All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Clinical practice guidelines for transplant and cellular therapies in mantle cell lymphoma: recommendations from ASTCT, CIBMTR, and EBMT
Mantle cell lymphoma (MCL) is a B-cell lymphoma with marked heterogeneity in clinical presentation, molecular profile, and management—in both the frontline and relapsed/refractory (R/R) settings. Treatment options for frontline therapy include induction followed by high dose therapy and autologous (auto-) hematopoietic cell transplantation (HCT) consolidation, or combination chemoimmunotherapy regimens alone without subsequent high dose therapy consolidation. In high-risk R/R MCL, selection of treatment modality is even more complicated due to newer therapies such as Bruton’s tyrosine kinase (BTK) inhibitors, lenalidomide, and chimeric antigen receptor (CAR) T-cell therapy.
Due to the complexities associated with the treatment of MCL, it is important to have guidance on the contemporary role, optimal timing, and sequencing of cellular therapies in MCL to help experts in making better treatment related decisions.
Recently, Munshi, et al.1 published recommendations developed by joint effort of the American Society of Transplantation and Cellular Therapy (ASTCT), the Center of International Blood and Marrow Transplant Research (CIBMTR), and the European Society for Blood and Marrow Transplantation (EBMT) regarding the role, timing, and sequencing of auto-HCT, allogeneic (allo-) HCT and CAR T-cell therapy for patients with newly diagnosed and R/R MCL.
Methods
Panel composition
A steering committee comprised of six members—one representative each from ASTCT, EBMT and CIBMTR, two project coordinators, and an independent methodologist—drafted the protocol and initial consensus statements and practice considerations and set up a panel of experts. The panel consisted of 33 physicians and investigators with diverse geographical representation and expertise in the field of MCL, cellular therapy, and transplant.
Consensus methodology
The RAND-modified Delphi method was used to generate consensus statements addressing the role, timing, and sequencing of HCT and CAR T-cell therapies in patients with newly diagnosed and R/R MCL. The following steps were involved in the development of consensus statements (Figure 1 provides an outline for the process):
- concept development and approval by CIBMTR, EBMT, ASTCT
- protocol development according to the modified Delphi method
- identification of participant baseline demographics
- determination of project scope
- review of results of baseline demographics and project scope
- generation of questions related to sequence of cellular therapy and practice scenario for first voting survey (issued to panel)
- revision and modification of recommendations not reaching consensus threshold
- development of second voting survey including revised clinical practice recommendation statements
- drafting of manuscript if consensus has been reached based on pre-defined threshold
Mantle cell lymphoma (MCL) is a B-cell lymphoma with marked heterogeneity in clinical presentation, molecular profile, and management—in both the frontline and relapsed/refractory (R/R) settings. Treatment options for frontline therapy include induction followed by high dose therapy and autologous (auto-) hematopoietic cell transplantation (HCT) consolidation, or combination chemoimmunotherapy regimens alone without subsequent high dose therapy consolidation. In high-risk R/R MCL, selection of treatment modality is even more complicated due to newer therapies such as Bruton’s tyrosine kinase (BTK) inhibitors, lenalidomide, and chimeric antigen receptor (CAR) T-cell therapy.
Due to the complexities associated with the treatment of MCL, it is important to have guidance on the contemporary role, optimal timing, and sequencing of cellular therapies in MCL to help experts in making better treatment related decisions.
Recently, Munshi, et al.1 published recommendations developed by joint effort of the American Society of Transplantation and Cellular Therapy (ASTCT), the Center of International Blood and Marrow Transplant Research (CIBMTR), and the European Society for Blood and Marrow Transplantation (EBMT) regarding the role, timing, and sequencing of auto-HCT, allogeneic (allo-) HCT and CAR T-cell therapy for patients with newly diagnosed and R/R MCL.
Methods
Panel composition
A steering committee comprised of six members—one representative each from ASTCT, EBMT and CIBMTR, two project coordinators, and an independent methodologist—drafted the protocol and initial consensus statements and practice considerations and set up a panel of experts. The panel consisted of 33 physicians and investigators with diverse geographical representation and expertise in the field of MCL, cellular therapy, and transplant.
Consensus methodology
The RAND-modified Delphi method was used to generate consensus statements addressing the role, timing, and sequencing of HCT and CAR T-cell therapies in patients with newly diagnosed and R/R MCL. The following steps were involved in the development of consensus statements (Figure 1 provides an outline for the process):
- concept development and approval by CIBMTR, EBMT, ASTCT
- protocol development according to the modified Delphi method
- identification of participant baseline demographics
- determination of project scope
- review of results of baseline demographics and project scope
- generation of questions related to sequence of cellular therapy and practice scenario for first voting survey (issued to panel)
- revision and modification of recommendations not reaching consensus threshold
- development of second voting survey including revised clinical practice recommendation statements
- drafting of manuscript if consensus has been reached based on pre-defined threshold
Figure 1. Outline of the steps for manuscript development
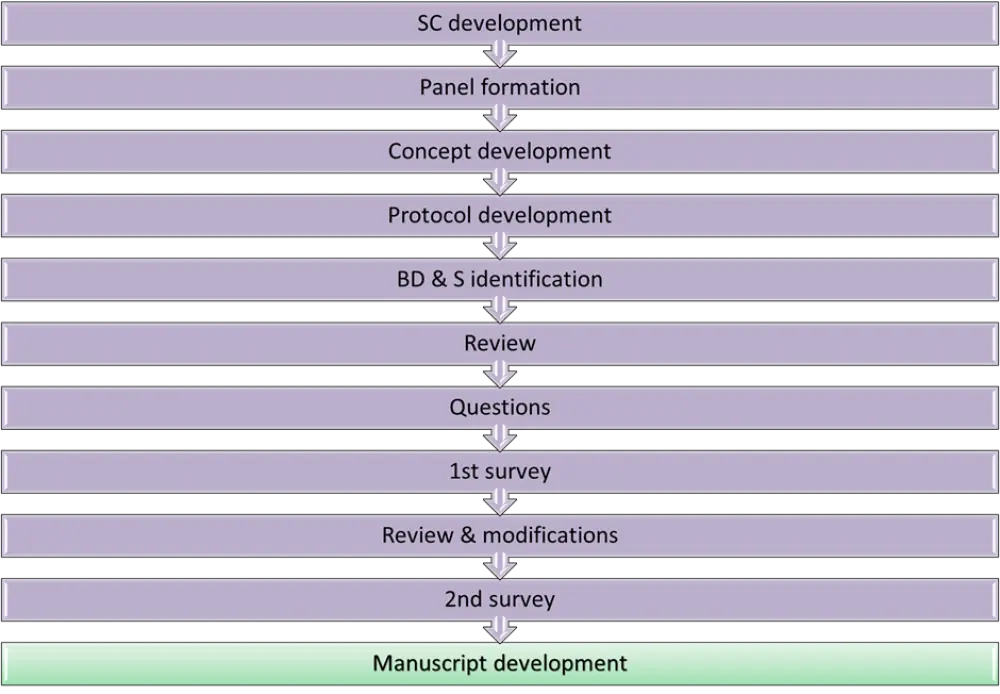
BD & S, baseline demographics and scope; SC, steering committee.
*Adapted from Munshi, et al.1
Results
The steering committee methodologist analyzed and summarized the results.
Demographic information about the members of consensus panel is included in Table 1.
Table 1. Demographic information of consensus panel members*
|
CAR-T, chimeric antigen receptor T cell; HCT, hemopoietic cell transplantation; MCL, mantle cell lymphoma; NDL, newly diagnosed lymphoma. |
|
|
Characteristics, % |
(n = 33) |
|---|---|
|
Male |
72.70 |
|
Academic practice setting |
93.9 |
|
>10 years of clinical experience in lymphoma and/or HCT practice |
66.7 |
|
Description of clinical practice |
|
|
Combined lymphoma and HCT/cell therapy practice |
75.8 |
|
Primarily HCT and/or cell therapy practice |
15.2 |
|
Estimated number of patients with NDL seen by individual member annually |
|
|
>75 |
69.7 |
|
51–75 |
18.2 |
|
26–50 |
9.1 |
|
Estimated number of patients with MCL seen by individual member annually |
|
|
>40 |
18.2 |
|
31–40 |
9.1 |
|
21–30 |
42.4 |
|
≤20 |
30.3 |
|
Estimated annual transplant volume (number of autologous plus allogeneic HCT) |
|
|
>300 |
39.4 |
|
201–300 |
21.2 |
|
101–200 |
27.3 |
|
51–100 |
9.1 |
|
Estimated annual autologous HCT performed |
|
|
>250 |
21.2 |
|
201–250 |
9.1 |
|
151–200 |
15.2 |
|
101–150 |
24.2 |
|
51–100 |
24.2 |
|
Estimated annual autologous HCT performed for lymphoma (Hodgkin plus non-Hodgkin) |
|
|
51–100 |
30.2 |
|
26–50 |
39.4 |
|
≤25 |
12.1 |
|
Estimated annual CAR T-cell therapies performed for lymphoma (on or off clinical trial) |
|
|
>20 |
63.6 |
|
16–20 |
9.1 |
|
11–15 |
15.2 |
|
≤10 |
12.1 |
First voting survey
The first voting survey consisted of 19 statements which were:
- specific to the role of auto-HCT in eligible patients with newly diagnosed MCL (6 statements)
- for patients with R/R MCL (2 statements)
- about allo-HCT for newly diagnosed patients with MCL (3 statements)
- about allo-HCT and/or CAR T-cell therapy for R/R MCL (8 statements)
All but five statements achieved consensus by predefined criteria (<75% agreement); four were revised and one was abandoned. Of the five statements that did not achieve consensus, three were proposed for the second voting survey after discussion via virtual video conference.
Second voting survey
The three statements included in the second voting survey (two reformulated statements and one merged statement) met the predefined criteria for consensus.
Consensus statements in the front-line setting for MCL
Final clinical practice guideline consensus statements for transplantation and CAR T-cell treatments in the frontline setting for MCL are stated in Table 2.
Table 2. Clinical practice recommendations for HCT in the frontline setting for MCL
|
CAR-T, chimeric antigen receptor T cell; CR/PR, complete remission/ partial remission; HCT, hemopoietic cell transplantation; MCL, mantle cell lymphoma; MIPI, mantle cell lymphoma international prognostic index; MIPI-c, combined MIPI; MRD, measurable residual disease; NDL, newly diagnosed lymphoma. |
|
|
Consensus statement |
Grading of recommendations |
|---|---|
|
The panel recommends autologous HCT as consolidation therapy in eligible, newly diagnosed MCL patients (without TP53 mutation or bi-allelic deletion) in CR/PR after first-line therapies. |
A |
|
The panel does not recommend autologous transplantation as consolidation therapy in patients with MCL experiencing disease not responsive to most recent anti-lymphoma therapy. |
B |
|
The panel does not recommend using MRD testing to guide use of autologous transplant consolidation after first-line therapies in MCL, outside the setting of a clinical trial. |
C |
|
The panel does not recommend using MIPI or MIPI-c prognostic score as a criterion determining use of autologous transplantation as consolidation therapy in eligible newly diagnosed patients with MCL in first CR/PR after first-line therapies. |
C |
|
The panel does not recommend allogeneic transplant consolidation in patients with MCL (without TP53 mutation or bi-allelic deletion), achieving a CR/PR after first-line therapies. |
B |
|
The panel does not recommend consolidation with CAR T-cell therapy in patients with MCL, achieving a CR/PR after first-line therapies, outside the setting of a clinical trial. |
C |
|
If a TP53 mutation (or bi-allelic deletion) is present, the panel recognizes that outcomes are poor for patients with MCL in complete or partial remission after first-line therapies who then undergo autologous transplantation. However, no specific alternative strategy has yet been shown to improve outcomes in such patients. Therefore, the panel recommends considering autologous transplant consolidation as well as alternative consolidation strategies (e.g., CAR T-cell therapy or allogeneic transplantation), ideally in the context of a clinical trial, for such patients. |
C |
|
A = good research-based evidence; B = fair research-based evidence; C = based on expert opinion and panel consensus |
|
Consensus statements for R/R-MCL
Final clinical practice guidelines consensus statements for transplantation and CAR T-cell treatments for relapsed and/or refractory MCL are stated in Table 3.
Table 3. Final clinical practice guidelines statements for HCT for R/R-MCL
|
BTK, Bruton’s tyrosine kinase; CAR-T, chimeric antigen receptor T cell; CR/PR, complete/ partial remission; HCT, hemopoietic cell transplantation; MCL, mantle cell lymphoma. |
|
|
Consensus statement |
Grading of recommendation |
|---|---|
|
If a TP53 mutation (or bi-allelic deletion) is present, the panel does not recommend autologous transplantation in relapsed patients with MCL achieving a CR/PR after second or subsequent lines of therapy. |
B |
|
The panel recommends both CAR T-cell therapy or allogeneic transplant consolidation as acceptable options, in relapsed patients MCL with TP53 mutation (or bi-allelic deletion) in a CR/PR after second or subsequent lines of therapy. |
C |
|
If a TP53 mutation (or bi-allelic deletion) is present, the panel recommends treatment with CAR T-cells in relapsed patients with MCL, with disease unresponsive to last anti-lymphoma therapy. |
B |
|
In relapsed patients with MCL, the panel recommends offering CAR T-cell therapy before proceeding with allogeneic transplantation. |
C |
|
Regarding timing of CAR T-cell application in relapsed patients with MCL (without TP53 mutation or bi-allelic deletion), the panel recommends offering CAR T-cell therapy to patients relapsing after (or who are intolerant to) at least one BTK inhibitor. |
B |
|
The panel does not recommend allogeneic transplantation in relapsed patients with MCL experiencing disease refractory to most recent anti-lymphoma treatment. |
B |
|
The panel recommends allogeneic transplantation for eligible relapsed patients with MCL that have achieved only a partial remission with a BTK inhibitor in second or subsequent treatment line, particularly in regions without access to CAR T-cell therapy or in subjects where such therapy is not feasible. |
B |
|
The panel recommends allogeneic transplantation in eligible patients with MCL relapsing/progressing after CAR T-cell therapy, if they achieve a CR/PR or if they have stable disease with subsequent anti-lymphoma therapies. |
C |
|
Among eligible patients with MCL lacking a TP53 mutation (or bi-allelic deletion) not undergoing autologous transplant consolidation following first-line therapies, the panel recommends considering autologous transplantation consolidation therapy in patients who have achieved a complete remission after second line chemo-immunotherapies. |
B |
|
The panel recommends considering allogeneic transplant consolidation in eligible patients with MCL who still have detectable disease, at 3 or more months following CAR T-cell therapy. |
C |
|
A = good research-based evidence B = fair research-based evidence C = based on expert opinion and panel consensus |
|
Conclusion
The guidelines and recommendations reported in this article, for the use of HCT in the treatment of newly diagnosed and R/R MCL, would be useful to address the gaps in knowledge regarding optimal timing and sequencing of these therapies in patients with MCL.
These guidelines recommend auto-HCT consolidation in the first-line setting as standard-of-care in eligible patients, though the panel acknowledged that, due to a lack of evidence for a survival benefit with upfront auto-HCT consolidation, some centers do not routinely recommend auto-HCT after frontline intensive induction regimens.
In the R/R setting, the preferential option is CAR T-cell therapy, especially in patients with MCL not responding/ intolerant to at least one BTK inhibitor, due to increased toxicities and life-threatening complications of allo-HCT. Allo-HCT is recommended if CAR T-cell therapy fails, if the patient achieves complete or partial remission, or if the patient has stable disease with subsequent anti-lymphoma treatment.
The authors concluded that RAND-modified Delphi methodology is effective in providing a formal framework for the development of consensus recommendations for the timing and sequence of cellular therapies for MCL. Lack of evidence for certain modalities, such as allo-HCT and CAR T-cell therapy, has limited their use in clinical practice; however, the treatment algorithm will eventually evolve with progress in the area of CAR T-cell therapy and BTK inhibitors.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?