All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Caribou Biosciences, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Chemotherapy-Free Induction with Ibrutinib-Rituximab Followed By Shortened Cycles of Chemo-Immunotherapy Consolidation in Young, Newly Diagnosed Mantle Cell Lymphoma Patients: A Phase II Clinical Trial
The 58th Annual Meeting & Exposition of the American Society of Hematology’s (ASH) took place in San Diego, CA, and on December 3rd, Professor Michael Wang, MD, from the University of Texas MD Anderson Cancer Center, presented the results of a Phase-II trial on ibrutinib-rituximab followed by short cycles of chemo-immunotherapy consolidation in newly diagnosed young MCL patients.
Their goal was to assess the efficacy of ibrutinib-rituximab (IR) in patients with newly diagnosed MCL, in a single center trial of chemotherapy-free initial therapy with IR, and after best response was achieved they were treated with short course chemo-immunotherapy.
Highlights:
- Recruited 50 newly diagnosed untreated MCL pts ≤65 yr
- Part 1 = 36 response evaluable patients – Part 1+2 = 19 response evaluable patients
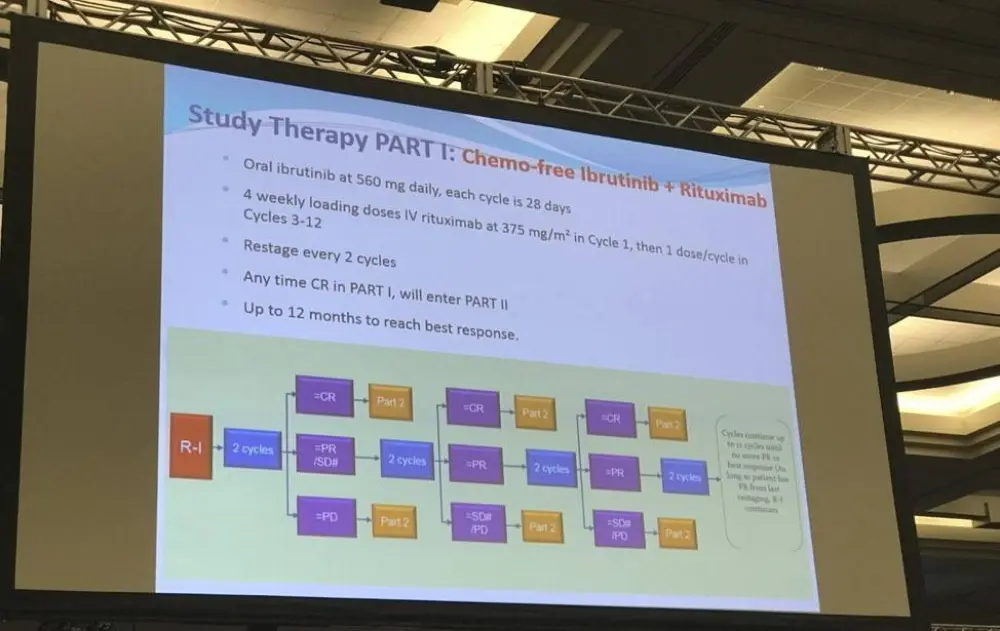
- Part 1 dose: Ibrutinib = 560mg/day, Rituximab = 375mg/m2 IV four times weekly for first cycle (28 days), then on day one of the third to twelfth cycle
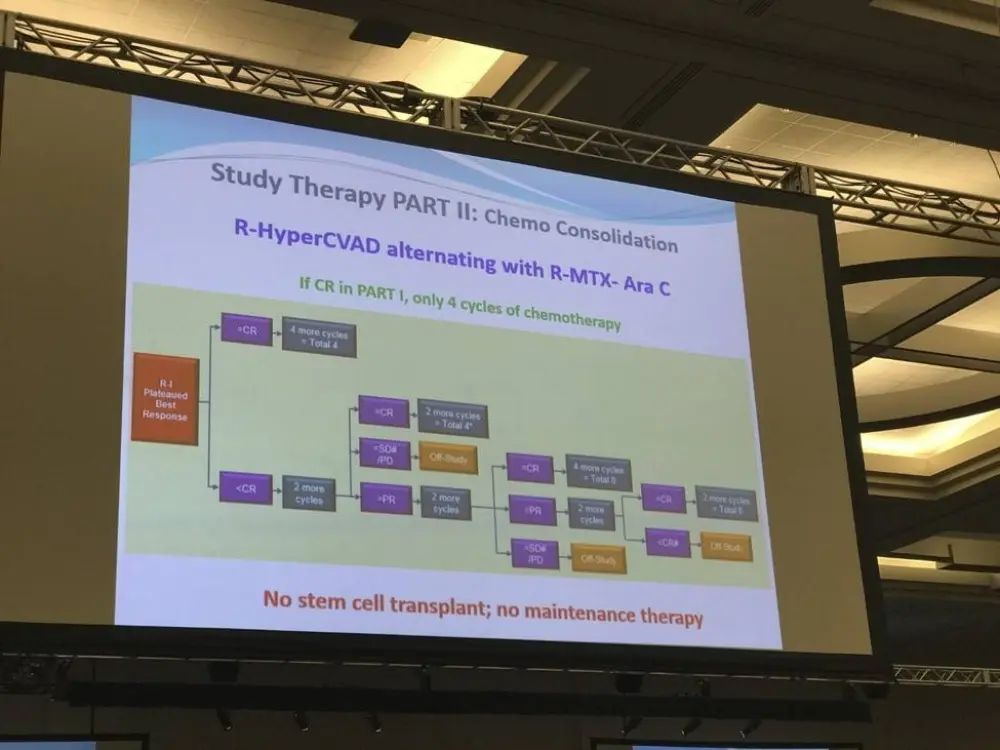
- Part 2 chemo-immunotherapy dose: rituximab + hyper-CVAD, alternating every 28 days with rituximab + high-dose methotrexate Ara C
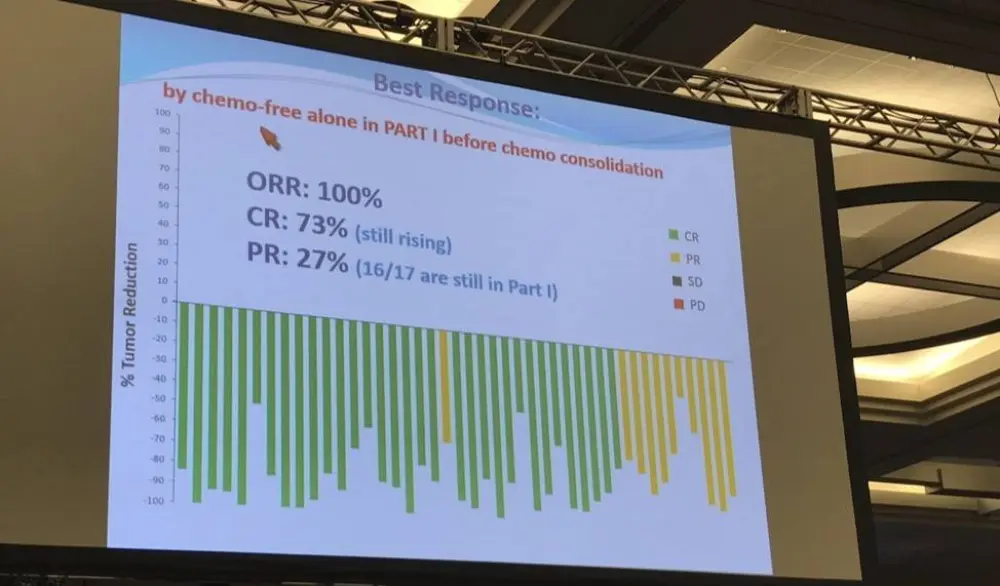
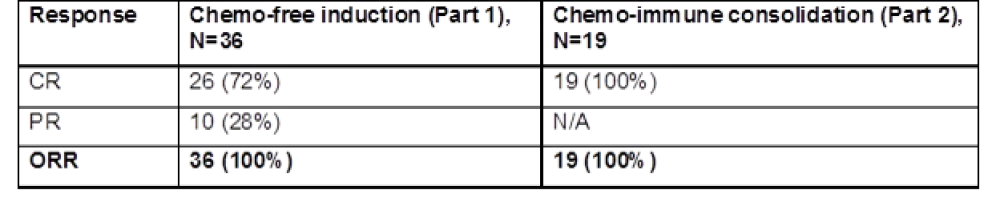
- Part 1: ORR = 100%, PR = 27%, CR = 73%
- Part 2: ORR = 100%, CR = 100%
The study reported a high number of grade 1-2 non-hematological AEs in patients, and grade 3 fatigue (n=3) and rash (n=1) in treatment part 1 with no grade 4 or 5. In treatment part 2, grade 1-2 hematological AEs were anemia (n=13), with four instances of grade 3-4 hematological AEs and no grade 5 AEs. However, data from a longer follow-up period is needed.
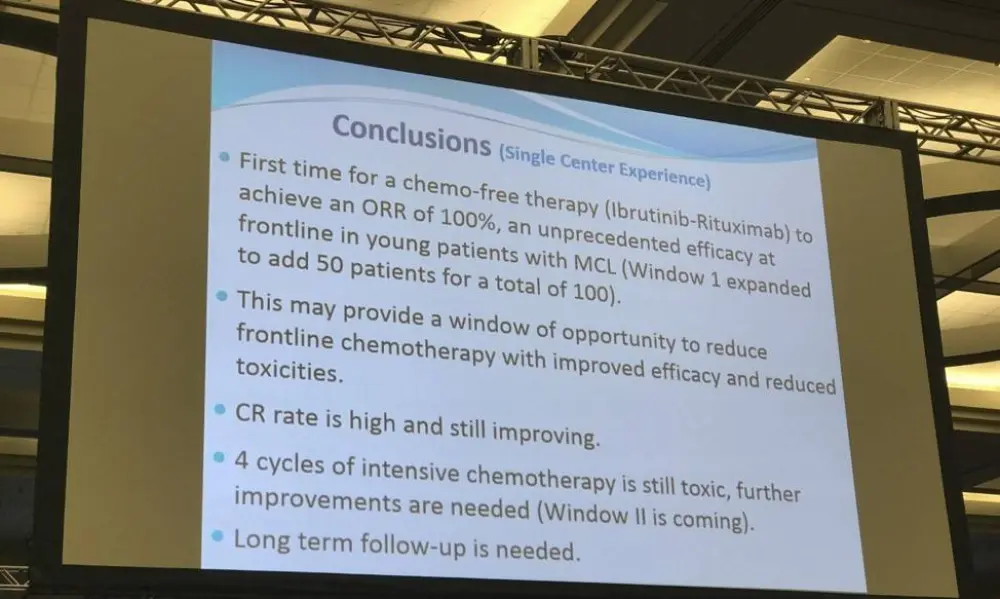
Michael Wang concluded that this study’s preliminary data indicated that their treatment part 1 consisting of chemo-free IR was well-tolerated and effective, potentially providing a new way of treating MCL in young, newly diagnosed patients utilizing less chemo-immunotherapy.
Abstract:
Introduction: Mantle cell lymphoma (MCL) is a rare and incurable subtype of B-cell lymphoma. Intense chemo-immunotherapy with 8 cycles of Rituximab-HyperCVAD alternating with Rituximab-Methotrexate-Ara C is associated with an overall survival of 10.7 years but the 10-year cumulative incidence of therapy-related myeloid neoplasm was 6.2%. The ibrutinib–rituximab combination has produced durable responses in 88% of patients with relapsed and refractory MCL with acceptable toxicity. This gives rise to a “Window” of opportunity to use chemotherapy-free induction with ibrutinib plus rituximab followed by fewer cycles of chemo-immunotherapy consolidation in young and fit patients with newly-diagnosed, untreated MCL.
Methods: Enrolment began in June 2015 for a Phase II single-center clinical trial consisting of an initial chemotherapy-free phase (window) of ibrutinib and rituximab combination treatment in Part 1 until best response, followed by a shortened course of intense chemo-immunotherapy in Part 2 among young newly diagnosed MCL patients of ≤65 years. The primary objective was to evaluate the response rate of ibrutinib plus rituximab. The secondary objectives were to evaluate the progression free survival (PFS) of ibrutinib plus rituximab after consolidation with a shortened number of cycles of intense chemo-immunotherapy, and to further evaluate the toxicity profile. Ibrutinib is dosed at 560 mg orally, daily, continuously. Rituximab is dosed at 375 mg/m2 IV weekly x 4 during cycle 1 (28 days cycle), then day 1 of cycles 3-12. Intense chemo-immunotherapy consists of rituximab plus cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD); alternating every 28 days with rituximab plus high-dose methotrexate-Ara C. If in complete remission (CR) after initial ibrutinib and rituximab treatment, a total of 4 additional treatments of intense chemo-immunotherapy are given. If the patient is in partial response or progression, and if responding to intensive chemo-immunotherapy, a total of 2 cycles of chemo-immunotherapy therapy are administered beyond achievement of CR.
Results: As of August 2, 2016, we have completed the target enrolment by accruing 50 out 50 patients with newly-diagnosed untreated MCL. Forty one (n=41) patients have begun treatment and 36 are evaluable for response. Of the 36 evaluable patients, overall response rate (ORR) to Part 1 alone (Ibrutinib plus rituximab) is 100% (n=36) with PR in 28% (n=10) and CR in 72% (n=20). Nineteen 19 patients have completed both Part 1 (ibrutinib and rituximab) and Part 2 (chemo-immunotherapy). The ORR to both Part 1 and Part 2 (n=19) was 100% and was equal to the CR rate (100%, n=19), i.e. all have achieved a CR to Part 1 and Part 2. Toxicities are recorded as the number of patients experiencing a certain adverse event. Regardless of their relation to study drug in Part 1, the most common grade 1-2 non-haematological (non-heme) adverse effects (AEs) are fatigue (n=40), diarrhea (n=25), rash (n=24), myalgia (n=22), oral mucositis (n=17), peripheral neuropathy (n=15), nausea (n=14), blurred vision (n=14), edema (n=13), constipation (n=12), headache (n=11), dry eyes (n=9), dizziness (n=9) and watery eyes (n=6). Grade 3 non-heme AEs included fatigue (n=3), nausea (n=0), rash (n=1), pleural effusion (n=1), infection (n=2) and dyspnea (n=1). There was no grade 4 or grade 5 non-heme toxicities in Part 1. In part 2, common grade 1-2 hematological (heme) AEs was anemia (n=13). Grade 3-4 haematological AEs included neutropenia (n=2), ALT increase (n=1) and febrile neutropenia (n=1). In Part 2, there was no grade 5 hematologic toxicity. The toxicity after intensive immune-chemotherapy in shortened cycles are much improved compared to historical controls but longer follow-up is needed.
Conclusions: Preliminary data indicate that the chemotherapy-free induction with ibrutinib and rituximab in newly diagnosed, young MCL patients was efficacious and well-tolerated. This unprecedented efficacy and safety may provide a window of opportunity for less chemo-immunotherapy needed for consolidation.
Table 1: Preliminary findings form the Window Study: a phase II clinical trial
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?