All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Rituximab Maintenance after Autologous Stem Cell Transplantation Prolongs Survival in Younger Patients with Mantle Cell Lymphoma: Final Results of the Randomized Phase III LyMa Trial of the Lysa/Goelams Group
The 58th Annual Meeting & Exposition of the American Society of Hematology (ASH) took place in San Diego, CA, and on December 3rd, Steven Le Gouill, MD, PhD, from Nantes University Hospital, France, presented the final results of the Phase-III randomized LyMa trial. The prospective trial was performed in young untreated MCL patients, who underwent maintenance rituximab (RM) following autologous stem cell transplant (ASCT).
Highlights:
- Treatment:
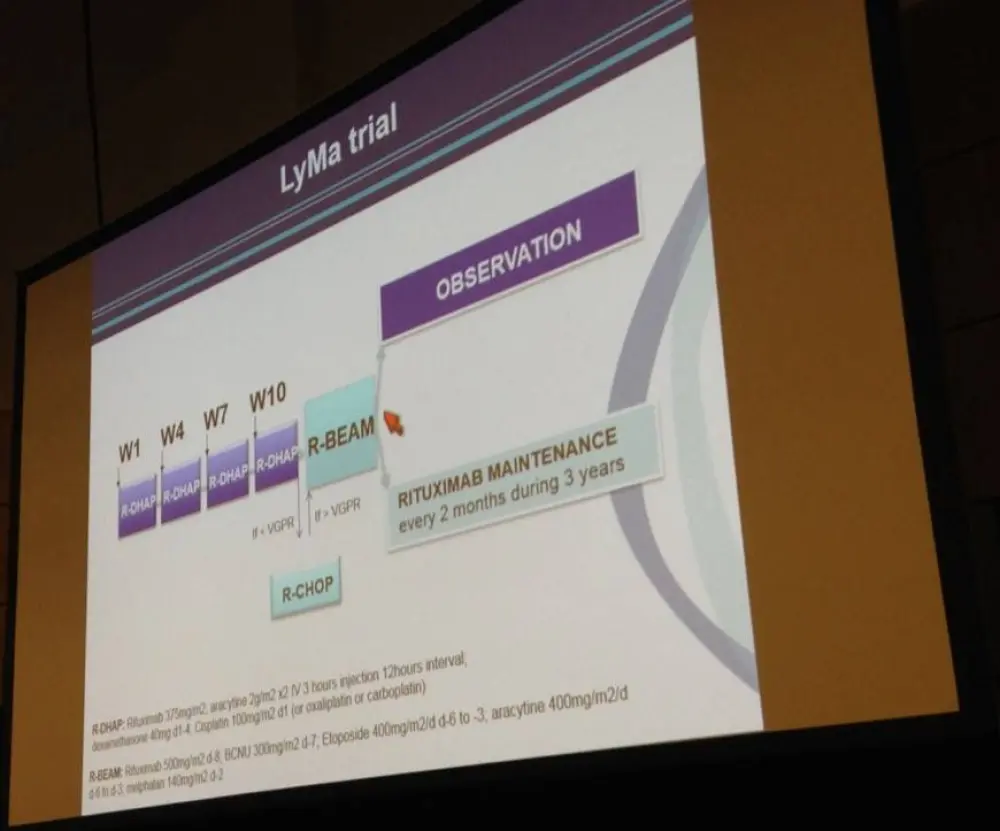
- All patients underwent four courses of D-HAP every 3 weeks before ASCT consolidation
- Unresponsive patients were given additional R-CHOP-14 for four courses before ASCT
- R-BEAM conditioning for ASCT
- ASCT responsive patients were then randomized to receive RM or no RM
- RM group = 375mg/m2 rituximab every two months for 36 months
- Final Analysis Results:
- 299 pts, <66yrs recruited
- 257 pts underwent ASCT (12 received R-CHOP/R-DHAP per above)
- 240 pts randomized, 120 no RM group, 120 RM group
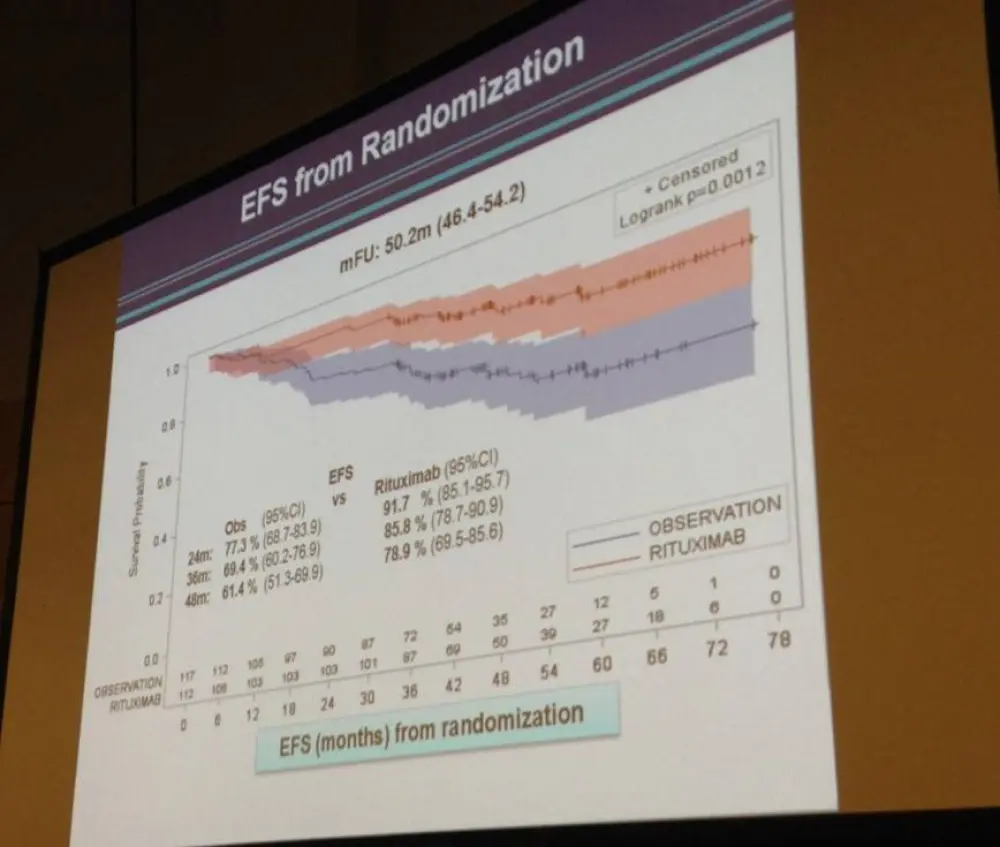
- 4 year EFS no RM = 61.4% vs. RM = 78.9% (P = 0.0012)
- EFS duration with RM had 54.3% reduction in event risk
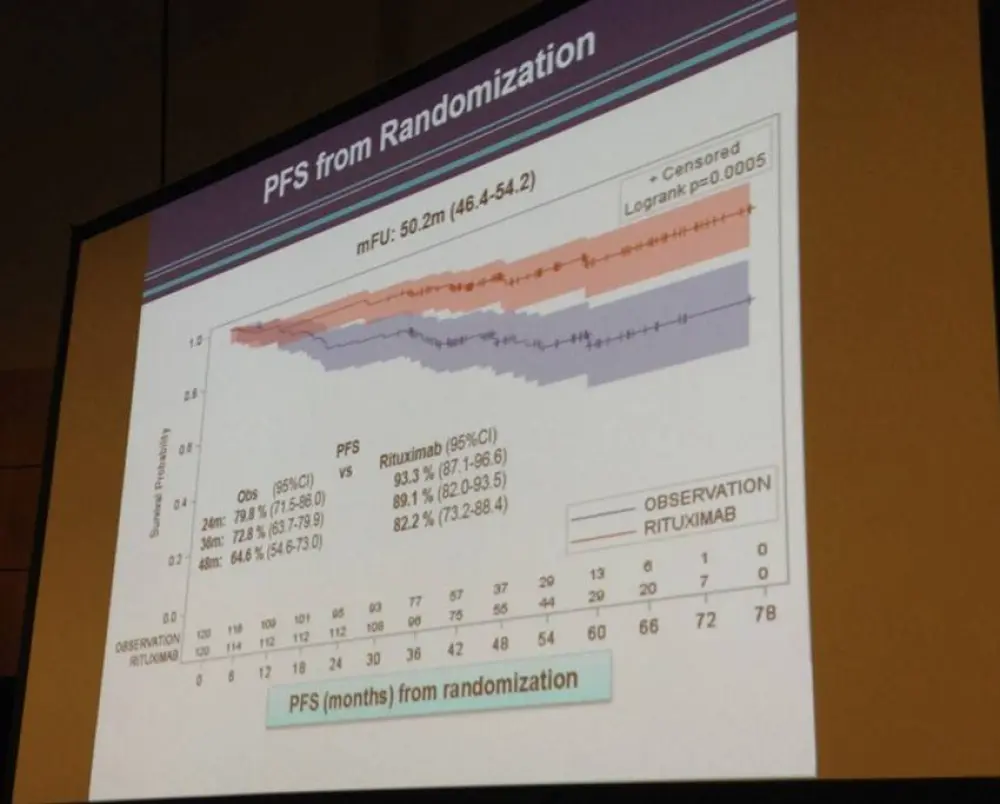
- 4-year PFS: no RM = 64.6% vs. RM = 82.2% (P = 0.0005)
- 4-year OS: no RM = 81.4% vs. RM = 88.7% (P = 0.0413)
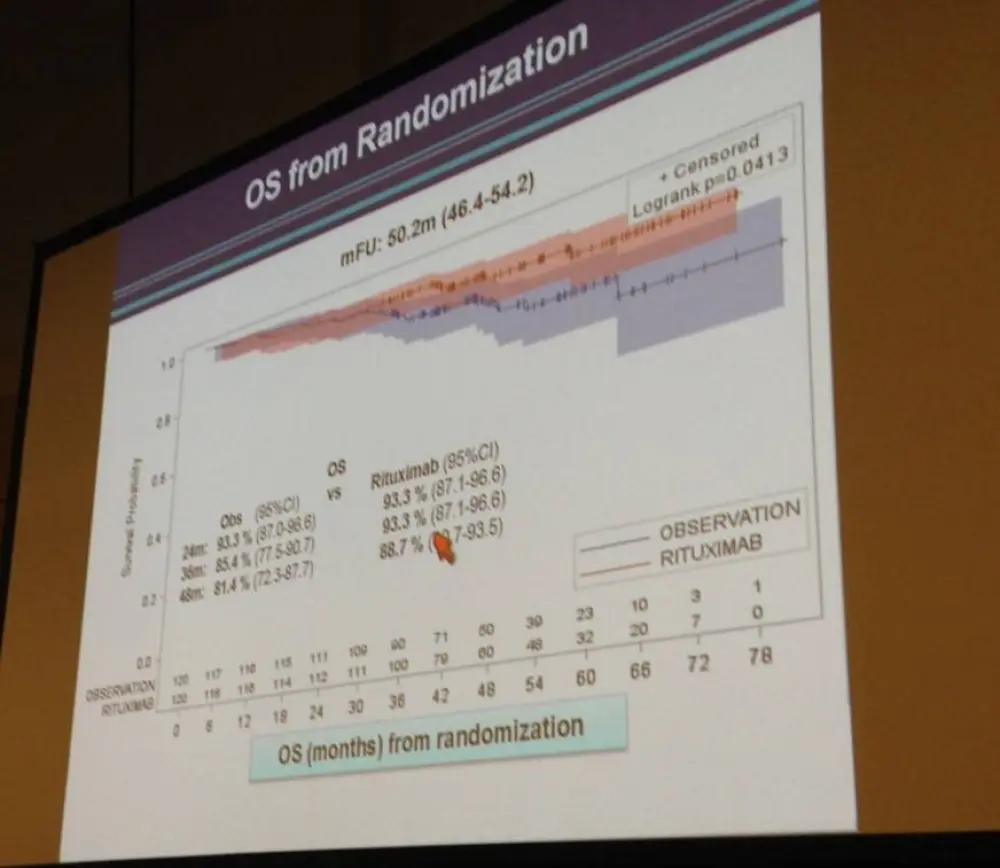
- Pts treated with RM had 60% reduction of progression risk (P=0.0007), and 50% lower risk of death (P = 0.0454)
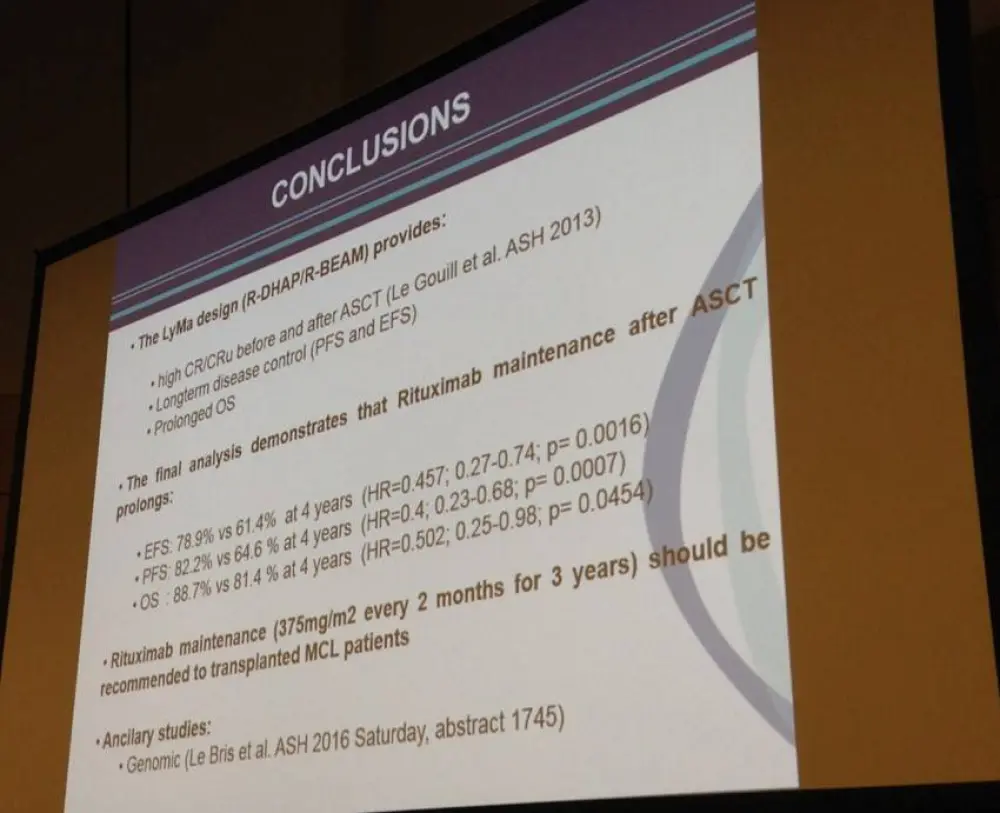
In summary, the RM group had better EFS, PFS, and OS. Steven Le Gouill then concluded his talk by stating that the LyMa trial results represents a new standard of care for young MCL patients of four courses of R-DHAP, ASCT, plus maintenance rituximab dosed at 375mg/m2 once every two months for three years.
Abstract:
Mantle cell lymphoma (MCL) accounts for approximately 6% of non-Hodgkin’s Lymphoma (NHL) in adults. MCL commonly responds to initial therapy but inevitably patients relapse and response duration decreases from one salvage therapy to the next. Indeed, there is an urgent need to control and/or eradicate residual MCL cells that are responsible for early and late relapses. Maintenance with Rituximab (RM) after R-CHOP has been shown to prolong OS in elderly MCL patients treated with R-CHOP (Kluin-Nelemans et al. NEJM). Induction with high-dose cytarabine followed by autologous stem cell transplant (ASCT) consolidation is standard of care for young patients but RM after ASCT has never been investigated so far. The LyMa trial (ClinicalTrials.gov, NCT00921414) is a prospective international randomized phase III trial that investigated RM after ASCT in young previously untreated MCL patients. Patients were included at diagnosis (<66y; stage >I, untreated, diagnosis of MCL according to WHO 2008 classification). Induction immuno-chemotherapy consisted of 4 courses of R-DHAP every 21 days (Rituximab, Dexamethasone, High-dose cytarabine, salt Platinum) followed by ASCT consolidation. Patients who were not in response (CR/CRu or PR) after R-DHAP received 4 additional courses of R-CHOP-14 before ASCT. The conditioning regimen for ASCT was R-BEAM. Patients in response after ASCT were randomized (1:1) between RM or no RM. RM consisted of one infusion of Rituximab (375mg/m2) every 2 months for 3 years. The primary endpoint was event-free survival (EFS) calculated from time of randomization; events were defined as disease progression, relapse, death, severe infection or allergy to Rituximab. Progression-free survival (PFS) and overall survival (OS) from time of diagnosis and time of randomization were secondary endpoints. The interim analysis showed a trend for a longer EFS and PFS in favor of RM arm. (Le Gouill et al, ASH 2014, abs 146). Herein, we present the results of the final analysis.
RESULTS. Two hundred and ninety nine patients were enrolled from September 2008 to August 2012. Demographic and clinical characteristics of the patients were as followed: median age of 57y (27-65), 79% of male, MIPI-low in 53.2%, MIPI-I in 27.4% and MIPI-H in 19.4%. After inclusion, 277 patients completed the 4 courses of R-DHAP. The CR/CRu rate after R-DHAP was 77.3% and ORR was 89.3%. Twenty patients received R-CHOP. In all, 257 patients (including 12 patients who received R-DHAP/R-CHOP) underwent ASCT. After ASCT, 240 patients were randomized (RM, n=120; no RM, n=120). Median follow-up (mFU) from inclusion and from randomization were 54.4m (52.7-59.2) and 50.2m (46.5-54.2), respectively. The mPFS and mOS from inclusion in an intention to treat analysis were not reached; the 4y-PFS and OS were 67.8% (95%CI, 62.1 to 72.8) and 78% (95%CI; 72.8 to 82.3), respectively. According to EFS definition, 47 (39.2%) patients had an event in the no RM versus 25 (20.8%) in the RM arm. The mEFS from randomization was not reached in both arms. The 4y-EFS was 61.4% (95%CI; 51.3 to 69.9) in the no RM arm vs 78.9% (95%CI; 69.6 to 85.6) in the RM arm (p=0.0012). The EFS duration was significantly superior in the RM arm with a 54.3% reduction in the risk of event (Hazard ratio (HR)= 0.457; 95%CI, 0.28 to 0.74; p=0.0016). The median PFS and OS from randomization were not reached in both arms. The 4y-PFS and OS from randomization were superior in the RM arm: 82.2% (95%CI; 73.2 to 88.4) vs 64.6% (95%CI; 54.6 to 73) (p=0.0005) and 88.7% (95%CI; 80.7 to 93.5) vs 81.4% (95%CI; 72.3 to 87.7)(p=0.0413). Patients in the RM arm had a 60% reduction of risk of progression (HR=0.4; 95%CI, 0.23 to 0.68; p=0.0007) and a 50% reduction of risk of death (HR=0.5; 95%CI, 0.25 to 0.98; p=0.0454). The per protocol analysis yielded similar results.
In conclusion, The LyMa trial demonstrates for the first time that RM after ASCT prolongs EFS, PFS and OS. Thus, 4 courses of R-DHAP plus ASCT (without TBI) followed by RM maintenance (one infusion every 2 month for 3 years) is a new standard of care for young MCL patients.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?