All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ESMO 2016 | Selected Oral Presentations: PMLBL: R-DA-EPOCH or R-CHOP? Which is a more effective treatment?
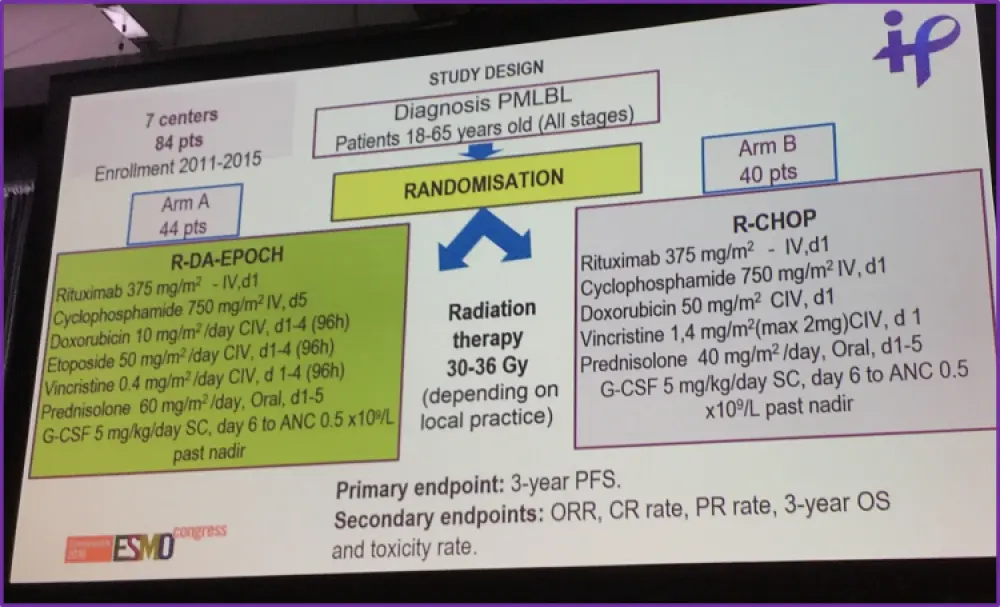
Dr Iryna Kryachok from the National Cancer Institute of the MPH Ukraine, in Kiev, Ukraine, and colleagues presented during the ESMO congress in October 2016 in Copenhagen, Denmark, the results of a prospective study comparing two different treatment regimens for PMLBL.
The aim of the study was to provide the first data from a large prospective study comparing two immunochemotherapy regimens for PMLBL, R-DA-EPOCH and R-CHOP, in order to determine which first-line therapy is the most effective and tolerable. The primary endpoint was 3-year PFS, with secondary endpoints being 3-year OS, ORR, CR, PR, and toxicity.
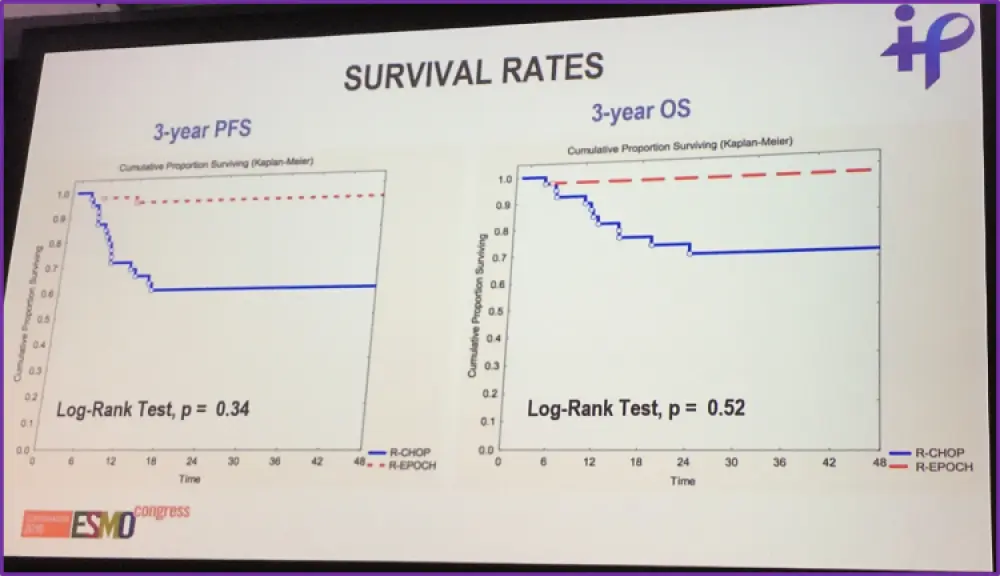
Data presented showed that PFS rates after 3-years were significantly higher in patients following treatment with R-DA-EPOCH (96%) than R-CHOP (60%). OS rates were higher in the R-DA-EPOCH group (97.7% vs 70% R-CHOP), although this was not significant.
Reported data on the secondary endpoints of the study showed that R-DA-EPOCH had significantly higher ORR than R-CHOP (97.7% vs 85% (P<0.05)) and CR (81.8% vs 50% (P<0.01)). R-DA-EPOCH also had significantly lower relapse rate and PD than R-CHOP.
| Response an survival | R-DA-EPOCH | R-CHOP | p |
|---|---|---|---|
| ORR, No (%) | 43 (97.7) | 34 (85.0) | <0.05 |
| CR, No (%) | 36 (81.8) | 20 (50) | <0.01 |
| PR, No (%) | 7 (15.9) | 13 (32.5) | >0.05 |
| SD, No (%) | 0 (0) | 1 (2.5) | >0.05 |
| PD, No (%) | 1 (2.3) | 6 (15) | <0.05 |
| Relapse, No (%) | 0 (0) | 6 (15) | <0.05 |
| 3-year PFS, % | 96 | 60 | 0.034 |
| 3-year OS, % | 97.7 | 70 | 0.052 |
The main difference between R-DA-EPOCH and R-CHOP in terms of toxicity were found to be anemia, grade 3-4 neutropenia, and neurologic grade 1-2 with sensory effects (R-DA-EPOCH = 54.5%, R-CHOP 25%, P<0.05).
| Toxicity type | R-DA-EPOCH (264 cycles) | R-CHOP (240 cycles) | p |
|---|---|---|---|
|
Anemia, No of cycles (%) Grade 3-4, No of cycles (%) |
173 (65.5) 32 (12.1) |
115 (47.9) 21 (8.8) |
<0.05 >0.05 |
|
Neutropenia, No of cycles (%) Grade 3-4, No of cycles (%) |
169 (64) 96 (36.4) |
132 (55) 49 (20.4) |
>0.05 <0.05 |
|
Thrombocytopenia, No of cycles (%) Grade 3-4, No of cycles (%) |
61 (23.1) 0 (0) |
41 (17.1) 0 (0) |
>0.05 |
| Febrile neutropenia, No of cycles (%) | 29 (10.9) | 30 (12.5) | >0.05 |
| Death due to toxicity, No of patients (%) | 0 (0) | 0 (0) |
The main conclusion from this presentation was that in patients with PMLBL, R-DA-EPOCH had a significantly higher efficacy than R-CHOP with a significantly lower rate of relapse and PD. R-DA-EPOCH also had a significantly higher OS and PFS than R-CHOP, but R-DA-EPOCH treatment came with higher levels of hematological toxicity and neurologic sensory effects. It was suggested that a longer follow up period is required in order to confirm their findings.
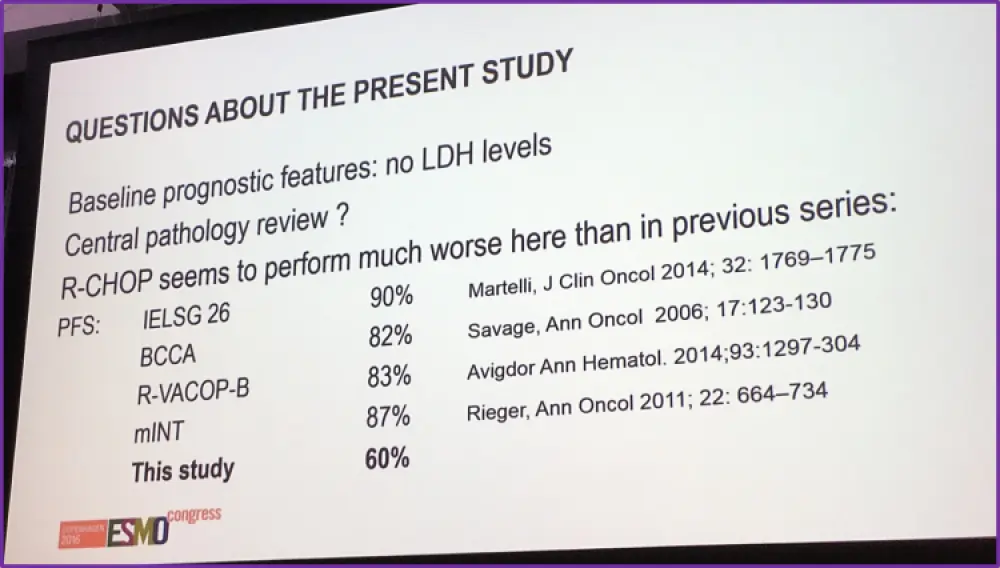
In the subsequent discussion session, chaired by Prof. Peter Johnson, some potential issues and areas of concern were raised. These included the absence of central pathology review, the absence of prognostic markers, such as LDH levels, at baseline, and R-CHOP PFS rates being lower than that seen in four other published articles since 2006. He concluded by stating that care is needed in the interpretation of this data and that the standard of care for PMBL remains R-CHOP+/-IFRT or DA-R-EPOCH. A prospective trial (IELSG 37) is testing the use of FDG-PET post-chemotherapy to determine whether IFRT can be omitted in good responders.
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?