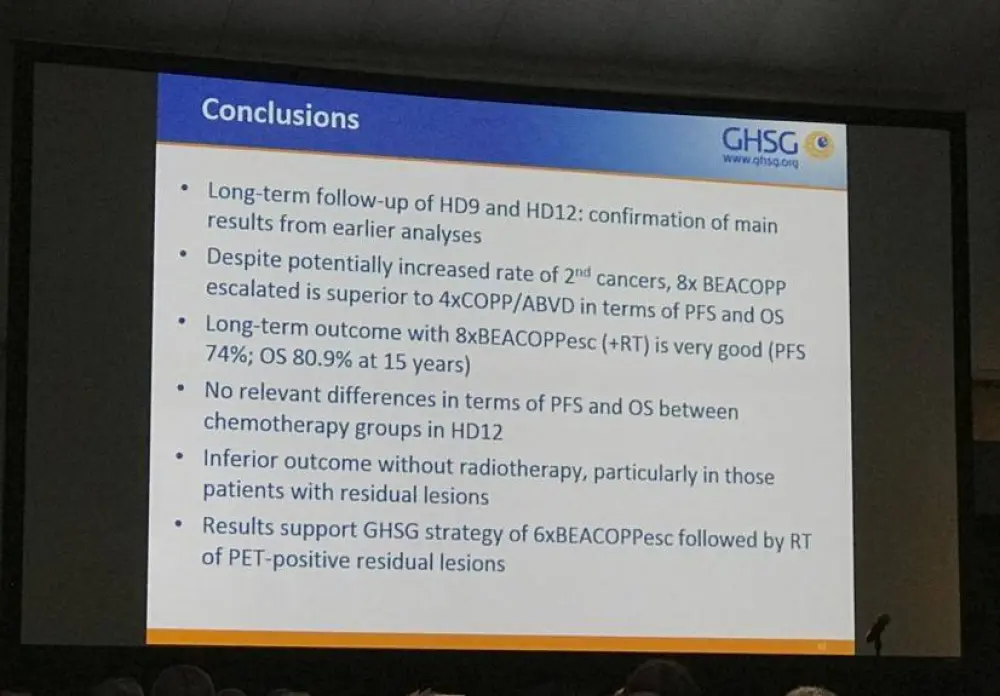
Bastian von Tresckow concluded that intensive first-line treatment, such as BECAOPPescalated, increases the 15 year OS and PFS of newly diagnosed advanced HL patients, and that consolidating RT provides a benefit to 10 year OS and PFS.
Abstract:
Background: The HD9 trial established 8 cycles of BEACOPPescalated followed by radiotherapy (RT) of initial bulk or residual tumors as German Hodgkin Study Group (GHSG) standard of care for advanced stage Hodgkin Lymphoma (HL) at that time. The succeeding HD12 trial aimed at reducing treatment intensity while maintaining efficacy. It compared 8 cycles of BEACOPPescalated with 4 cycles of BEACOPPescalated followed by 4 cycles of BEACOPPbaseline (“4+4” regimen) as well as RT with no RT of initial bulk or residual disease. Although tumor control is outstanding, long-term safety of BEACOPPescalated still is a matter of concern, and the need of consolidating RT in advanced stage HL is discussed controversially. We therefore performed a long-term follow up of the HD9 and HD12 trials in order to address these open questions.
Patients and Methods: Between February 1993 and March 1998, 1,282 patients in the HD9 trial were treated with either 8 cycles of COPP/ABVD, 8 cycles of BEACOPPbaseline, or 8 cycles of BEACOPPescalated. Between January 1999 and January 2003, 1,670 HD12 patients were randomized for two questions in a factorial design: first, for 8 cycles of BEACOPPescalated or “4+4”, and second for consolidation RT or no RT to regions of initial bulk or residual disease. Patients with inadequate response or skeletal involvement were irradiated irrespective of randomized RT group based on the recommendation of a central diagnostic panel blinded to treatment groups.
Results: In HD9-patients treated with COPP/ABVD, BEACOPPbaseline, and BEACOPPescalated, the 15-year progression-free survival (PFS) was 57%, 66.8%, and 74% with overall survival (OS) rates of 72.3%, 74.5%, and 80.9%, respectively. BEACOPPescalated remains significantly better than COPP/ABVD in terms of PFS (difference 17.0%; 95%-CI 8.3% to 25.6%) and OS (difference 8.6%; 95%-CI 1.4% to 15.7%) with consistent effects in subgroups by gender, IPS and ages up to 60 years. A total of 123 second malignancies corresponding to 15-year cumulative secondary malignancy incidences of 7.2%, 13%, and 11.4% were reported for COPP/ABVD, BEACOPPbaseline, and BEACOPPescalated, respectively, without a difference between COPP/ABVD and BEACOPPescalated (p=0.5). Standardized incidence ratios (SIR) with 95%-CI showed elevation compared to the general German population in all groups: 2.0 [1.2 to 3.2], 2.6 [1.9 to 3.4] and 2.6 [1.9 to 3.4]. Regarding HD12, the 10-year PFS and OS rates in the two chemotherapy groups were not significantly different with 82.6% and 87.3% in the BEACOPPescalated group and 80.6% and 86.8% in the 4+4 group, respectively. After chemotherapy, 153 of 1,481 (10.3%) patients with complete information had an RT recommendation irrespective of group and 378 (25.5%) had neither bulk nor residual disease. Amongst the remaining 950 patients (64.1%) with bulk or residual disease, patients randomized to no RT showed a significantly inferior 10-year PFS of 83.5% compared to patients in the RT group (88.6%, difference -5.1%; 95%-CI,-9.9% to -0.4%, hazard ratio [HR] 1.47) and a trend towards inferior OS in no RT patients (RT 93%; no RT 90.2%; difference -2.7%; 95%-CI,-6.5% to 1%). Patients with residual lesions without RT had both an inferior PFS and OS as compared to patients with RT (as treated comparison: 10-year PFS RT 89.7%; no RT 83.4%; difference -6.3%; 95%-CI,-12.8% to -0.1%; 10-year OS RT 94.4%; no RT 88.4%; difference -6%; 95%-CI,-11.4% to -0.5%). 10-year cumulative incidence of second malignancies ranged between 6.4% (4+4) and 9.7% (BEACOPPescalated+RT) without a significant difference between pooled chemo- or radiotherapy groups.
Conclusions: These long-term follow-up observations indicate an ongoing benefit of an intensive first-line therapy strategy for the PFS and OS of patients with newly diagnosed advanced stage HL. The observed OS benefit suggests an important role of consolidating RT for patients with newly diagnosed advanced stage HL. The OS benefit does not seem to be relevantly compromised by the incidence of second malignancies.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?