All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Caribou Biosciences, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Results of phase III study of R-CHOP versus DA-EPOCH-R in untreated DLBCL
The 58th Annual Meeting & Exposition of the American Society of Hematology (ASH) took place in San Diego, CA, on December 3–6, 2016. On Sunday 4th December, an oral abstract session was held between 4:30pm and 6:00pm in the “Aggressive Lymphoma (Diffuse Large B-Cell and other aggressive B-Cell Non-Hodgkin Lymphomas) – results from prospective clinical trials: Novel Approaches in Aggressive Lymphoma” category. This session was moderated by Jason R. Westin, MD MS, from The University of Texas MD Anderson Cancer Center, and Laurie H Sehn, MD, of the British Columbia Cancer Agency.
Abstract #469 was the first abstract presented during this session, titled “Phase III randomized study of R-CHOP Versus DA-EPOCH-R and molecular analysis of untreated Diffuse Large B-Cell Lymphoma: CALGB/Alliance 50303” by Wyndham H. Wilson MD PhD, of the National Cancer Institute, Bethesda, Maryland, and colleagues.
R-CHOP has not been studied within Diffuse Large B-Cell Lymphoma (DLBCL) molecular subtypes. This group are conducting a phase III study, CALGB/ Alliance 50303 (NCT00118209), aimed at comparing the efficacy of R-CHOP and Dose Adjusted (DA)-EPOCH-R regimens in treating DLBCL patients, specifically in GCB and ABC subtypes. Event Free Survival (EFS) of R-CHOP versus DA-EPOCH-R and developing a molecular predictor of outcome based on GCB and ABC DLBCL were the primary endpoints of this study.
- Five-hundred and twenty-four patients were randomized to receive either R-CHOP (Arm A [n = 233]) or DA-EPOCH- R (Arm B [n = 231])
- At median follow up of 4.9 years; no difference in EFS in Arm A and Arm B (HR= 1.02, P = 0.89)
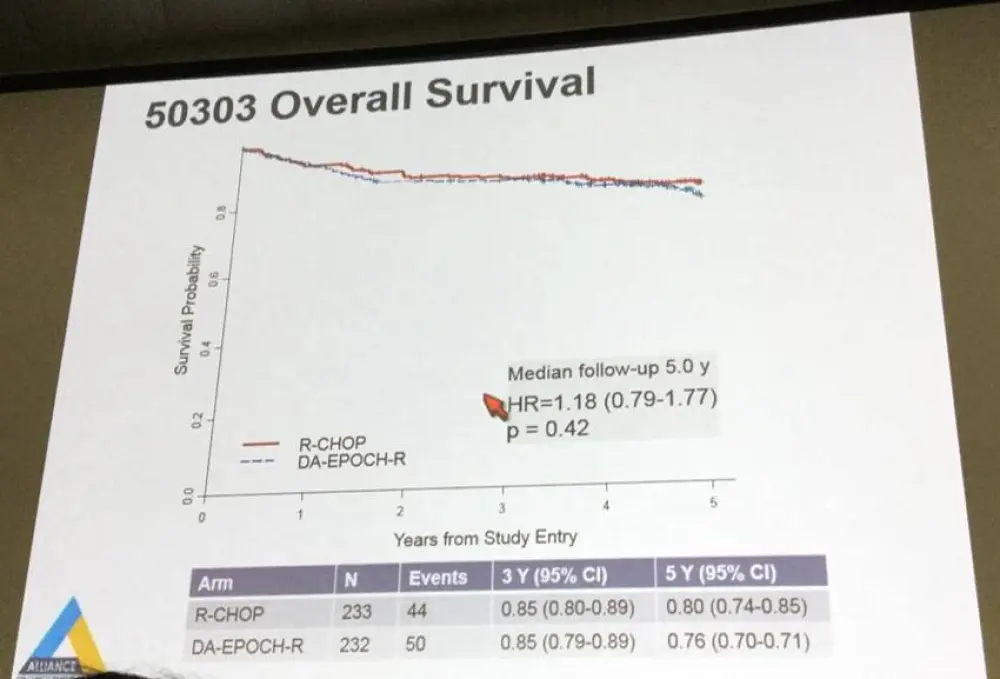
- At median follow up of 5.0 years, Overall Survival (OS) was similar in Arm A and Arm B (HR= 1.18, P = 0.42)
- AEs as the reason for treatment discontinuation occurred in 1.7% and 5.6% of patients in Arm A and Arm B, respectively
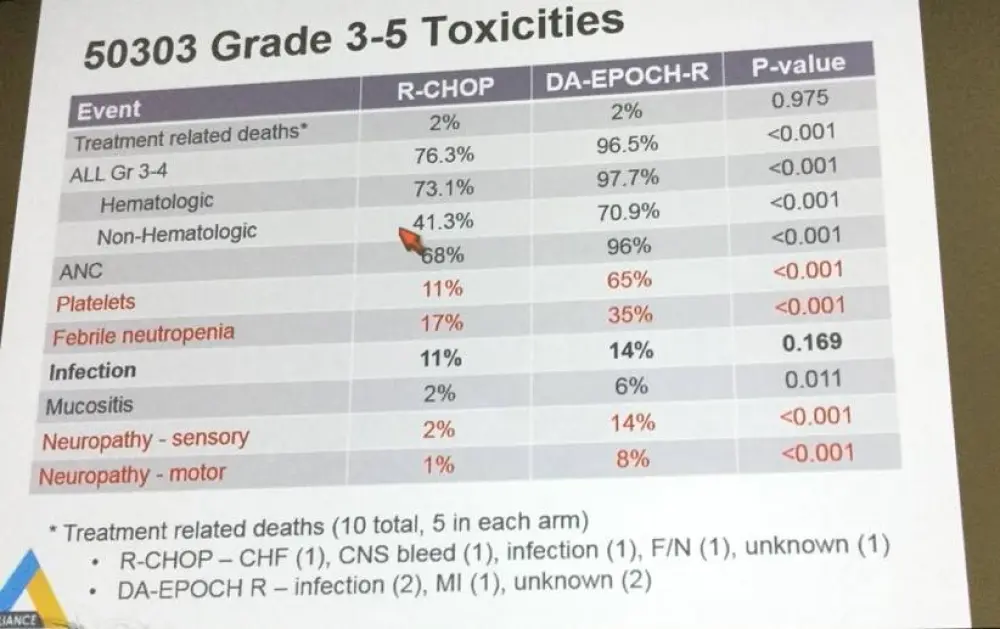
- Grade 4 neutropenia (90%; 56%), thrombocytopenia (35%; 6%), grade 3/4 febrile neutropenia (35%; 17%) and grade 3 neuropathy (motor: 8%; 1% and sensory: 14%; 2%) were more associated with Arm B compared to Arm A
- Grade 5 AEs were the same on both Arms
During this oral presentation, it was concluded that there were no differences observed in the EFS or OS between R-CHOP and DA-EPOCH-R, when considered in all patients. Additionally, although DA-EPOCH showed increased toxicity consistent with higher dose intensity, it did not have increased grade 5 AEs, which might suggest patterns of care in patients. More analyses are required to determine the effect of CNS relapse, GCB and ABC subtype, IPI, and age on the outcome of the two regimens. Further analysis of EFS and OS by age (<60 and ≥60) and by GCB versus ABC DLBCL are in process. Due to the low frequency of PMBL or MYC DLBCL, these data do not address the efficacy of these regimens in these subtypes. Molecular analyses are currently ongoing.
Abstract
Background: Diffuse large B-cell lymphoma (DLBCL) is comprised of multiple diseases with different outcomes, cell of origin and molecular pathogenesis. DLBCL derived from germinal center B-cells (GCB) and activated B-cells (ABC) constitutes over 80% of DLBCL. A small number of DLBCL tumors harbor MYC translocations, which are associated with a poorer prognosis. Primary mediastinal B-cell lymphoma (PMBL) occurs in younger patients and is typically treated with intensive or combined modality therapy. R-CHOP is the standard of care for DLBCL but has not been prospectively studied within DLBCL molecular subtypes. DA-EPOCH-R is an alternative and more dose-intensive regimen that showed a PFS of 81% at 4-years in a phase II multicenter CALGB study (Haematologica 2012; 97:758). CALGB/Alliance undertook a phase III randomized study to compare R-CHOP and DA-EPOCH-R in DLBCL and specifically within the GCB and ABC subtypes.
Methods: Patients had stage II or higher newly diagnosed DLBCL, age ≥ 18 years and were HIV negative. Subjects were randomized 1:1 to receive R-CHOP or DA-EPOCH-R as previously published. Central nervous system prophylaxis in at-risk patients was 12 mg intrathecal methotrexate in cycles 3-6 (4 doses total). All subjects with accessible tumor were required to have a biopsy or waiver. Subjects received a total of 6 treatment cycles. The primary study endpoints were EFS of R-CHOP (Arm A) versus DA-EPOCH-R (Arm B) and to develop a molecular predictor of outcome based on GCB and ABC DLBCL. Additional analyses include toxicity, pharmacogenomics and analysis of tumor genetics by next generation sequencing, and.
Results: 524 patients registered (262 on each arm) between May 2005 and May 2013. Efficacy analysis includes R-CHOP (n=233) and R-EPOCH (n=231) assigned patients with confirmed eligibility who received any treatment. Characteristics of patients registered to Arm A and B did not differ with median age (58; 56), male sex (53.2%; 53.7%), high-intermediate/high IPI (33.6%; 38.2%) and primary mediastinal B-cell lymphoma histology (6.9%; 5.2%). Therapy was completed per protocol in 89% and 83%, respectively, for Arm A and B, and disease progression on therapy was 2.6% and 1.7%. Adverse side effects leading to treatment discontinuation were 1.7% and 5.6%, respectively, for Arm A and B. Arm B compared to Arm A was associated with more grade 4 neutropenia (90%; 56%), grade 4 thrombocytopenia (35%; 6%), grade 3/4 febrile neutropenia (37%; 19%) and grade 3 neuropathy (motor: 8%;1% and sensory: 15%; 3%). Grade 5 events on study were the same in both arms. Preliminary analysis of EFS in confirmed eligible subjects shows no difference between Arm A and B with hazard ratio of 1.02 and p=0.89 at a median follow-up of 4.9 years. Overall survival is also similar with hazard ratio of 1.19 and p=0.40 at median 5.0 years. Additional analyses of EFS and OS by age (<60 and >=60) and by GCB versus ABC DLBCL are in process. Conclusions: There was no difference in EFS or OS between R-CHOP and DA-EPOCH-R when considering all patients. DA-EPOCH-R showed increased toxicity consistent with higher dose-intensity but not increased grade 5 toxicity. Compared to R-CHOP, more patients on DA-EPOCH-R did not complete treatment, which may reflect patterns of care or toxicity. Due to the clinical and genetic diversity of DLBCL, subset analyses are necessary to determine the effect of CNS relapse, GCB and ABC subtypes, age and IPI on outcomes of the two arms. These data do not address the efficacy of these regimens in PMBL or MYC+ DLBCL due to their low frequency, and where more dose-intense regimens appear to be important. Full molecular analyses are ongoing. Support: U10CA180821, U10CA180882, U10CA180888, CA180799, CA180820, CA180833, CA21076, CA21115.ClinicalTrials.gov Identifier: NCT00118209.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?