All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
EHA-SWG 2017 | Rare Lymphomas: double hit lymphoma
On March 10–12 2017, the EHA-SWG meeting on Rare Lymphomas took place in Barcelona, Spain, and was jointly chaired by Prof. Martin Dreyling, from Klinikum der Universität München, Germany, and Prof. Marie José Kersten, from the Academic Medical Center, Amsterdam, The Netherlands.
On March 11th 2017, I. Aurer (University Hospital Centre Zagreb, Croatia) gave a talk titled “Double hit lymphoma”, during the “MYC-driven lymphomas” scientific session.
The talk began by stating that it has been “recognized years ago” that diseases harboring t(14;18) and t(8;14) or t(8;22) are associated with a poorer prognosis. In the 2008 WHO classification, Double Hit Lymphoma (DHL) fell into the B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and Burkitt Lymphoma. In the latest revision, DHL was recognized as a distinct nosological entity under the category “High-grade B-cell lymphoma, with MYC and BCL2 or BCL6 translocations”.
Aurer then discussed how DHLs are defined, their incidence, and predispositions:
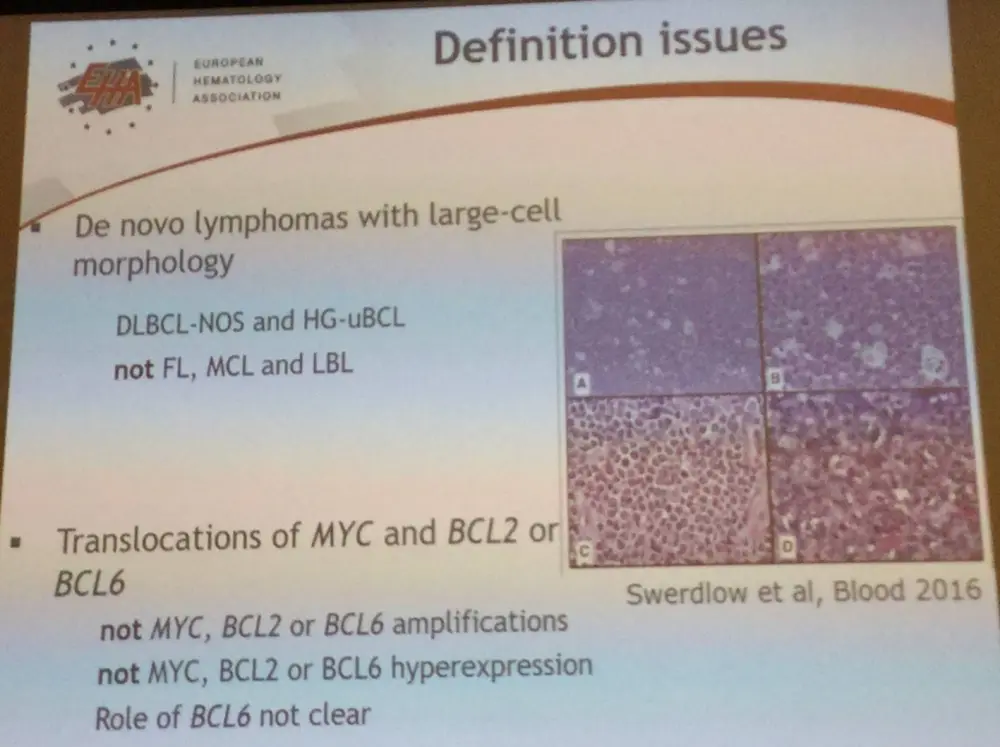
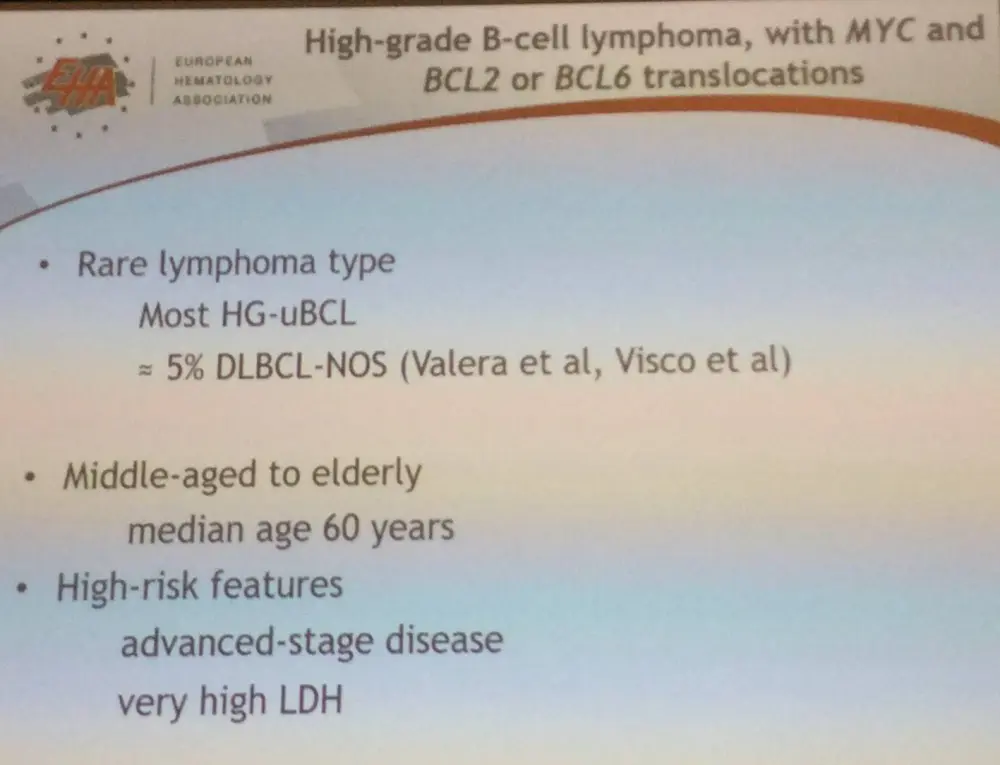
The majority (90%) of DHLs carry BCL2 translocations. Currently, it is unclear whether DHLs which carry BCL6 translocations have an equally bad prognosis as those which carry BCL2 translocations. Moreover, it is uncertain if Triple Hit Lymphomas (i.e. MYC, BCL2, and BCL6 translocations) carry different biological characteristics and prognoses from DHLs.
In the current definition, other types of genetic rearrangements, such as amplifications, are not included. Also, it is uncertain whether FISH, which is not routinely used in the diagnosis of DLBCL, should be carried out in all patients or just those the GC-DLBCL with sufficiently high MYC and BCL2/BCL6 expression by IHC.
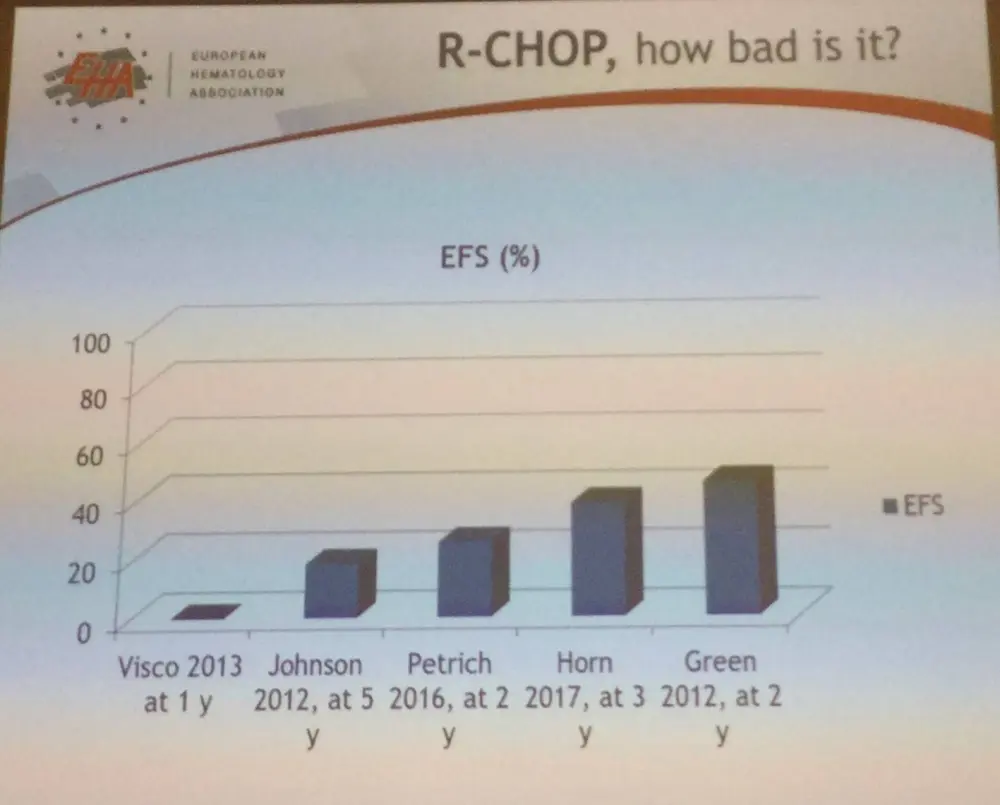
Aurer moved on to discuss DHL treatment, by stating that there is a consensus that results with R-CHOP are “unacceptably bad”, with 2-year PFS ranging from 0–45%.
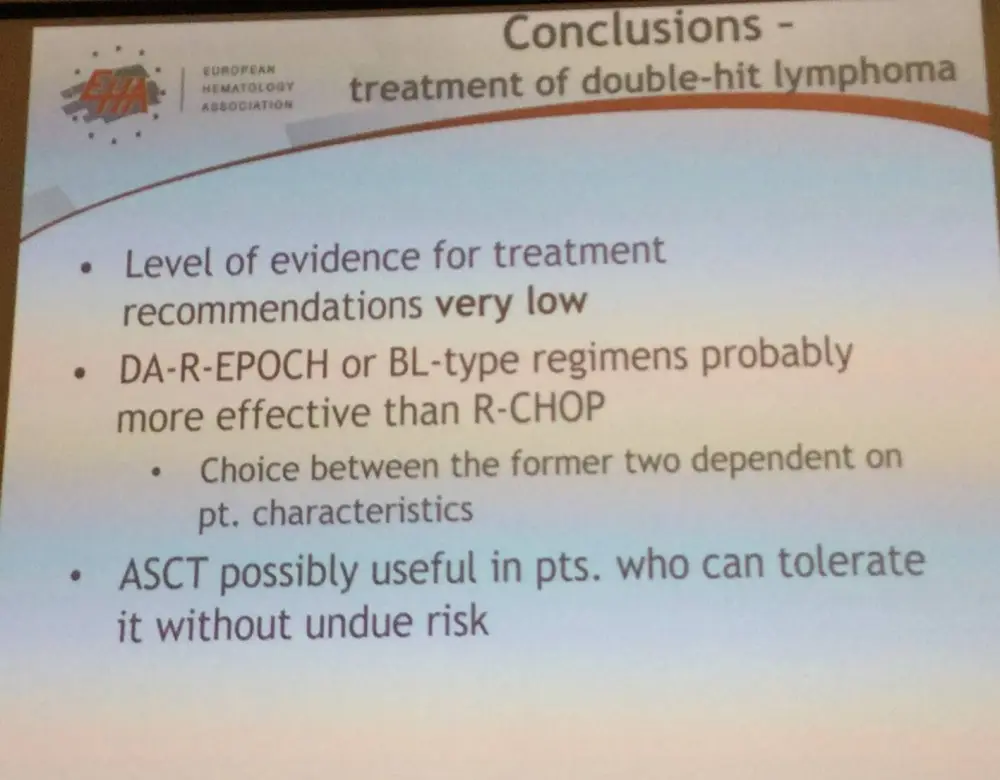
DA-R-EPOCH, R-HyperCVAD, and R-CODOC-M/IVAC (more aggressive regimens) potentially improve 2-year PFS (to 32–67%), however the difference is not always statistically significant. Moreover, due to the number of salvage regimens being very limited in patients who fail more aggressive regimens, improvement in OS is even worse.
Aurer also made the point that comparisons between DA-R-EPOCH and Burkitt Lymphoma-type regimens (e.g. R-Hyper-CVAD and R-CODOX-M/IVAC) are hindered due to the latter regimens being commonly used in high-risk disease patients and so “no meaningful conclusions regarding differences in efficacy can be obtained from currently available data”.
During the talk, it was also stated that patients who received an autograft in first remission appeared to trend towards an improved DFS.
Aurer ended the talk with a succinct conclusion:
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?