All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Final results of the phase III study of obinutuzumab or R-CHOP in DLBCL
The 58th Annual Meeting & Exposition of the American Society of Hematology (ASH) took place in San Diego, CA, on December 3–6, 2016. On Sunday 4th December, an oral abstract session was held between 4:30pm and 6:00pm in the “Aggressive Lymphoma (Diffuse Large B-Cell and other aggressive B-Cell Non-Hodgkin Lymphomas) – results from prospective clinical trials: Novel Approaches in Aggressive Lymphoma” category. This session was moderated by Jason R. Westin, MD MS, of The University of Texas MD Anderson Cancer Center, and Laurie H Sehn, MD, of the British Columbia Cancer Agency.
Abstract #470 was presented during this session, titled “Obinutuzumab or Rituximab Plus CHOP in Patients with Previously Untreated Diffuse Large B-Cell Lymphoma: Final Results from an Open-Label, Randomized Phase 3 Study (GOYA)” by Umberto Vitolo, of the Azienda Ospedaliera Universitaria Città della Salute e della Scienza di Torino, Italy, and colleagues.
The group conducted an open-label, multicenter study, GOYA (NCT012887741), to compare the efficacy and safety of obinutuzumab (G) in combination with CHOP (G-CHOP) versus rituximab in combination with CHOP (R-CHOP) in patients with previously untreated Diffuse Large B- Cell Lymphoma (DLBCL). Investigator (INV) assessed Progression Free Survival (PFS) was the primary endpoint of the study. PFS assessed by Independent Review Committee (IRC), Overall Survival (OS), Overall Response Rate (ORR) and safety were the secondary endpoints. Enrolled patients had a median age of 62 years (43–78). Current results are:
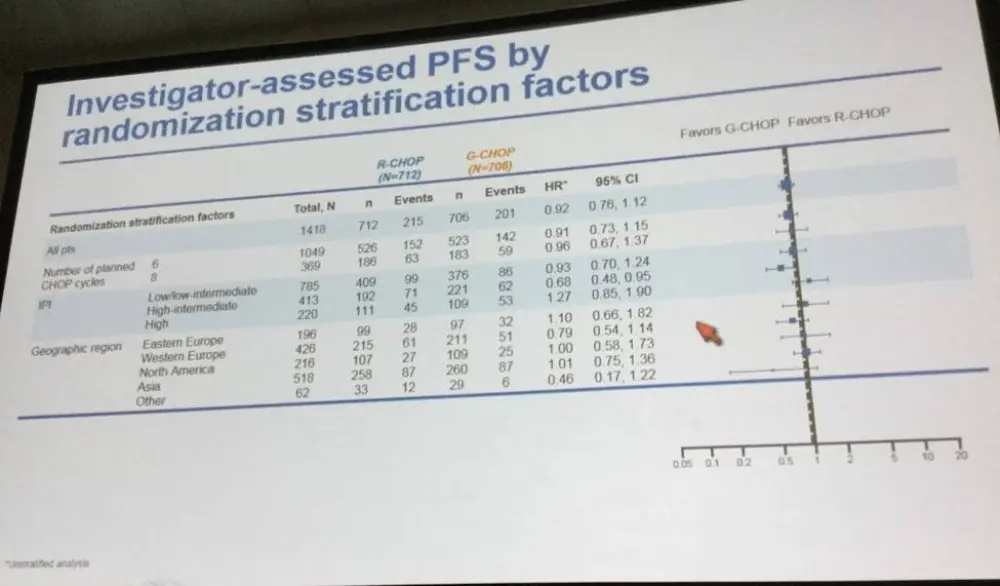
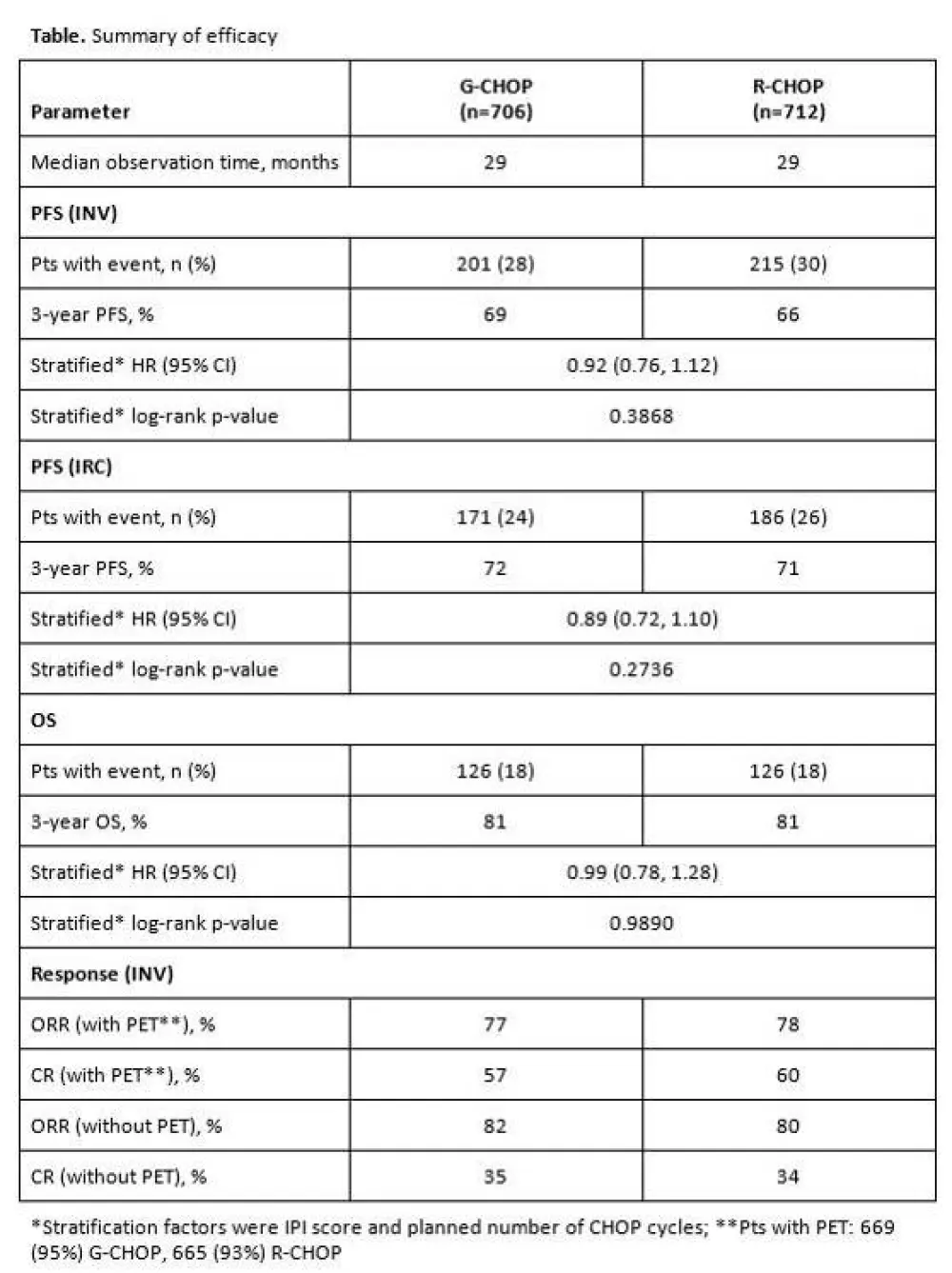
- No significant difference in INV-assessed PFS between G-CHOP and R-CHOP ( 3-year PFS, 69% vs 66%, stratified HR = 0.92, P = 0.3868)
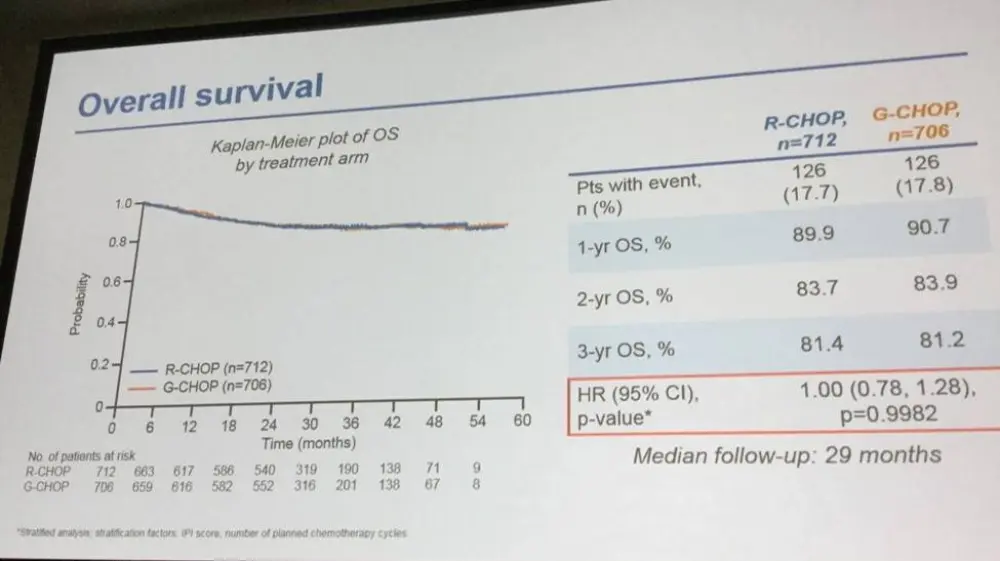
- PFS by IRC, OS and ORR were similar between G-CHOP and R-CHOP (Table)
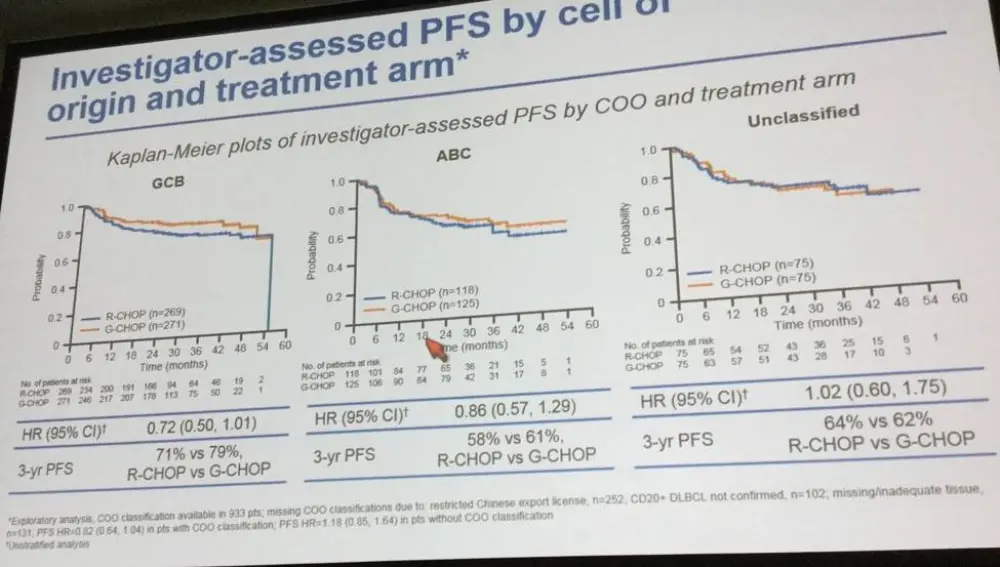
- In GCB DLBCL subgroups, INV-assessed PFS, stratified HR of 0.72 was in favor of G-CHOP over R-CHOP (3-year PFS, 79% vs 71%)
- Grade ≥ 3 AEs (74% vs 65%) and serious AEs ( 43% vs 38%) were more common in the G-CHOP arm than in the R-CHOP arm
- Most frequent ≥ 3 AEs in G-CHOP compared to R-CHOP = neutropenia (57% vs 44%), thrombocytopenia (8% vs 3%), infusion-related reactions (45% vs 32%), and infections (54% vs 44%)
- AEs with fatal outcome were slightly more common with G-CHOP (6% [42/704]) compared to R-CHOP (4% [30/704])
- Common AEs leading to death were pneumonia (5 G-CHOP; 6 R-CHOP) and sepsis/septic shock (7 G-CHOP; 3 R-CHOP).
The presentation was concluded by highlighting that the primary endpoint of the study was not met. Compared with R-CHOP, G-CHOP did not significantly improve INV-assessed PFS in previously untreated DLBCL patients. Additionally, no unexpected safety concerns were identified. Investigations into outcomes in subgroups of DLBCL is planned.
Abstract
Background: Rituximab (R) plus CHOP (R-CHOP) is standard-of-care treatment for previously untreated diffuse large B-cell lymphoma (DLBCL). Approximately 35–40% of patients (pts) will relapse following R-CHOP, and outcomes with salvage therapy remain poor. Obinutuzumab (GA101; GAZYVA/GAZYVARO; G) is a glycoengineered, type II anti-CD20 monoclonal antibody with greater direct cell death induction and antibody-dependent cellular cytotoxicity/phagocytosis activity than R. In the Phase 2 GATHER study (NCT01414855), G plus CHOP (G-CHOP) demonstrated manageable toxicity and promising efficacy in pts with advanced untreated DLBCL. GOYA (NCT01287741) is an open-label, multicenter, randomized Phase 3 study comparing the efficacy and safety of G-CHOP with R-CHOP in pts with previously untreated DLBCL. GOYA was sponsored by Roche with scientific support from the Fondazione Italiana Linfomi.
Methods: Eligible pts were aged ≥18 years and had adequate hematologic function, ≥1 bi-dimensionally measurable lesion, an ECOG performance status (PS) of ≤2 and an International Prognostic Index (IPI) score of ≥2 (high, high-intermediate or low-intermediate risk). Low-risk pts with an IPI score of 1 (but not due to age alone) or with an IPI score of 0 with bulky disease (one lesion ≥7.5cm) were also eligible. Pts were randomized 1:1 to receive 8 (21-day) cycles of G (1000mg i.v. on Days [D] 1, 8, and 15, Cycle [C] 1 and D1, C2–8) or R (375mg/m2i.v. on D1, C1–8) in combination with 6 or 8 cycles of CHOP (number of cycles preplanned in advance for all pts at each site). Preplanned radiotherapy was allowed for bulky or extranodal disease. The primary endpoint was investigator (INV)-assessed progression-free survival (PFS); for the target hazard ratio (HR) of 0.75, the 3-year PFS was expected to improve from 60% to 68%. Secondary endpoints included: PFS assessed by Independent Review Committee (IRC); overall survival (OS); complete response (CR) and overall response rate (ORR) with or without PET (assessed by INV or IRC according to modified Cheson 2007 criteria); and safety.
Results: 1418 pts were randomized to study treatment: 706 to G-CHOP and 712 to R-CHOP. Baseline characteristics were well balanced between the G-CHOP and R-CHOP arms: mean age, 62.0 years in both arms; ECOG PS ≥2, 12% vs. 14%; IPI score ≥3, 47% vs. 43%; Ann Arbor stage III–IV, 76% in both arms. Cell-of-origin distribution, as assessed by gene-expression profiling (NanoString), was similar in both treatment groups (GCB: 58% [271/471] G-CHOP, 58% [269/462] R-CHOP; ABC: 27% [125/471] G-CHOP, 26% [118/462] R-CHOP; Unclassified: 15.9% [75/471] G-CHOP, 16.2% [75/462] R-CHOP). For the primary endpoint of INV-assessed PFS, there was no significant difference between G-CHOP and R-CHOP (3-year PFS, 69% vs. 66%; stratified HR, 0.92; 95% confidence interval [CI], 0.76, 1.12; p=0.3868; Table). Secondary endpoints, including PFS by IRC, OS, and end-of-treatment ORR/CR rate (with and without PET), were consistent with the primary endpoint, with no clinically meaningful differences observed between the treatment arms (Table). In a prespecified subgroup analysis of INV-assessed PFS, a stratified HR of 0.72 (95% CI, 0.50, 1.01) in favor of G-CHOP over R-CHOP was determined for pts with GCB DLBCL (3-year PFS, 79% vs. 70%). No new safety signals were identified. Grade ≥3 adverse events (AEs; 74% vs. 65%) and serious AEs (43% vs. 38%) were more common in the G-CHOP than in the R-CHOP arm. Grade ≥3 AEs of particular interest that were numerically more common with G-CHOP than R-CHOP included neutropenia (57% vs. 48%), infusion-related reactions (45% vs. 32%), infections (54% vs. 44%), and thrombocytopenia (8% vs. 3%). AEs resulting in withdrawal from treatment (12% [84/704] G-CHOP; 9% [60/703] R-CHOP) and AEs with fatal outcome (6% [41/704] G-CHOP; 4% [30/703] R-CHOP) were slightly more common with G-CHOP. The most common AEs leading to death were pneumonia (5 G-CHOP; 6 R-CHOP) and sepsis/septic shock (7 G-CHOP; 3 R-CHOP).
Conclusions: The primary endpoint of this study was not met: G-CHOP did not significantly improve INV-assessed PFS compared with R-CHOP in previously untreated pts with DLBCL. No unexpected safety signals were identified. Further investigation of outcomes in subgroups is planned.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?