All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Emerging novel therapies for the treatment of patients with aggressive R/R NHL
Introduction
Despite the success of chimeric antigen receptor (CAR) T-cell therapies in patients with relapsed/refractory (R/R) non-Hodgkin lymphoma (NHL), responses are not robust in all patients and many experience disease progression following treatment; therefore, there is an urgent need for novel therapies in this population.1 CAR T-cell products and small molecule agents are being evaluated in clinical trials aimed at improving upon the clinical efficacy and safety of currently available products.
Results from the following three novel therapeutic trials were presented at the European Hematology Association (EHA) 2022 Congress: a phase I study of YTB323, a next-generation CAR T-cell therapy in patients with R/R diffuse large B-cell lymphoma (DLBCL)1; a phase I/II study of anbalcabtagene autoleucel (anbal-cel), a novel anti-CD19 CAR T-cell therapy with dual silencing of PD-1 and TIGIT in R/R large B-cell lymphoma (LBCL)2; and a phase I study evaluating the clinical activity of CC-99282, an E3 ligase modulator (CELMOD) agent, in patients with R/R NHL.3 Below, we highlight the key findings from each study.
Phase I study of YTB323, a next-generation CAR T-cell therapy, in patients with R/R DLBCL
YTB323 is manufactured through an innovative process involving cell expansion, primarily within the body of the patient. This method reduces the CAR T-cell manufacturing time and preserves both the naïve and stem cell memory T cells to reduce T-cell exhaustion, increasing functionality and persistence. It is anticipated that this will lead to increased efficacy and more durable responses in patients.
Study design
Patients aged ≥18 years with measurable disease at study entry, Eastern Cooperative Oncology Group Performance Status of 0–1, and R/R DLBCL ≥2 prior lines of therapy or hematopoietic stem cell transplantation were included in this study. Figure 1 shows the treatment regimen for patients infused with YTB323.
The primary endpoints were incidence of dose-limiting toxicities (DLTs) and adverse events to determine a recommended dose. The secondary endpoints included overall response rate (ORR), duration of response (DOR), overall survival, and cellular kinetics.
Figure 1. Treatment regimen for patients with R/R DLBCL infused with YTB323*
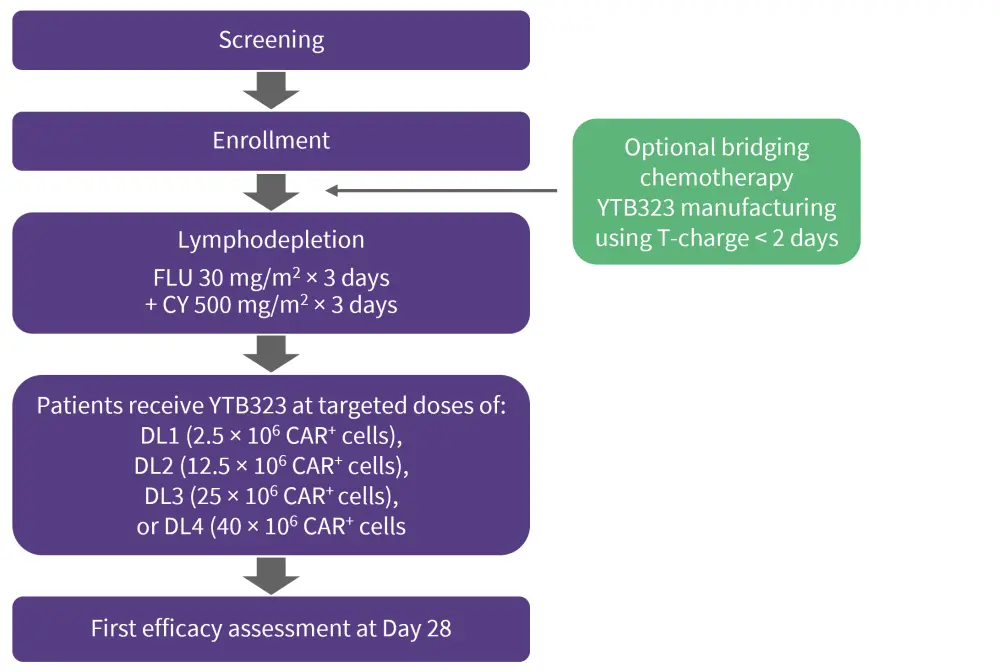
CAR, chimeric antigen receptor; CY, cyclophosphamide; DL, dosing level; DLBCL, diffuse large B-cell lymphoma; FLU, fludarabine; R/R, relapsed/refractory.
*Data from Dickinson.1
Results
Baseline characteristics
Baseline characteristics for patients infused with YTB323 (N = 45) are summarized in Table 1.
Table 1. Baseline characteristics of patients with R/R DLBCL treated with YTB323*
|
DLBCL, diffuse large B-cell lymphoma; HSCT, hematopoietic stem cell transplantation; LDG, laparoscopic distal gastrectomy; ULN, upper limit of normal. |
|
|
Variable, % (unless otherwise stated) |
YTB323 infused (N = 45) |
|---|---|
|
Median age (range), years |
64.8 (41–79) |
|
Race |
|
|
Asian |
2.2 |
|
White |
93.3 |
|
Histology |
|
|
DLBCL |
95.6 |
|
Transformed lymphoma/other |
4.4 |
|
Elevated LDG (>ULN) |
55.6 |
|
Prior HSCT |
28.9 |
|
Prior lines of therapy |
|
|
2 |
66.7 |
|
>3 |
33.3 |
|
Time since most recent relapse/progression to YTB323, median (range), months |
2.8 (1.4–81.8) |
|
Received bridging therapy |
66.7 |
Safety
Almost all patients experienced at least one AE of any grade. At dose level (DL) 2, the selected dose, DLTs occurred in two patients (7%), one with Grade 4 cytokine-release syndrome (CRS) and the other with Grade 4 cytopenia (Table 2). There were no further DLTs, despite six patients receiving higher doses, and no deaths were reported.
The overall incidence of CRS was low, with 36% (10/28) of patients experiencing Grade 1/2 events and one patient experiencing a Grade 3/4 event. For the management of CRS, tocilizumab was given to seven patients, corticosteroids to three patients, and vasopressor to one patient at DL2. CRS had a delayed onset of 10 days and lasted for a median of 4 days at the selected dose. At DL2, immune cell-associated neurologic syndrome occurred in three patients (10.7%) at 10, 16, and 28 days; two patients had Grade 3/4 and one patient had Grade 1/2. For the management of immune cell-associated neurologic syndrome, two patients received dexamethasone and anakinra and one patient received methylprednisolone.
Table 2. Adverse events in patients with R/R DLBCL treated with YTB323*
|
AE, adverse event; CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome. |
||||
|
Adverse events, % (unless |
YTB323 |
YTB323 |
YTB323 |
YTB323 |
|---|---|---|---|---|
|
Any AE |
|
|
|
|
|
Any grade |
100 |
96 |
86 |
100 |
|
Grade >3 |
100 |
86 |
86 |
100 |
|
Dose-limiting toxicities |
0 |
7 |
0 |
0 |
|
Deaths |
50 |
14 |
0 |
33 |
|
Related to YTB323 |
0 |
0 |
0 |
0 |
|
Infections |
|
|
|
|
|
Any grade |
50 |
21 |
29 |
50 |
|
Grade> 3 |
25 |
14 |
0 |
33 |
|
CRS |
25 |
36 |
29 |
33 |
|
Grade 1/2 |
25 |
32 |
29 |
33 |
|
Grade 3/4 |
0 |
4 |
0 |
0 |
|
Time to onset, days |
9 |
10 (1–17) |
7.36 |
2.9 |
|
Time from onset to resolution, days |
5 |
4 (1–18) |
5.10 |
5.7 |
|
ICANS |
0 |
10.7 |
0 |
33.3 |
|
Grade 1/2 |
0 |
3.6 |
0 |
33.3 |
|
Grade 3/4 |
0 |
7.1 |
0 |
33.3 |
|
Time to onset, days† |
— |
10, 16, 28 |
— |
6, 28 |
|
Time from onset to resolution, days |
— |
11, 16, 24 |
— |
1, 36 |
Efficacy and cellular kinetics
Across all dose groups, the ORR and complete response (CR) rates were 69% and 62%, respectively, at Day 28. At DL2, the ORR and CR were 69% and 65%, respectively. Responses were durable with CR maintained at 63% and 69% after 3 and 6 months, respectively. Median DOR was not reached. YTB323 expansion at DL2 was comparable to the higher end of tisagenlecleucel expansion, at a 25-fold lower dose.
Figure 2. Response rates in patients with R/R DLBCL who were treated with YTB323*
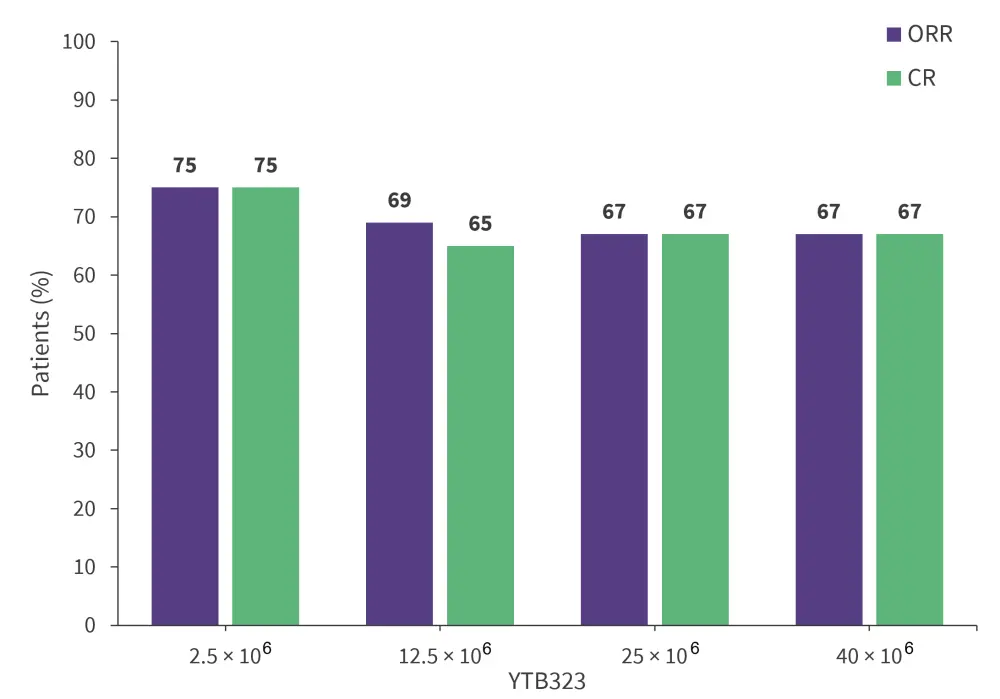
CR, complete response; ORR, overall response rate.
*Data from Dickinson.1
Phase I/II study of anbal-cel, a novel anti-CD19 CAR T-cell therapy with dual silencing of PD-1 and TIGIT, in R/R LBCL
One potential reason for the failure of CAR T-cell therapy is the reduction of CAR+ T-cells due to the high expression of immune checkpoint proteins, such as TIGIT and PD-1. Anbal-cel is designed to downregulate the expression of both PD-1 and TIGIT in order to sustain the efficacy and durability of CAR T-cells.
Study design
Key eligibility criteria:
- Either DLBCL-not otherwise specified, high-grade B-cell lymphoma (HGBL), primary mediastinal B-cell lymphoma, or transformed follicular lymphoma
- Eastern Cooperative Oncology Group Performance Status of 0–1
- R/R after ≥2 lines of prior therapies
- Appropriate organ functions
- No prior CD19 targeted therapy
The treatment regimen can be seen in Figure 3.
The primary endpoints were safety related and included DLTs and maximum tolerated dose (MTD). The secondary endpoints included ORR, DOR, progression-free survival, and overall survival.
Figure 3. Treatment regimen for patients infused with anbal-cel*
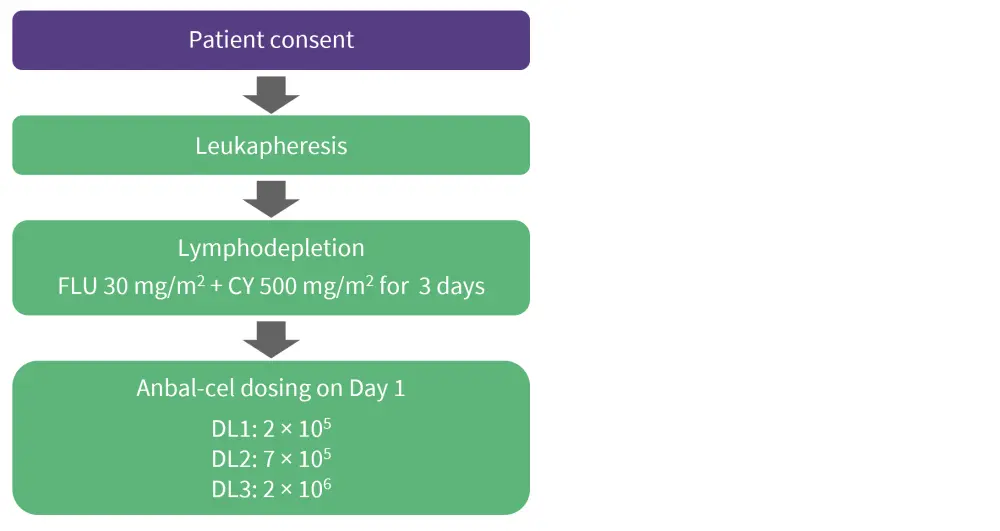
Anbal-cel, anbalcabtagene autoleucel; CY, cyclophosphamide; DL, dosing level; FLU, fludarabine.
*Adapted from Kim.2
Results
Baseline characteristics
The baseline characteristics for the 11 patients treated in this study are highlighted in Table 3.
Table 3. Baseline characteristics for patients infused with anbal-cel*
|
anbal-cel, anbalcabtagene autoleucel; ASCT, autologous stem cell transplantation; DLBCL, diffuse large B-cell lymphoma; ECOG, Eastern Cooperative Oncology Group; GCB, germinal center B-cell; SPD, sum of the product of diameters; tFL, transformed follicular lymphoma. |
|
|
Characteristic, % (unless otherwise stated) |
All patients (N = 11) |
|---|---|
|
Median age (range), years |
46 (26–71) |
|
≥65 |
4 (36) |
|
Male |
55 |
|
ECOG Performance Status 1 |
36 |
|
Disease subtype |
|
|
DLBCL |
91 |
|
tFL |
9 |
|
Cell of origin of cancer |
|
|
GCB |
55 |
|
Non-GCB |
45 |
|
Double expressor type |
45 |
|
Previous line of therapy |
|
|
1/2 |
36 |
|
3 |
27 |
|
≥4 |
36 |
|
Refractory to last line of therapy |
73 |
|
Previous ASCT |
36 |
|
Refractory to 1st line of therapy |
55 |
|
median SPD (range), mm2 |
3,520 (570–7,719) |
|
≥5,000 mm2 |
45 |
Safety and efficacy
Of the 11 evaluable patients, five (46%) experienced CRS; two patients with Grade 1, one patient with Grade 2, and two patients with Grade 3. Most of the treatment-emergent adverse events were observed at the higher dose, DL3. The most common adverse events across all doses were CRS (46%), anemia (18%), neutropenia (18%), fever (18%), and thrombocytopenia (18%; Table 4). The onset of CRS was delayed, occurring at 7 days, and had a median duration of 5 days. Only one patient experienced a Grade 2 neurological event at DL3, this patient also had CRS and was therefore treated with both tocilizumab and steroids.
Tmax were 15.4, 15.8, and 11 days at DL1, DL2, and DL3, respectively, which is slightly delayed when compared to other CAR T-cell therapies. There was a dose-dependent drug expansion observed where area under the curve (AUC) and Cmax proportionally increased with dose of anbal-cel. AUC at Day 0–28 was 679,125, 1,110,108, and 2,852,235 copies/ug gDNA at DL1, DL2, and DL3, respectively. Median Cmax was 18,003, 30,103, and 53,688 copies/ug gDNA at DL1, DL2, and DL3.
All patients who responded to treatment achieved a CR across all dose levels, with an overall ORR and CR of 82%. Both ORR and CR were 75%, 67%, and 100% at DL1, DL2, and DL3, respectively. For CR patients at DL1 and DL2, these responses were durable.
Table 4. TRAE’s for patients treated with anbal-cel*
|
anbal cel, anbalcabtagene autoleucel; CRS, cytokine release syndrome; DIC, disseminated intravascular coagulation; ICANS, immune-effector cell-associated neurotoxicity syndrome; n/a, not applicable; TRAE, treatment-related adverse event. |
||||
|
TRAE any grade, % |
2 × 105 cells/kg |
7 × 105 cells/kg |
2 × 106 cells/kg |
Total |
|---|---|---|---|---|
|
CRS |
|
|
|
|
|
Incidence |
0 |
100 |
50 |
46 |
|
Median onset |
n/a |
7 (6–11) |
8.5 (1–16) |
7 (1–16) |
|
Median duration |
n/a |
2 (1–5) |
16.5 (14–19) |
5 (1–19) |
|
Anemia |
0 |
0 |
50 |
18 |
|
Neutropenia |
0 |
0 |
50 |
18 |
|
Fever |
25 |
0 |
25 |
18 |
|
Thrombocytopenia |
0 |
0 |
50 |
18 |
|
DIC |
0 |
0 |
25 |
9 |
|
Herpes |
0 |
33 |
0 |
9 |
|
Hypogammaglobulinemia |
0 |
0 |
25 |
9 |
|
ICANS |
0 |
0 |
25 |
9 |
|
Rash |
0 |
0 |
25 |
9 |
|
Sepsis |
0 |
0 |
25 |
9 |
|
Neurological events |
|
|
|
|
|
Incidence |
0 |
0 |
25 |
9 |
|
Median onset, |
n/a |
n/a |
7 |
7 |
|
Median duration, |
n/a |
n/a |
13 |
13 |
Figure 4. Response rates in patients infused with anbal-cel*
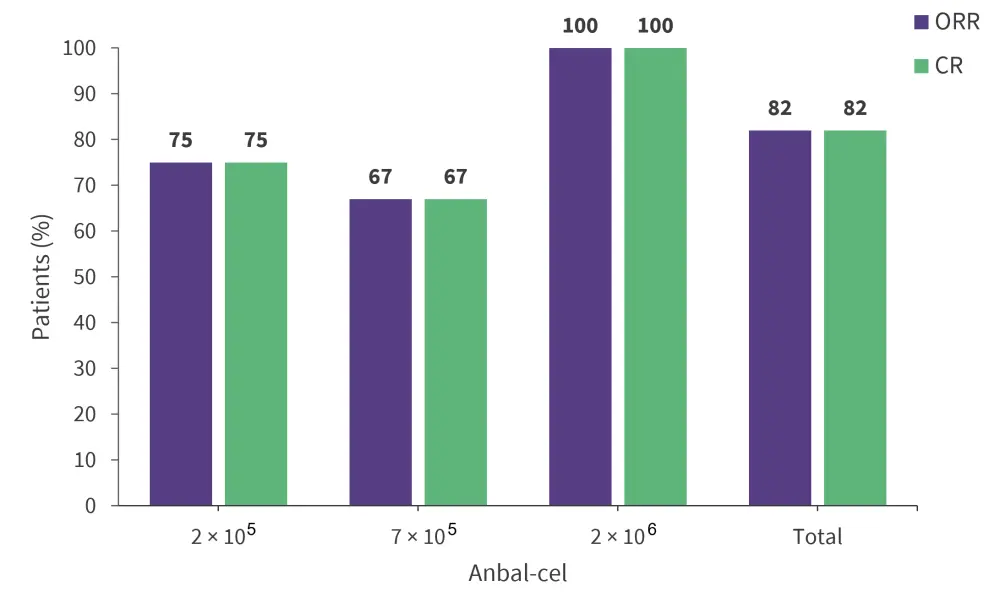
anbal-cel, anbalcabtagene autoleucel; CR, complete response; ORR, overall response rate.
*Data from Kim.2
Phase I, open-label study evaluating the clinical activity of CC-99282, a cereblon E3 ligase modulator agent, in patients with R/R NHL
CC-99282, a small cereblon E3 ligase modulator agent, targets the degradation of two transcription factors, Ikaros and Aiolos, which are important for B-cell development and differentiation. CC-99282 has shown antiproliferative and apoptotic activity in large B-cell lymphoma (LBCL) cell lines and this first-in-human study explores its safety and efficacy in a clinical setting.
Study design
This is a multicenter, open-label study consisting of two parts: a dose escalation of CC-99282 monotherapy and a dose expansion with and without combination partners. This report focuses on the dose escalation results. Eligible patients were those with R/R DLBCL or follicular lymphoma who progressed after two or more lines of therapy, and patients with R/R DLBCL who received one or more line of therapy and were also unfit for chemotherapy or transplant. Patients received CC‑99282 at an oral dose of 0.2, 0.4, 0.6, or 0.8 mg once daily in three intermittent dosing schedules of 28-day cycles: a 5/7 days schedule (5 days on/2 days off), a 7/14 days schedule (7 days on/7 days off), and a 14/28 days schedule (14 days on/14 days off).
The primary endpoints were safety and tolerability to determine MTD and the recommended phase 2 dose. The secondary endpoints were pharmacokinetics and preliminary efficacy.
Results
Baseline characteristics
The baseline characteristics for patients are summarized in Table 5.
Table 5. Baseline characteristics for patients treated with CC-99282*
|
CAR, chimeric antigen receptor; DLBCL, diffuse large B-cell lymphoma; ECOG, Eastern Cooperative Oncology Group; FL, follicular lymphoma; NOS, not otherwise specified. |
|
|
Characteristic, % (unless otherwise stated) |
All patients (N = 50) |
|---|---|
|
Median age (range), years |
65.5 (35–89) |
|
Male |
58 |
|
Diagnosis |
|
|
DLBCL |
76 |
|
NOS |
44 |
|
Double- or triple-hit positive |
14 |
|
Transformed |
32 |
|
FL (Grade 1–3B) |
24 |
|
Median time from initial diagnosis to first dose |
|
|
DLBCL |
22.5 (4.5–94.5) |
|
FL |
71.8 (22.5–135.9) |
|
ECOG Performance Status |
|
|
0 |
42 |
|
1 |
50 |
|
2 |
8 |
|
Stage IV cancer at diagnosis |
58 |
|
Treatment history |
|
|
Median prior lines of therapy (range), n |
3 (1–8) |
|
Prior stem cell transplant |
20 |
|
Prior CAR T-cell therapy |
28 |
|
Prior lenalidomide/avadomide |
22 |
|
Refractory to last regimen |
50 |
Safety and efficacy
A total of 32 patients reported a Grade 3/4 treatment-related adverse event. The most common were neutropenia (58%), thrombocytopenia (8%), and anemia (8%; Figure 5). No patients discontinued treatment because of neutropenia. The high incidence of severe neutropenia was found to be strongly related with the number of prior lines of alkylating agent and not related to CC-99282. Neutropenia was managed with dose modifications of CC-99282 and granulocyte colony stimulating factors. All DLTs were hematologic, mostly caused by neutropenia, and MTDs of interest were 0.6 mg and 0.4 mg during the 7/14-day schedule and the 14/28-day schedule, respectively. Eight patients (16%) reported serious adverse events related to CC-99282, including 4 patients (8%) with febrile neutropenia.
ORR was 42% at the dose of interest (0.4 mg), CR and partial response was achieved in 17% and 25%, respectively. Durable responses were observed at the dose of interest and above in patients with initial partial response converting to a CR. Median DOR was 239 days and median follow-up was 247 days at the 7/14 days schedule. For the 14/28 days schedule, the median DOR and median follow-up were 112 days and 121 days, respectively.
In terms of pharmacokinetics, there was dose-dependent activity of CC-99282, with an increase in plasma CC-99282 and degradation of transcription factors Ikaros/Aiolos in peripheral T cells, as the dosage increased. A shift of peripheral CD8+ cells to an activated phenotype, and a shift of CD8+ naïve cells to a memory T-cell phenotype was observed within 2 weeks of initiating CC-99282, which supports the immune-stimulation of the study drug. A reduction in ctDNA after treatment with CC-99282 was also observed, which could suggest strong tumor cell-intrinsic activity.
Figure 5. TEAEs related to CC-99282*
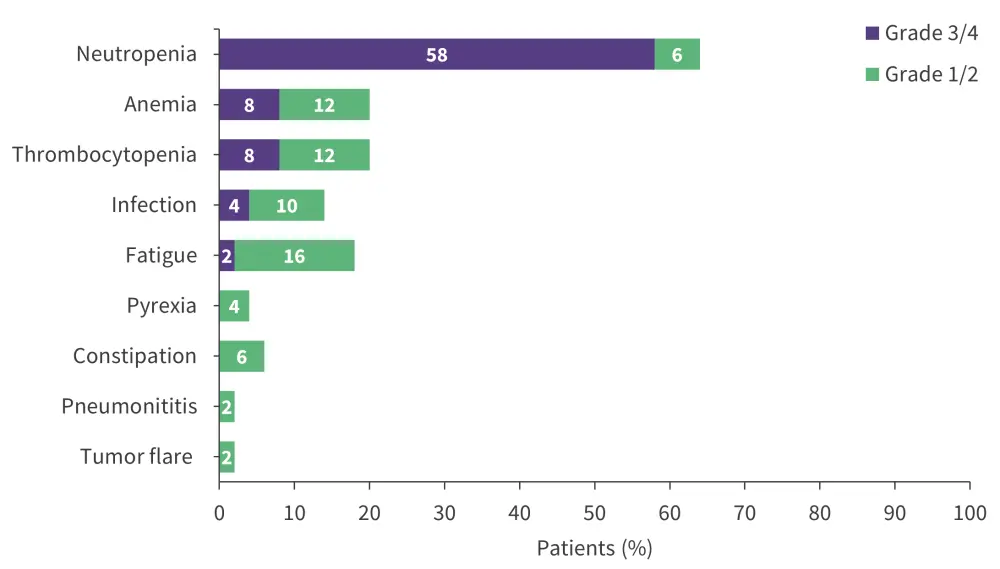
TEAE, treatment-emergent adverse events.
*Data from Michot.3
Conclusion
These results demonstrate the promising efficacy of emerging novel CAR T-cell therapies and small molecule agents in patients with aggressive NHL. YTB323, a CAR T-cell therapy with a next-generation manufacturing method, anbal-cel, a novel anti-CD19 CAR T-cell therapy with dual silencing of PD-1 and TIGIT, and CC-99282, a cereblon E3 ligase modulator agent, all produced a favorable safety profile and therefore could offer new treatment options for patients with R/R B-cell NHL.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content