All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | ZUMA-1: KTE-C19 CAR-T cells show significant clinical benefit
On 3–6 December 2016, the Annual Meeting & Exposition of the American Society of Hematology (ASH) took place in San Diego, CA. On Tuesday 6th December, a Late-Breaking Abstracts session was held between 7:30am and 9:00am and was co-chaired by Jorge Di Paola, MD, of the University of Colorado, and Selina Luger, MD, of the University of Pennsylvania.
Late-Breaking Abstract 6 (LBA-6) was the last abstract presented during this session, titled “KTE-C19 (anti-CD19 CAR T Cells) Induces Complete Remissions in Patients with Refractory Diffuse Large B-Cell Lymphoma (DLBCL): Results from Pivotal Phase II ZUMA-1” by Sattva S. Neelapu, MD, from The University of Texas MD Anderson Cancer Center, Houston, TX, and colleagues.
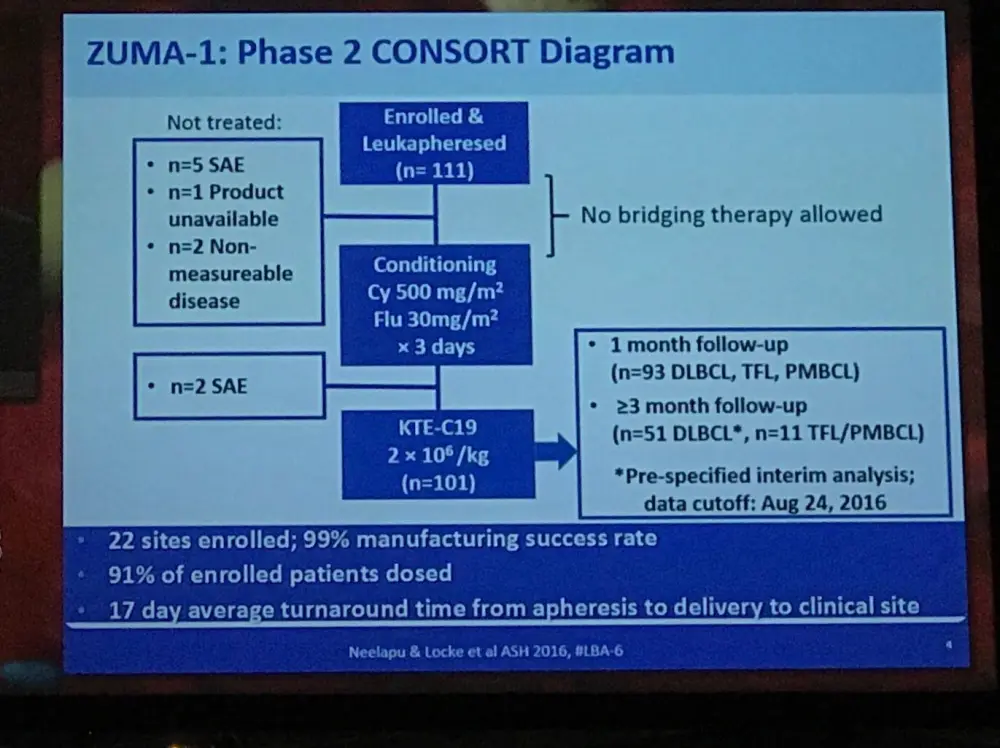
ZUMA-1 is the first multicenter trial of anti-CD19 CAR-T cells in refractory, aggressive NHL (NCT02348216). Two cohorts of patients are included in the Phase II portion of the ZUMA-1 study: DLBCL (cohort 1), and transformed FL (TFL) or PMBL (cohort 2). Results of a prespecified interim analysis were presented during this talk.
Overall, 111 patients from 22 different centers were enrolled and leukapheresed. Of these, 101 were administered KTE-C19. The study design is shown below:
Highlights:
- Successful manufacture of KTE-C19 was achieved in nearly all (99%) patients who enrolled
- Average turnaround time from apheresis to administration of KTE-C19 at the clinical site = 17.4 days
- 1 month follow-up (n=93): ORR = 71% (DLBCL 68%, PMBCL/TFL 80%), CR = 38% (DLBCL 33%, PMBCL/TFL 55%)
- Estimated 1-month PFS = 92%; estimated 3-month PFS = 56%
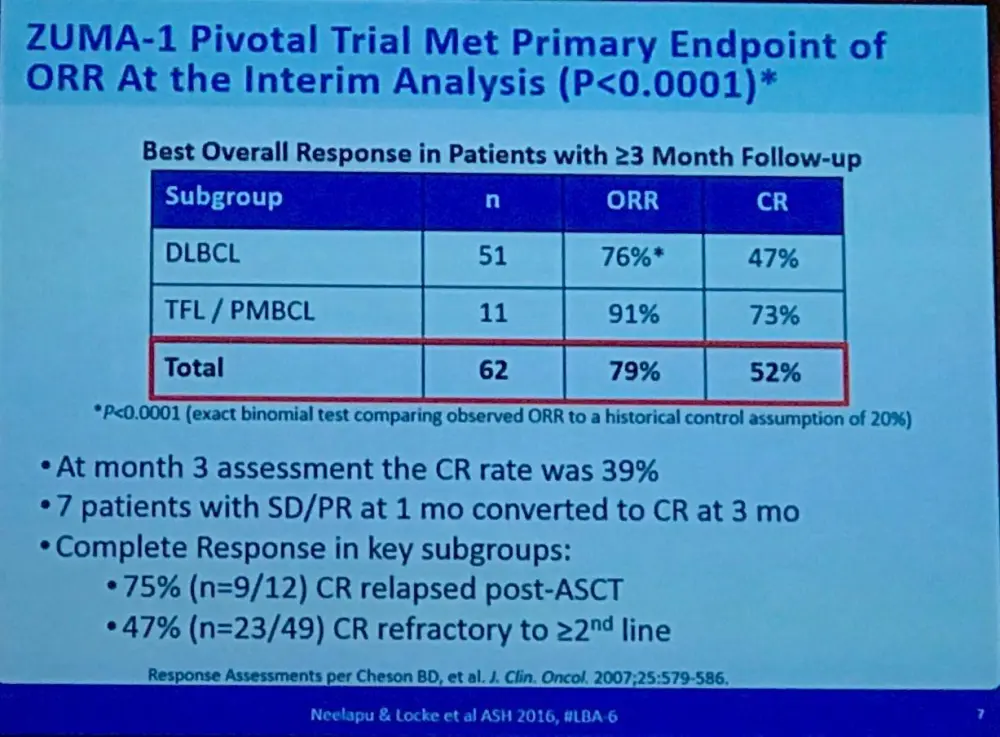
- Final interim analysis results: ORR = 76%; CRs = 47% (p<0.0001)
- Responses in patients refractory to chemo = 76%; Responses in patients who relapsed post-ASCT = 80%
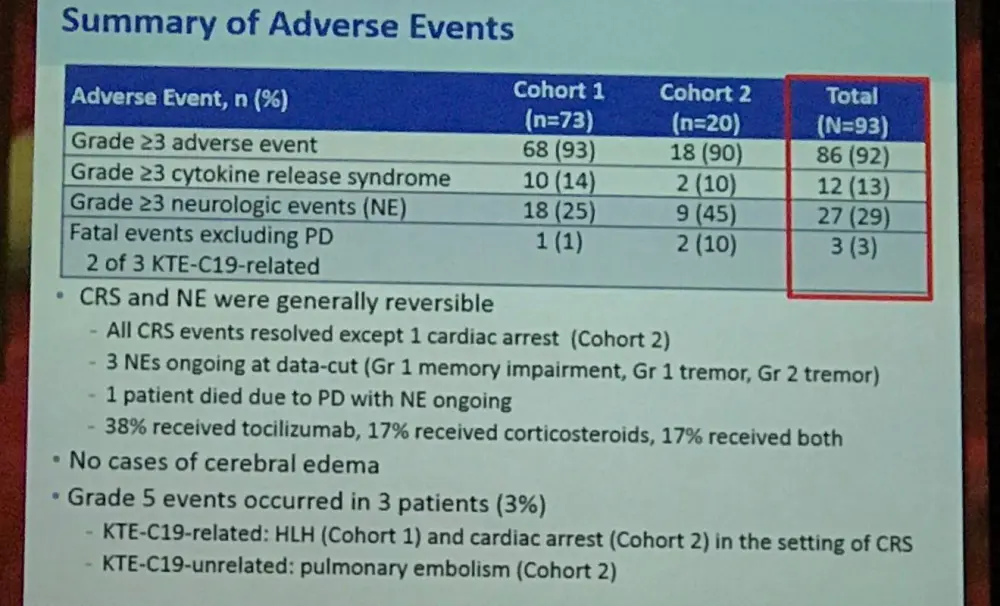
- The most frequently reported ≥grade 3 treatment-emergent AEs = neutropenia (67%), anemia (39%), thrombocytopenia (29%), febrile neutropenia (27%), and encephalopathy (24%)
- Grade ≥3 neurologic events and CRS were reported in 29% and 20% of patients, respectively
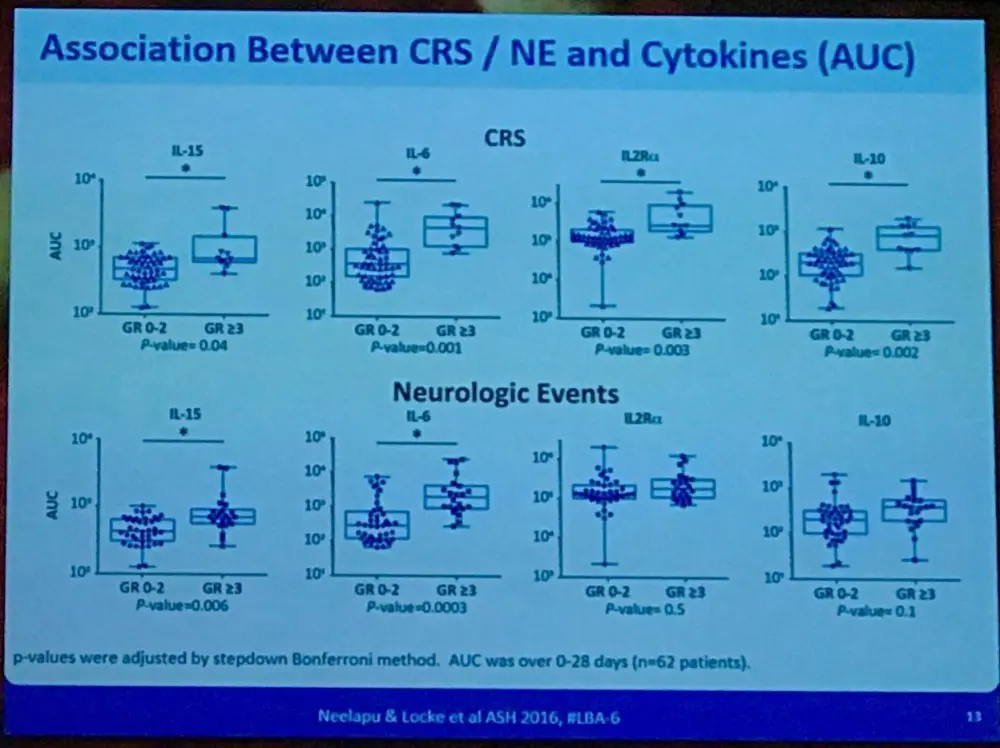
- Patients who experienced grade ≥3 neurological events had increased serum levels of IL-15, IL-6, IL-10, and IP-10 (P=0.0002, 0.003, 0.009, 0.0003, respectively)
Importantly, the data shown was stated as being consistent with earlier studies into KTE-C19 in aggressive NHL. Finally, this talk concluded by stating that KTE-C19 CAR-T cell therapy showed significant clinical benefit in patients with DLBCL and no other curative treatment options. Indeed, Sattva Neelapu stated that there was a 6-fold higher CR rate, with 39% durable CR after 3 months. The manufacture, logistics, and management of AEs were successfully carried out across 22 different institutions; the majority having no previous experience implementing CAR-T cell therapy. This pivotal, multicenter study provides exciting data for the field of CAR-T cell technology.
Abstract
Background: Patients (pts) with refractory aggressive non-Hodgkin lymphoma (NHL) have poor outcomes with currently available therapies, with a complete response (CR) rate of 8%, a partial response (PR) rate of 18%, and median overall survival (OS) of 6.6 months (mo) as demonstrated in the 635 pt SCHOLAR-1 meta-analysis (Crump, ASCO 2016; abstract 7516). ZUMA-1 is the first multicenter trial of anti-CD19 chimeric antigen receptor (CAR) T cells in refractory, aggressive NHL (NCT02348216). The phase 1 portion of ZUMA-1 showed ongoing CRs at 12+ mos in 43% of pts (Locke, ESMO 2016; abstract 1048O). The pivotal phase 2 portion of ZUMA-1 comprises 2 cohorts based on tumor type: DLBCL (cohort 1) and primary mediastinal B-cell lymphoma or transformed follicular lymphoma (cohort 2). Here, we present results of a prespecified interim analysis from cohort 1.
Methods: Pts received a target dose of 2 × 106 anti-CD19 CAR T cells/kg after a low-dose conditioning regimen of cyclophosphamide (500 mg/m2) and fludarabine (30 mg/m2) daily for 3 days. The primary endpoint is objective response rate (ORR) per 2007 IWG criteria. Key secondary endpoints include duration of response, frequency of adverse events (AEs), and levels of CAR T cells and serum cytokines. Key inclusion criteria include age ≥18 years, ECOG performance status (PS) 0-1, and refractory disease defined as progressive disease or stable disease as best response to last line of therapy, or disease progression ≤12 mos after autologous stem cell transplant (ASCT). Pts must have received a prior anti-CD20 antibody and an anthracycline-containing regimen. A prespecified interim analysis was to be conducted to determine early efficacy with a nominal alpha level of 0.017 in 50 treated pts in cohort 1 with a minimum follow-up of 3 mos.
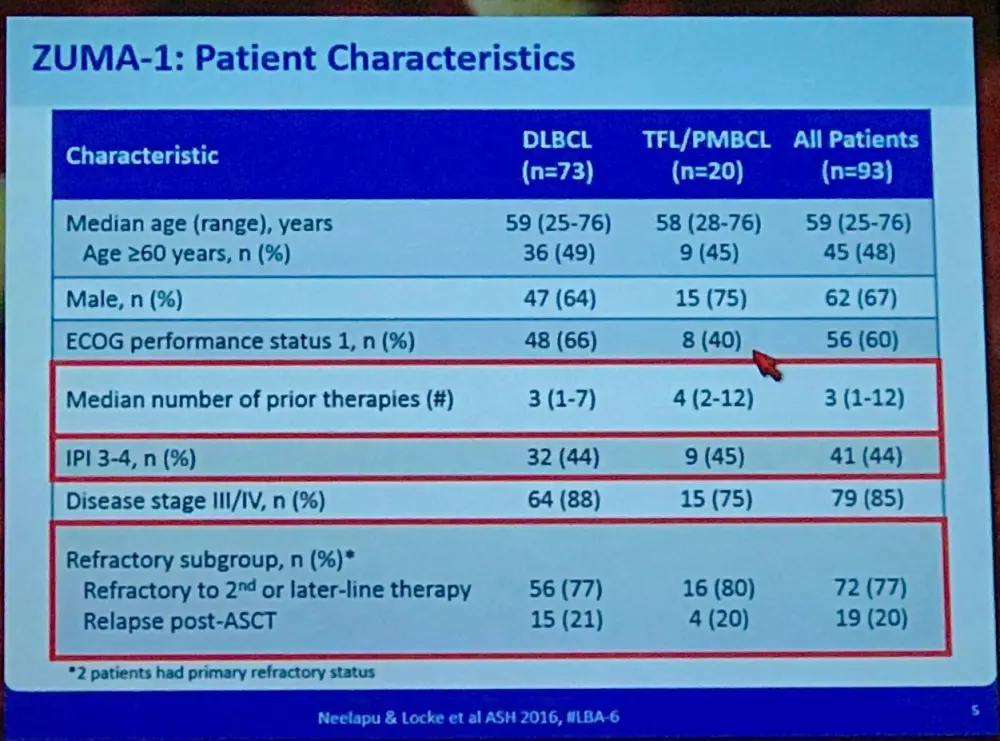
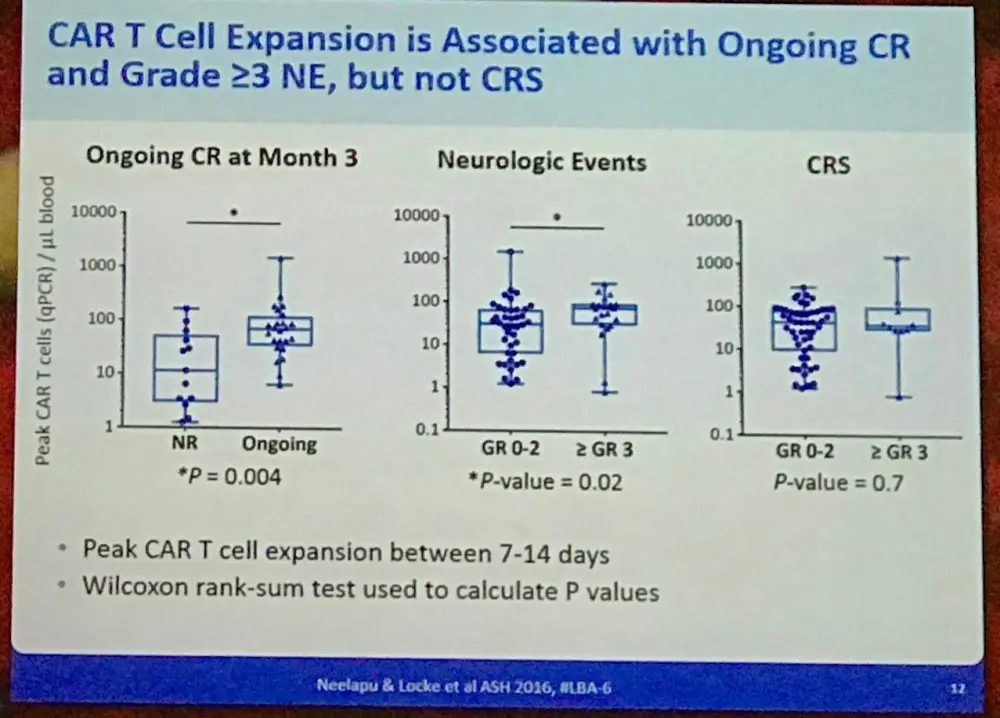
Results: In total, 111 pts from 22 institutions were enrolled and leukapheresed, and 101 pts received KTE-C19. As of August 24, 2016, 51 pts in cohort 1 were eligible for analysis. Median age was 58 years (range, 25-76), 73% were male, 71% had ECOG PS 1, 78% were refractory to ≥2 lines of therapy, 20% relapsed ≤12 mos of ASCT, and 61% were treated with ≥3 lines of prior therapy. KTE-C19 was successfully manufactured in 99% of pts enrolled. Average turnaround time from apheresis to receipt of KTE-C19 at the clinical site was 17.4 days. With an ORR of 76%, the study met the primary endpoint (P<0.0001; exact binomial test comparing observed ORR to a historical control assumption of 20%), with 47% CRs and 29% PRs. 92% of responses occurred within the 1st mo, and 39% of pts had ongoing responses (CR in 33%) at 3 mos. Responses were seen across key covariates, including refractory subgroup (refractory to chemotherapy=76%, relapse post ASCT=80%). Kaplan-Meier estimates of progression-free survival at 1 and 3 mos were 92% and 56%, respectively. The most common grade ≥3 treatment-emergent AEs were neutropenia (67%), anemia (39%), thrombocytopenia (29%), febrile neutropenia (27%), and encephalopathy (24%). Grade ≥3 cytokine release syndrome (CRS) and neurologic events occurred in 20% and 29% of pts, respectively. There was 1 grade 5 KTE-C19–related event of hemophagocytic lymphohistiocytosis. CAR T cells expanded within 14 days of KTE-C19 infusion, and peak expansion was associated with ongoing response at mo 3 (P=0.008). Pts who developed grade ≥3 neurological events had increased serum levels of IL-15 (P=0.0002), IL-6 (P=0.003); IL-10 (P=0.009) and IP-10 (P=0.0003). Cytokines/chemokines returned to baseline levels in most pts by day 28. Data from 93 pts with at least 1 mo of follow-up at the data cutoff will be presented.
Conclusions: ZUMA-1 is the first reported multicenter trial of CAR T cell therapy in pts with refractory aggressive NHL. KTE-C19 induced a nearly 6-fold higher CR rate compared to historical outcomes in SCHOLAR-1. Efficacy strongly associated with peak CAR T levels. Central manufacturing, logistics, and AE management were successfully implemented across 22 sites, most with no prior CAR T therapy experience. Results from cohort 2 of ZUMA-1 are also presented (Abstract #998). KTE-C19 demonstrated significant clinical benefit in pts with no curative treatment options.
Supported in part by funding from The Leukemia & Lymphoma Society Therapy Acceleration Program®. Drs Neelapu and Locke contributed equally to this study.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?