All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ESMO 2016 | Multidisciplinary Cases Session: Treatment regimens in Primary Central Nervous System (CNS) Lymphoma
Dr Francesc Graus from the Neurology Service Hospital Clinic, Barcelona, Spain, presented a session based on results from a range of multidisciplinary studies focused on identifying optimal treatment regimens for patients with Primary Central Nervous System Lymphoma (PCNSL) at the ESMO congress 2016, at Copenhagen, Denmark.
Dr Graus discussed, through the presentation of the case studied, the main questions raised for the treatment of a primary CNS lymphoma.
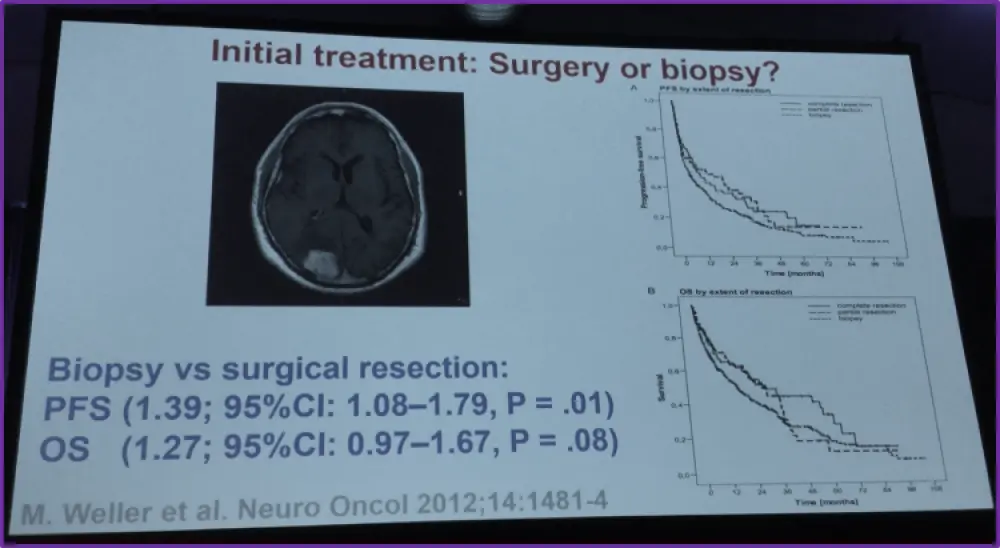
- The first question concerned the choice between biopsy and surgical resection. Dr Graus presented the secondary analysis of the German PCNSL Study Group-1 trial. The data obtained showed that the Progression Free Survival (PFS; HR of 1.39) and the Overall Survival (OS; HR of 1.27) favored the surgical resection.
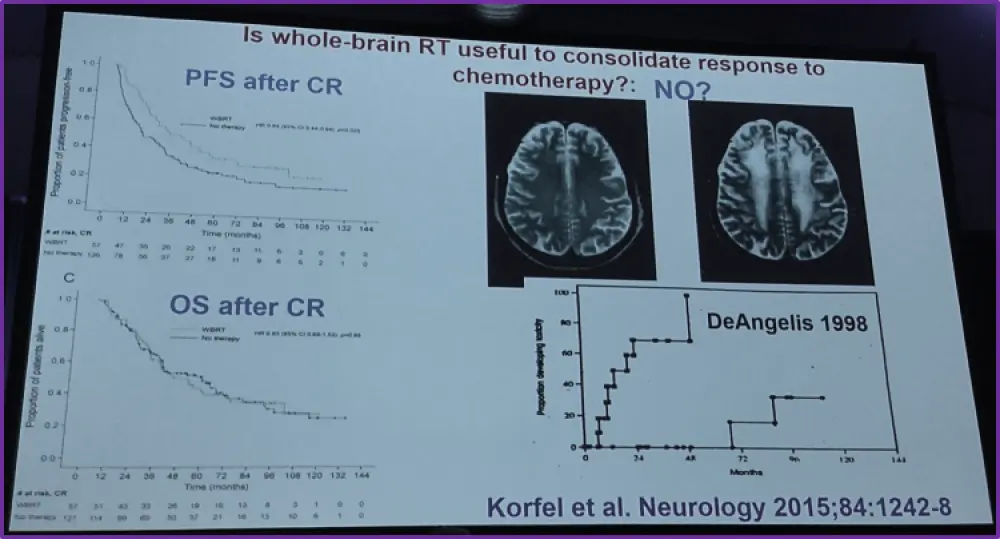
- The second question focused on the place of WBRT as consolidation. To demonstrate this point, Dr Graus used the German retrospective study published by Korfel et al. with a median follow-up of 81.2 months. The omission of WBRT for patients in CR after high-dose methotrexate (HDMTX) does not worsen OS.
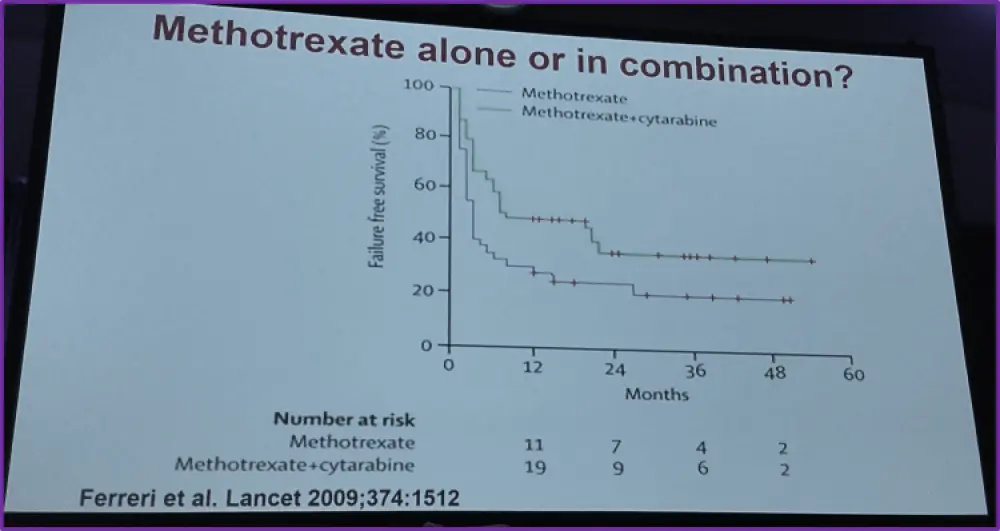
- The next question concerned the use of HDMTX alone or in combination with high-dose cytarabine. He presented an international phase II trial published by Ferreri et al. showing that adding HD cytarabine to HDMTX improved outcome.
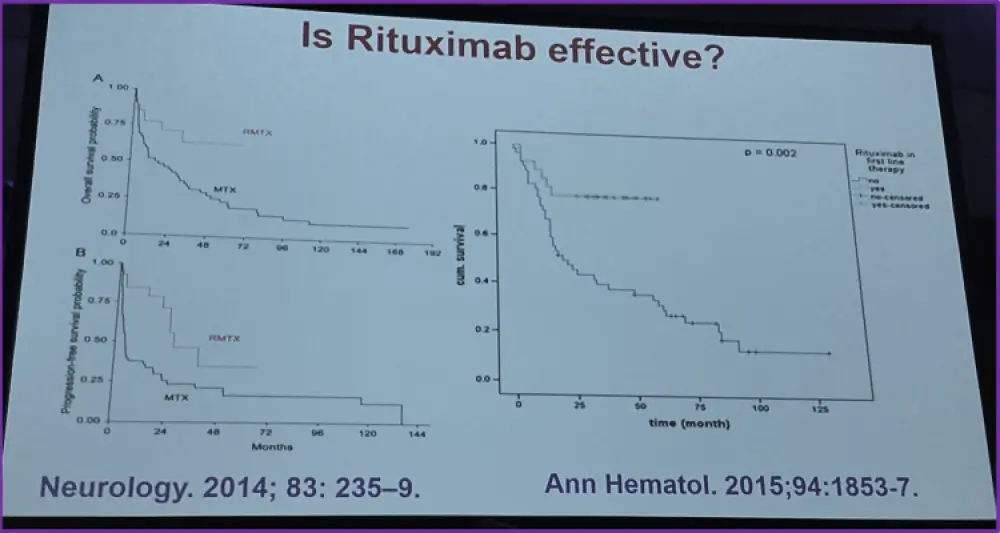
- Then Dr Graus questioned the efficiency of adding rituximab to HDMTX. To illustrate this point, he chose 2 trials. The first one, from the John Hopkins Hospital, demonstrated in a randomized phase II trial that the addition of rituximab to HDMTX in newly diagnosed immunocompetent PCNSL patients improved CRR, PFS and OS. The data obtained showed that the median OS in patients treated with MTX alone was 16.3 months and was not reached in patients treated with MTX plus rituximab. This finding was confirmed in a retrospective study on 81 PCNSL patients where the addition of rituximab to HDMTX improved significantly the 3-year OS (77.8% vs 39.9%).
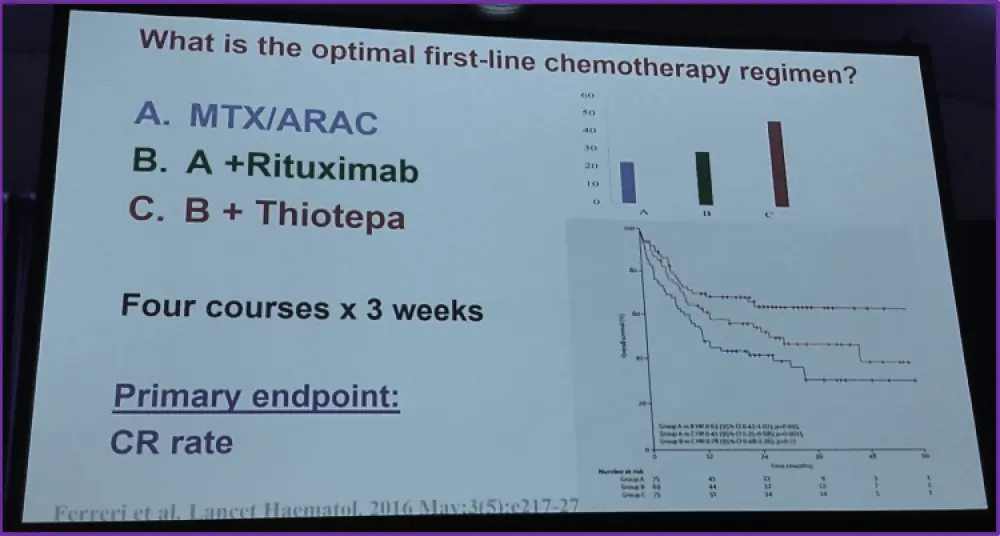
The role of chemoimmunotherapy was confirmed by the IELSG phase 2 trial published recently by Ferreri et al. in the Lancet Hematology. 219 PCNSL patients were given either MTX/cytarabine alone or in combination with rituximab, or rituximab and thiotepa. The primary outcome of this trial was to compare the complete response of participants to the different treatment regimes. The trial results showed that patients treated with rituximab plus thiotepa had a CRR of 49% compared with 23% for MTX/cytarabine alone and 30% for MTX/cytarabine/rituximab.
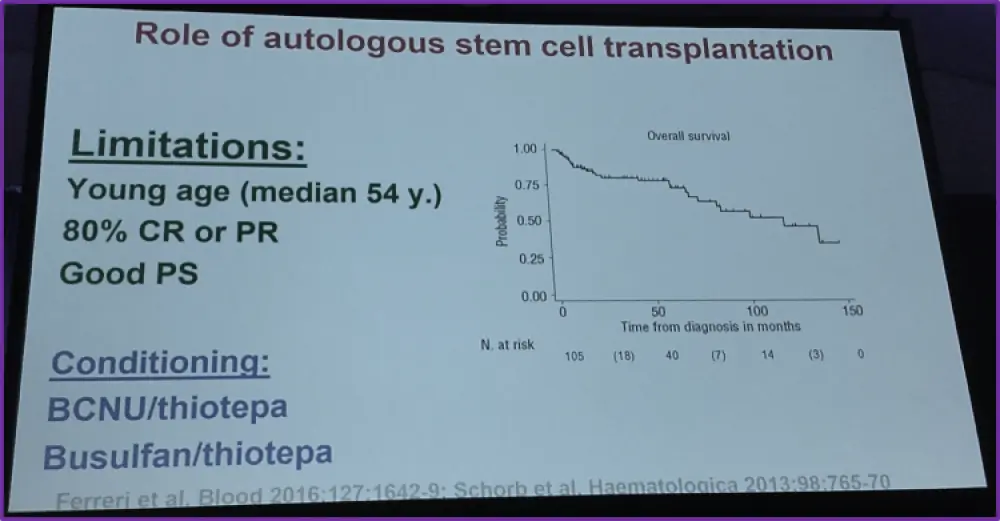
- One more question concerned the role of Autologous Stem Cell Transplantation (ASCT). A retrospective study investigated the survival rates of PCNSL patients who were treated with HD chemotherapy followed by ASCT. The results of this study indicate that HD chemotherapy followed by ASCT leads to increased OS (median = 121 months) rate. However, these data are limited to patients of a relatively young age (median = 54 years) and either good PS or with an 80% CRR.
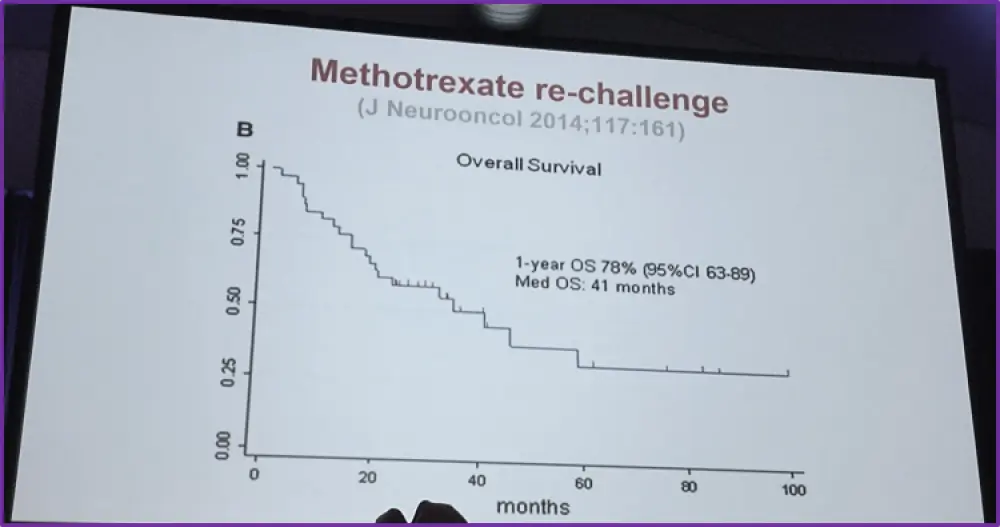
Finally, the question of treatment options for PCNSL relapses was raised. One study with a primary outcome to investigate MTX re-challenge to 39 PCNSL patients who responded previously to MTX therapy and experienced relapse was presented. The trial data revealed that the 1-year OS was 79% and the median OS was 41 months, thus suggesting MTX re-challenge is effective in relapsed PCNSL patients.
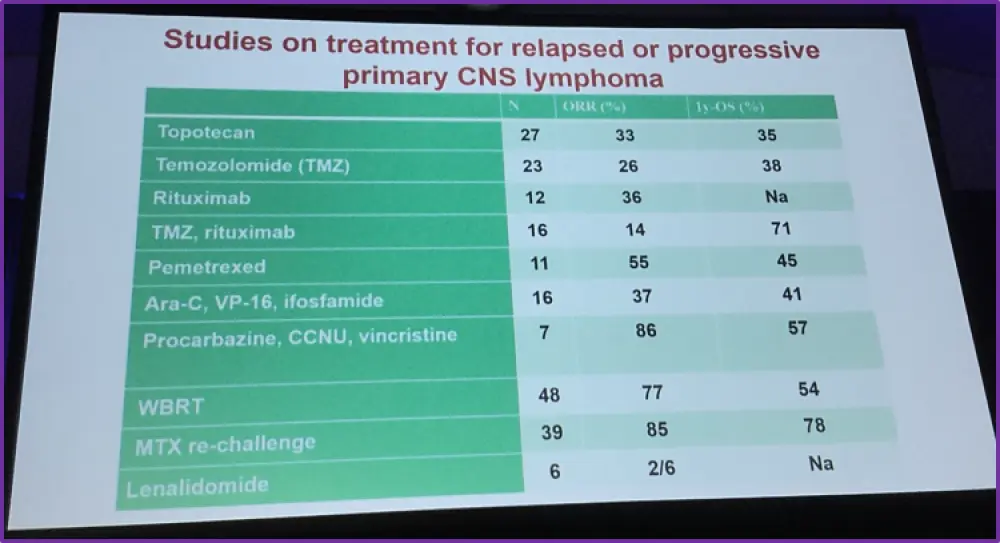
On-going clinical trials are underway for patients with either relapsed or progressive PCNSL using different therapeutic agents and the results in terms of OS are promising.
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?