All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ESMO 2016 | Educational Session – MZL: Recent Developments in Diagnostics and Therapeutics
Professor Catherine Thieblemont from the Hôpital Saint-Louis in Paris, France, presented an educational session on the latest developments in diagnostics and therapeutics in Marginal Zone Lymphoma (MZL) during the ESMO congress in October 2016 in Copenhagen, Denmark. MZL affects 17% of adults with lymphoma and is the second most frequent lymphoma in patients over 80 years old, making up 30% of cases.
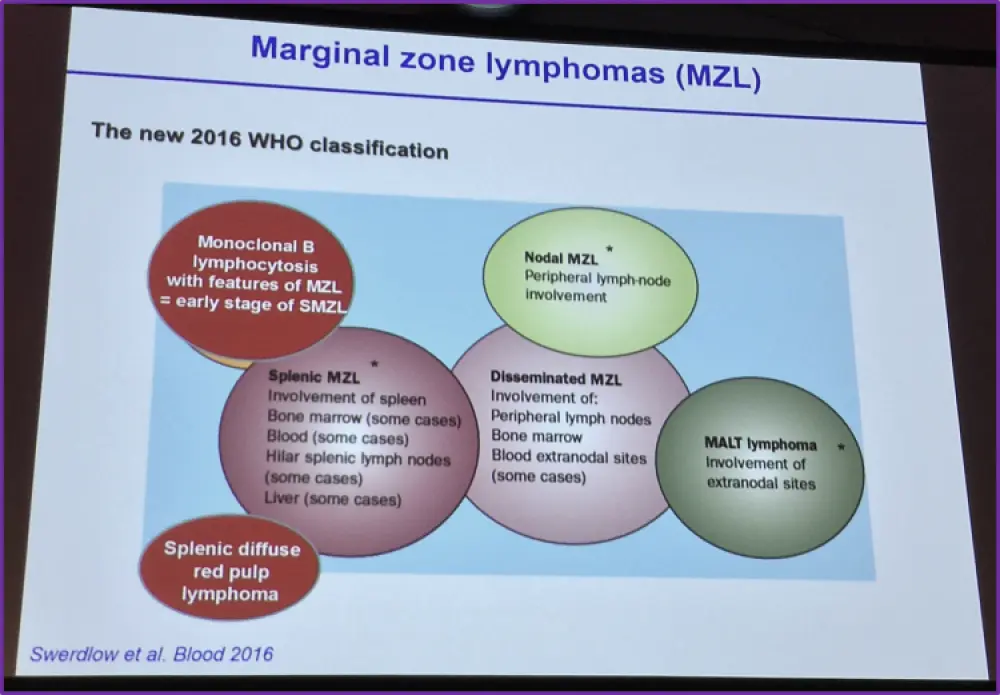
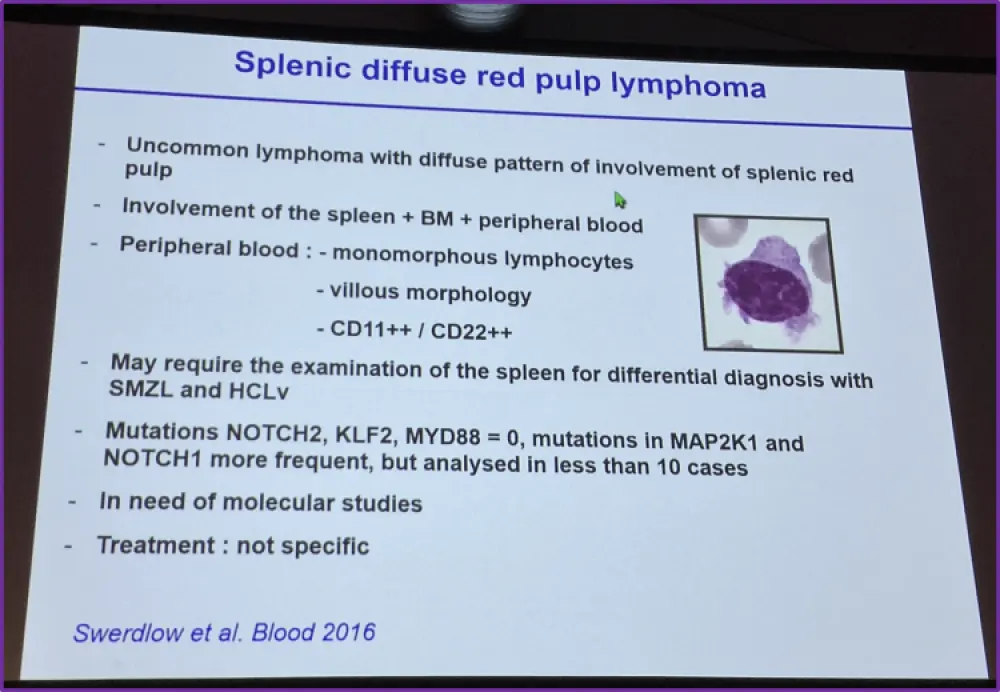
The session began with an update on the WHO classification of MZL sub-types, published in 2016, displayed below. The key changes since the 2008 classification were the classification of monoclonal B-cell lymphocytosis with features of MZL and the addition of splenic diffuse red pulp lymphoma. Splenic diffuse red pulp lymphoma was subsequently detailed.
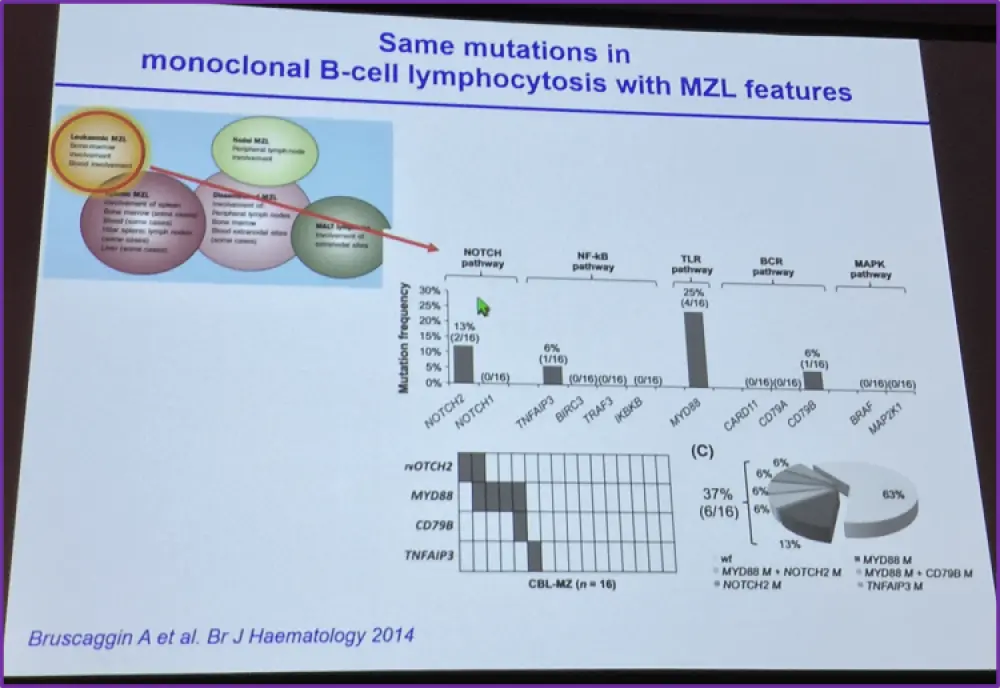
Data was presented that showed that the subtypes of MZL share common signaling pathways, for example SMZL, NMZL, MALT lymphoma and monoclonal B-cell lymphocytosis share a higher frequency of mutations in the NFkB pathway. SMZL, NMZL and monoclonal B-cell lymphocytosis also share increased mutation frequency in NOTCH, TLR (MYD88) and BCR pathways.
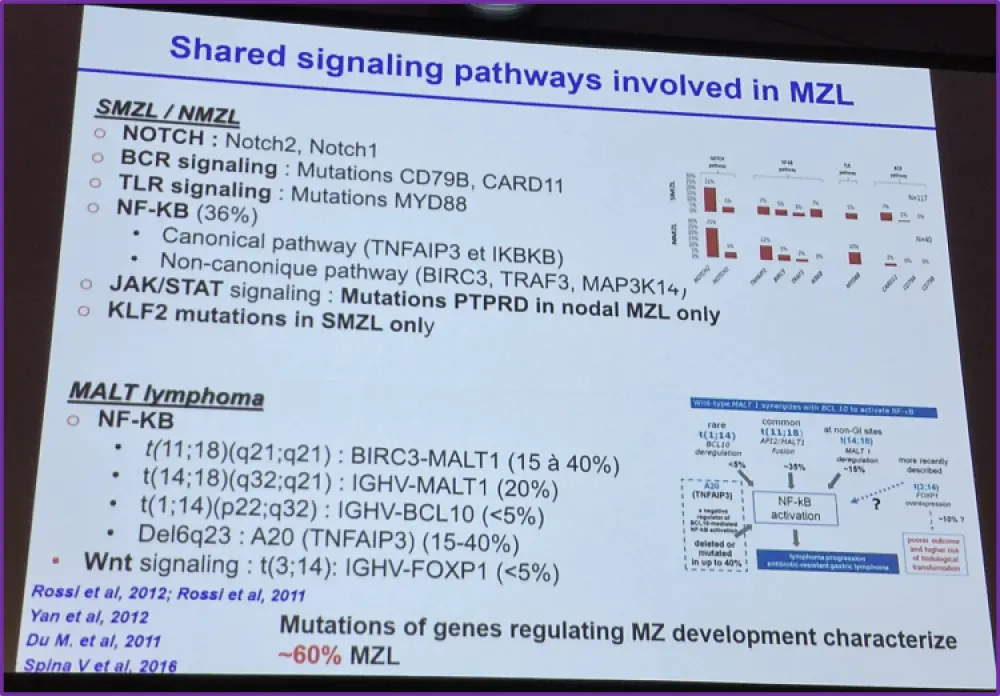
Proteins in the pathways involved in cell survival and actin remodeling were suggested as potential new drug targets including NOTCH, TLR and BCR. Most of these target pathways are involved with NFkB signaling. JAK/STAT signaling has also been implicated.
Currently, there is no standard treatment for the different MZL subtypes and Professor Thieblemont summarized the current approaches to treatment, shown below.
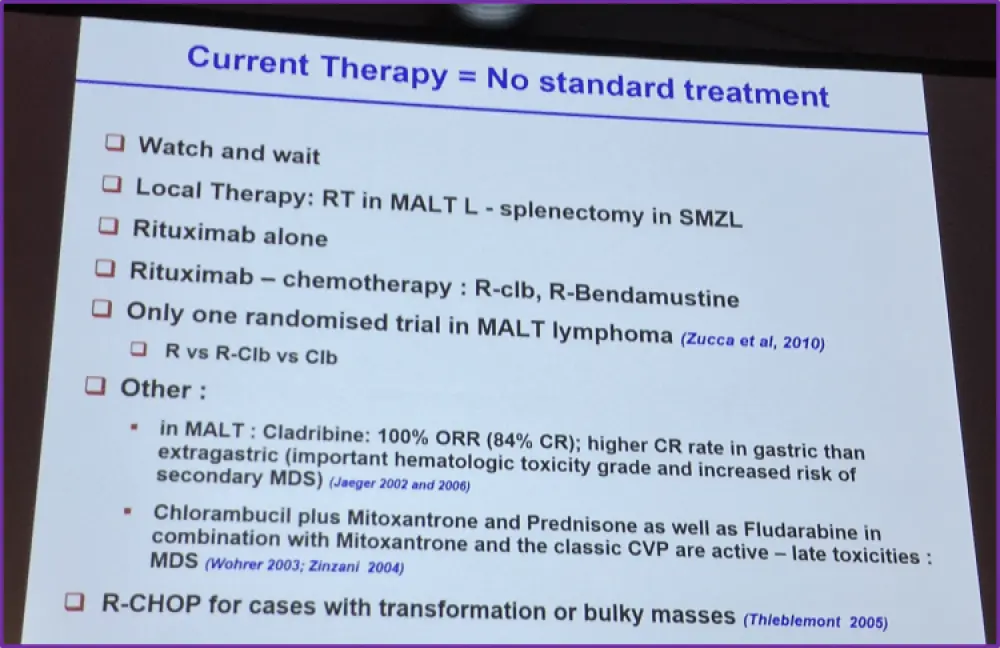
In cases of MALT lymphoma non-dependent to a pathogen, there are multiple therapeutic options, which were discussed during the session. For stage I and II, these were radiation (30Gy), rituximab (R) and R-alkylant. For stage III-IV, the options were only R-alkylant and R. Results from multiple trials performed in MALT lymphoma were also presented, shown below.
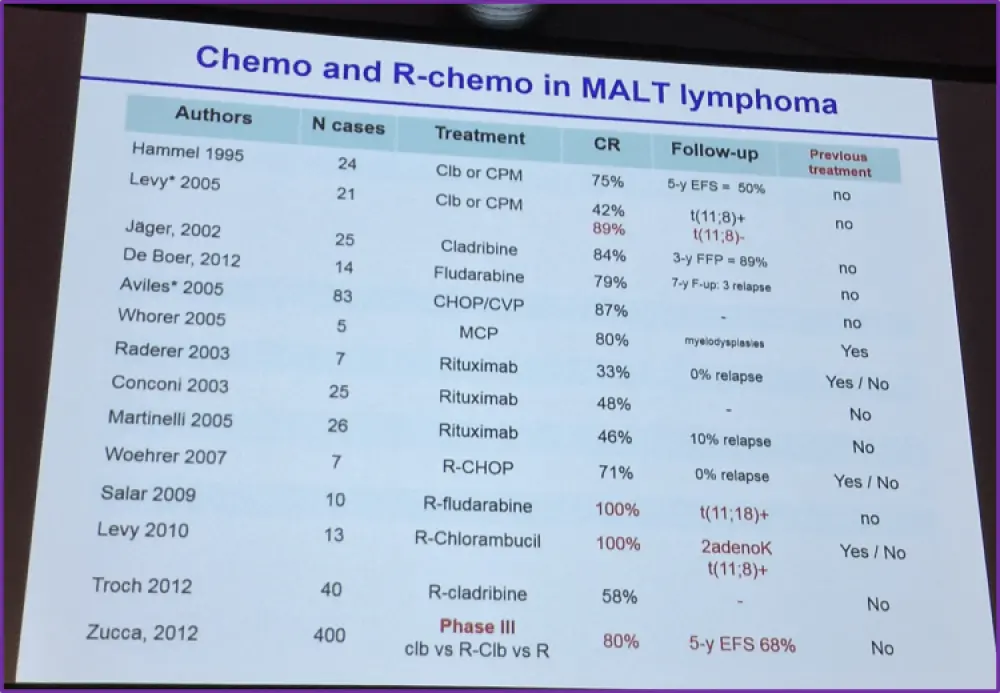
Furthermore, results of the IELSG-19 randomized trial by Zucca et al. (Lugano ICML 2013) compared the efficacy of R-chlorambucil, chlorambucil alone and R alone in the treatment of MALT lymphoma. Results showed that R-chlorambucil and chlorambucil alone treatment resulted in significantly higher CR than R alone. R-chlorambucil had a higher CR and ORR than chlorambucil alone. R-chlorambucil also had a significantly higher EFS and PFS at 60 months. Additionally, R-bendamustine was shown by Salar (Lancet Haematology 2014) in patients with MALT lymphoma to achieve a 3-year EFS of ~84% and, after 3-cycles, a CRR of 75%.
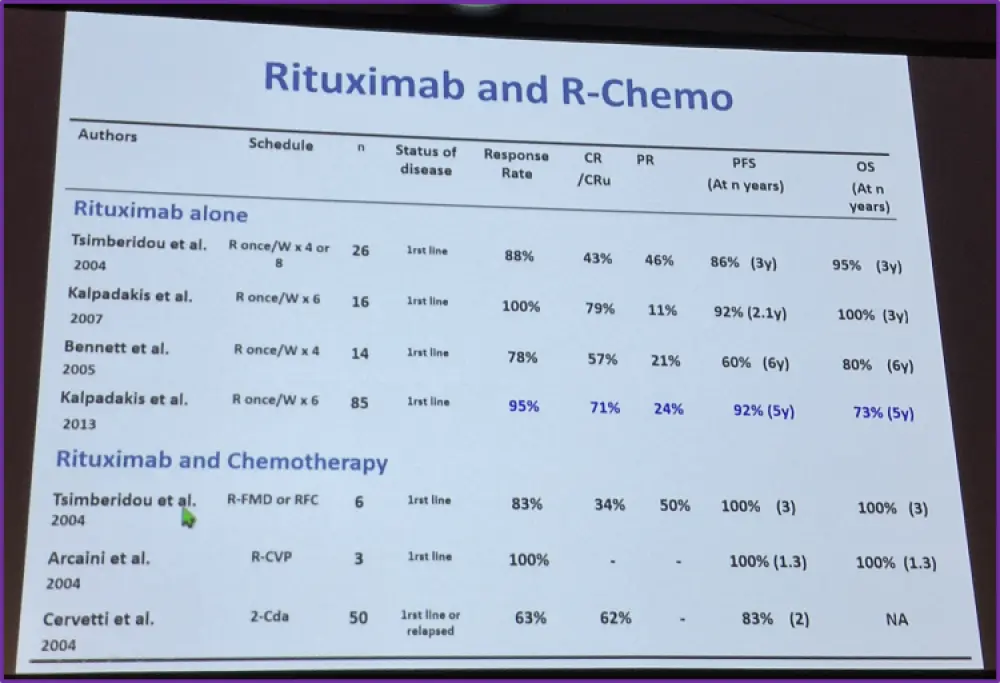
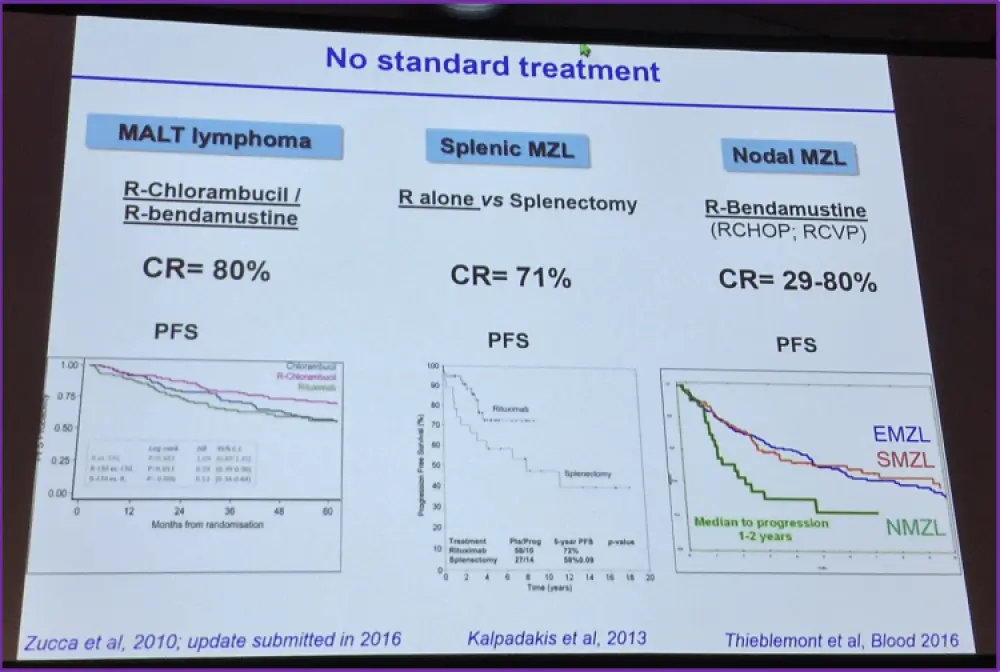
The main therapeutic options for SMZL were presented as being splenectomy, chemotherapy, R or combined R-chemotherapy. Each of these options was then discussed in turn by Professor Thieblemont. Splenectomy was shown to result in correction of cytopenias and a reduction in bone marrow infiltration with a median treatment time of longer than 8 years. 5-year PFS and OS following splenectomy in a trial of 100 SMZL patients were shown to be 61% and 84%, respectively, with 10-year PFS and OS being 46% and 67%, respectively (Lenglet J. et al. Leukemia & Lymphoma, 2013). Chemotherapy after splenectomy has not been shown to be beneficial, however it may be necessary in high-grade lymphoma in cases of transformation. A summary of trials conducted on the efficacy of R and R-chemotherapy were presented, shown below.
A large prospective trial was discussed which is studying the efficacy (CR rate) of R-bendamustine treatment in symptomatic SMZL patients who either were not able/willing to undergo splenectomy or had undergone a splenectomy but were quickly progressing. This ‘Benda-Rituximab in symptomatic patients with Splenic Marginal Zone Lymphoma’ (IELSG 36-BRISMA) study is expected to have complete analysis by the end of 2017.
In summary, there is no standard treatment for MALT lymphoma, SMZL or NMZL, with NMZL currently being treated similarly to FL.
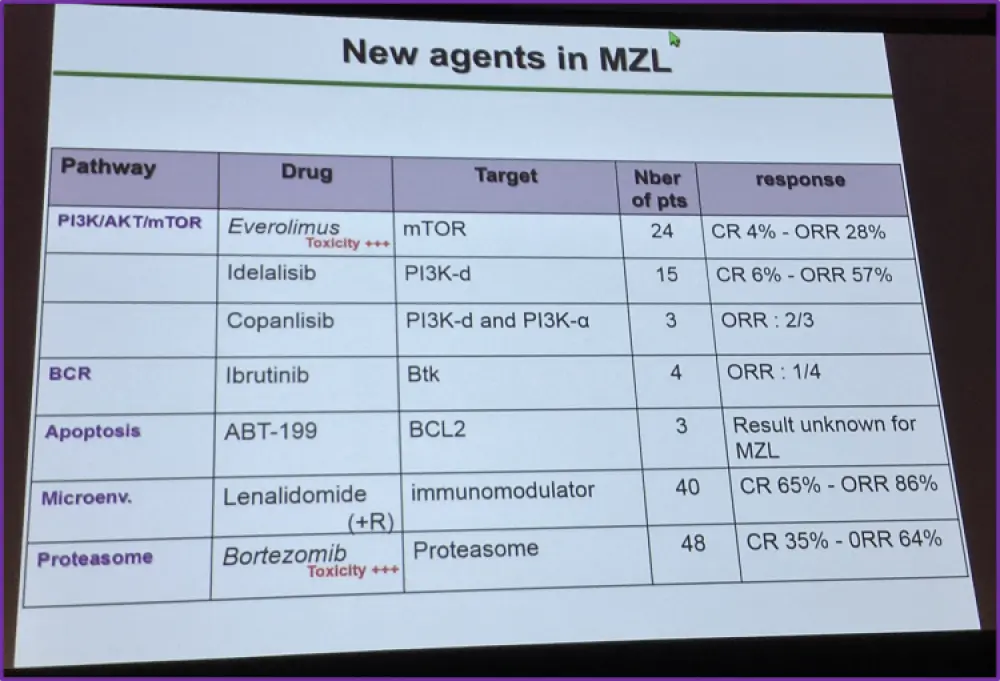
Finally, Professor Thieblemont gave an overview of the potential new agents for treating MZL, which are currently being explored, and data from a review examining the efficacy of combination therapies in the treatment of MZL (Thieblemont et al. Blood, 2016).
Take home messages from this talk are listed below:
- Heterogeneous disease with a specific physiopathology
- No standard treatment
- CLINICAL TRIAL!!
- New drugs
- Inhibitors of signalling pathways: TLR, BCR, NOTCH, NFkB, Jas/stat
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?