All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Follicular lymphoma: A summary of the hot topics presented at the 63rd American Society of Hematology Annual Meeting and Exposition
Introduction
Follicular lymphoma (FL), a form of non-Hodgkin lymphoma, is an indolent but incurable lymphoproliferative disorder of mature B cells which is characterized by diffuse lymphadenopathy, splenomegaly, and bone marrow (BM) involvement.1 FL is associated with recurrent relapses and reduced progression-free survival (PFS) intervals with each line of conventional treatment, as well as potential transformation to a more aggressive histology.2,3
This article summarizes the hot topics presented at the 63rd American Society of Hematology (ASH) Annual Meeting and Exposition regarding FL, including single-cell profiling, practice changing research on disease monitoring, alternative first line treatment options, and promising therapies in development.
Developments in disease biology: single-cell profiling in FL to identify at-risk patients
Developments in our understanding of underlying disease pathophysiology may pave the way for tailored treatment strategies. Wang, et al.2 hypothesized that the variable clinical outcomes of FL may in part be due to clonal heterogenicity and patient-specific immune responses, and thus understanding the complex tumor ‘ecosystem’ could allow for treatment to be individualized to each patient.
Their previous analysis of B- and T-cell‒focused phenotypic profiling at single cell resolution by mass cytometry (CyTOF) of 155 newly diagnosed pretreatment FL biopsy samples revealed two distinct evolutional trajectories (independently reflected in both B- and T-cell compartments), one involving germinal center B cells, and another related to naïve/memory B cells. These trajectories were found to be mutually exclusive and tended not to be found within the same tumor.
In further analysis, following incorporation of DNA mutational information and clinical outcomes, tumors were grouped based on the phenotype of the majority of tumor cells present, type A tumors dominated by germinal center B cells (28%), type B tumors by naïve/memory B cells (18%) and type nonA/nonB tumors dominated by neither (54%).
Mutations in EZH2, TNFRSF14, and MEF2B were significantly enriched in type A tumors. Type B tumors with a high measure of intratumoral phenotypic diversity, or “entropy”, were significantly associated with transformation risk, and type B tumors with above median entropy exhibited a hazard ratio (HR) of 5.9 for transformation risk compared to all other tumor types combined. Multivariate analysis found type B tumors and high entropy remained significant risk factors for transformation (p = 0.043 and p = 0.011, respectively), whilst high Follicular Lymphoma International Prognostic Index (FLIPI) score was not identified as a significant risk factor (p = 0.962).
In a sub-cohort of 108 patients who had received bendamustine and rituximab as primary therapy, type nonA/nonB tumors had the poorest disease specific survival (DSS) outcomes compared with all other tumor types combined (5 year survival, 78% vs 98%; log-rank p = 0.0241). This tumor type combined with high entropy revealed significantly reduced DSS (HR, 5.3; log-rank p = 0.0019). In multivariate analysis, tumor type nonA/nonB and high risk FLIPI score were significant risk factors for reduced DSS (p = 0.038 and p = 0.035, respectively), and high entropy trended towards reduced DSS, but did not reach statistical significance.
The findings of Wang et al. support the use of CyTOF-defined phenotypic subtypes of FL and measurement of intratumoral phenotypic diversity to identify—at diagnosis—patient subgroups at increased risk of disease transformation and inferior survival outcomes.
Practice changing developments in FL: MRD monitoring (results from the FIL FOLL12 trial)
The Fondazione Italiana Linfomi (FIL) FOLL12 study was a prospective, phase III, randomized clinical trial comparing rituximab maintenance with a combined positron emission tomography/minimal residual disease (PET/MRD) response-based post-induction treatment strategy in patients with advanced FL following first line therapy.4 The trial included systematic MRD analysis which sought to address unresolved issues with MRD monitoring in FL. MRD analysis is an important tool for identifying patients with FL at risk of relapse, but data on the most reliable technique(s), best tissue source, and most predictive time points for analysis are lacking. Marco Ladetto and colleagues performed the analysis—based on the detection of Bcl-2/IGH rearrangement—on both BM and peripheral blood (PB) taken at eight preplanned time points (baseline, end of induction [EoI], and every 6 months thereafter until Month 36) by both nested polymerase chain reaction (PCR) and real time quantitative (RQ) PCR. The results of their study are summarized as follows:
- In total, 780 of 786 eligible patients were screened at baseline for presence of molecular markers, of which 443 (57%) had detectable Bcl-2/IGH rearrangement and were included in the study.
- High rates of MRD negativity were observed at EoI by both PCR techniques:
- Nested PCR: 87% in BM, 95% in PB.
- RQ-PCR: 90% in BM, 95% in PB.
- The presence of an MRD positive result at any point during the follow-up period was associated with an increased risk of relapse in the subsequent 6 month interval (HR for PFS, 2.82, 95% confidence interval [CI], 1.84–4.34; p < 0.001).
- MRD positive results at 6, and particularly 12 months or later after EoI showed a sharp increase in HR for relapse, outperforming earlier evaluation at EoI, and were similar in both BM or PB, and using nested or RQ-PCR.
- Although later timepoints were superior in identifying progression risk, MRD positivity in BM at EoI was predictive of shorter 4-year PFS (61% vs 75% by nested-PCR and 54% vs 74% by RQ-PCR; p = 0.03 and p = 0.003, respectively).
- Patients who were MRD positive at EoI and subsequently converted to MRD negative at the following time point had superimposable outcomes to patients who were consistently MRD negative.
- Conversely, patients who were MRD negative at EoI and subsequently converted to MRD positive had worse outcomes (HR for PFS, 1.75; 95% CI, 1.21–2.53; p = 0.003).
- BM results were more reliable initially; however, PB results were comparable to BM results from month 12 after EoI onwards.
In summary, MRD analysis was predictive of poor outcomes at preplanned time points taken over a 36-month period, with both nested and RQ-PCR performing adequately. Ladetto, et al. suggest RQ-PCR as the preferred method, given it is widely used and internationally standardized. BM sampling was superior in predicting relapse early on, but from Month 12 after EOI onwards, PB was equivalent, and thus offers reliable long-term non-invasive MRD monitoring.
Lenalidomide and rituximab: A chemotherapy-free first line therapy for patients with FL
Morschhauser, et al.5 presented 6-year results from this phase III trial (NCT01650701), which compared standard rituximab and chemotherapy (R-chemo), with the chemotherapy-free combination lenalidomide and rituximab (R2) in patients with previously untreated FL. Second interim analysis results were reported after 75% of total PFS events were reached.
Overall, 1,030 patients with untreated Grade 1‒3a FL requiring therapy according to Groupe d'Etude des Lymphomes Folliculaires (GELF) criteria were randomized to R2 (n = 513) or R-chemo (n = 517); similar baseline characteristics were observed in each group.
The R2 treatment regimen consisted of (Figure 1):
- Lenalidomide: 20 mg/day on Days 2–22 of each 28-day cycle for 6 cycles. Patients with a complete response (CR) after 6 cycles receive 10 mg/day for 12 cycles; patients with a partial response continue 20 mg/day for 3‒6 cycles and then 10 mg/day for up to 18 cycles.
- Rituximab dose: 375 mg/m2 weekly in Cycle 1, and on Day 1 of Cycles 2–6, continued in responders every 8 weeks for 12 additional cycles.
R-chemo treatment regimen:
- Investigator’s choice of standard R-chemo (R-CHOP, R-CVP, or BR), followed by 12 cycles of rituximab.
Figure 1. Experimental arm treatment for Cycles 1‒6*
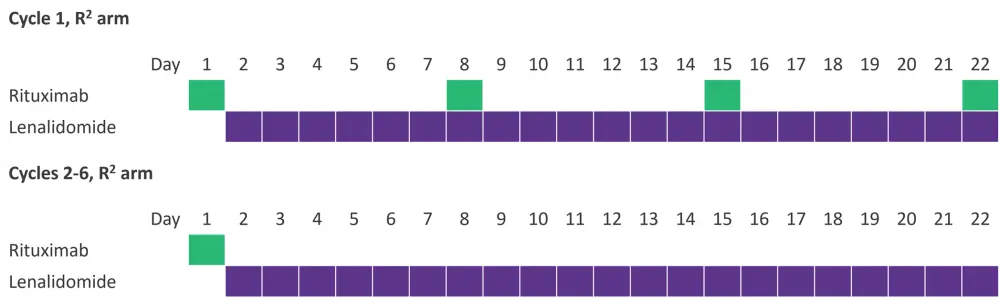
*Data from Morchhauser, et al.5
Results are summarized in Table 1. In both R2 and R-chemo groups, 32% of patients experienced progression/relapse, of which 107 and 99 patients received additional treatment, respectively, and the overall response rate (ORR) and overall survival following treatment remained comparable. The overall safety profiles in both groups were consistent with the previous analysis.
Table 1. Efficacy results of R2 vs R-chemo*
|
CI, confidence interval; CR, complete response; CRu, unconfirmed complete response; EFS, event free survival; HR, hazard ratio; OS, overall survival; PFS, progression free survival; PR, partial response; R2, Rituximab + lenalidomide; R-chemo, standard rituximab chemotherapy; TTNLT, time to next antilymphoma treatment. |
||||
|
Response, % (95% |
R2 |
R-chemo |
R2 vs R-Chemo, HR (95% CI) |
p value |
|---|---|---|---|---|
|
CR/CRu at 120 |
48 |
53 |
|
0.1 |
|
6-year PFS |
60 (55–64) |
59 (54–64) |
1.03 (0.84–1.27) |
0.78 |
|
6-year OS |
89 |
89 |
1 |
|
|
6-year EFS† |
60 (56–65) |
62 (58–67) |
1.07 (0.88–1.32) |
0.49 |
|
6-year TTNLT |
70 (65–73) |
73 (68–76) |
1.19 (0.94–1.51) |
0.14 |
|
Survival after progression |
||||
|
5-year OS after progression |
69 (60–77)‡ |
74 (65–81)§ |
1.17 (0.73–1.87) |
0.51 |
|
Response after progression/relapse treatmentǁ |
||||
|
ORR |
61 |
59 |
— |
— |
|
CR |
32 |
42 |
— |
— |
|
CRu |
6 |
3 |
— |
— |
|
PR |
23 |
13 |
— |
— |
In conclusion, R2 demonstrated similar efficacy compared with R-chemo in patients with previously untreated Grade 1‒3a FL, offering a chemotherapy-free alternative first line treatment.
FL therapies in development
Mosunetuzumab and glofitamab, both CD20/CD3 bispecific antibodies that redirect T cells to target and eliminate malignant B cells,6 offer new potential treatments for patients with relapsed or refractory (R/R) FL. Data from studies of mosunetuzumab and glofitamab in the third line setting for FL were presented at this year’s ASH annual meeting and are summarized below.
Mosunetuzumab monotherapy: A third+ line treatment option for patients with R/R FL
A total of 90 patients were included in Budde, et al.3 phase I/II study of mosunetuzumab monotherapy in R/R FL. Patients had Grade 1‒3a FL, an Eastern Cooperative Oncology Group Performance Status (ECOG PS) ≤1, and were R/R to at least 2 prior therapy lines, including an anti-CD20 antibody and an alkylator. Mosunetuzumab was given for 8 (in patients with CR) or 17 (in patients with partial response or stable disease) cycles, with step up dosing (SUD) to reduce CRS risk as follows:
- Cycle 1: Day 1: 1 mg, Day 8: 2 mg, Day 15: 60 mg
- Cycle 2: Day 1: 60 mg
- Cycles 3+: Day 1: 30 mg
The primary end point, CR, was assessed by positron emission tomography - computed tomography (PET/CT). Results are shown in Table 2. Median PFS was 17.9 months.
Table 2. Response rates to mosunetuzumab monotherapy by pre-specified subgroups*
|
Ab, antibody; CI, confidence interval; CR, complete response; ORR, objective response rate; POD24, progression of disease within 24 months from the start of initial therapy. |
||
|
Study population |
ORR, % (95% CI) |
CR, % (95% CI) |
|---|---|---|
|
All† |
80 (70–88) |
60 (49–70) |
|
POD24‡ |
85 (72–94) |
57 (42–72) |
|
2 prior therapy lines§ |
85 (69–95) |
74 (56–87) |
|
³≥3 prior therapy linesǁ |
77 (64–87) |
52 (38–65) |
|
Disease refractory to prior |
76 (64–85) |
52 (40–64) |
|
Double refractory disease# |
71 (56–83) |
50 (35–65) |
|
Disease refractory to last |
77 (65–87) |
52 (39–65) |
Mosunetuzumab had a manageable safety profile with a low discontinuation rate due to adverse events (AEs [4 patients; 4.4%]). CRS was the most common AE, but was generally mild, occurred in Cycle 1, and resolved in all patients in a median of 3 days. Serious adverse events occurred in 42 out of 90 patients (47%).8
Mosunetuzumab produced deep and durable results in patients with R/R FL, including those with POD24 and double refractory disease, and represents a potential new third line therapy option for patients with R/R FL.
Glofitamab as monotherapy or in combination with obinutuzumab offers another potential third line therapy for R/R FL
Glofitamab monotherapy with obinutuzumab pretreatment, or combined with obinutuzumab, has shown efficacy and a tolerable safety profile in patients with R/R non-Hodgkin lymphoma. Morschhauser, et al.6 presented updated results with three different SUD regimens in patients with R/R FL.
Three monotherapy cohorts:
- Obinutuzumab 1000 mg given 7 days prior to first glofitamab dose.
- IV glofitamab SUD given on Day 1 and Day 8 of Cycle 1; then at target dose for Cycle 2:
-
- 2.5/10/16, n = 3.
- 2.5/10/30, n = 21.
- Or SUD on Day 1 and 8 of Cycle 1, and Day 1 of Cycle 2, then target dose Day 1 of Cycle 3:
- 0.5/2.5/10/30, n = 29.
Combination cohort: (n = 19)
- Glofitamab SUD given on Day 1 (2.5 mg) and Day 8 (10 mg) of Cycle 1, then at target dose (30 mg) combined with obinutuzumab 100 mg from Day 1, Cycle 2 and onwards (every 21 days for up to 12 cycles).
Results are shown in Table 3. Median follow up of CMR was 4.4 months and 5.5 months for monotherapy and combination therapy, respectively, and was therefore insufficient to assess CMR duration.
Table 3. Complete metabolic response rates and overall response rates of glofitamab monotherapy and combination therapy with obinutuzumab*
|
CMR, complete metabolic response rate; ORR, overall response rate; PI3Ki, phosphoinositide 3-kinase inhibitor; POD24, progression of disease within 24 months from the start of initial therapy; SUD, step-up dose. |
||||
|
Outcome, % (unless otherwise stated) |
Monotherapy cohort |
Combination therapy |
||
|---|---|---|---|---|
|
ORR |
81 |
100 |
||
|
CMR |
70 |
74 |
||
|
CMR by subsets of study population |
||||
|
Double |
50 |
43 |
||
|
POD24 |
58 |
70 |
||
|
Pl3Ki |
43 |
50 |
||
|
Monotherapy cohort SUD subgroups |
||||
|
|
0.5/2.5/10/30 mg‡ |
2.5/10/16 mg§ |
2.5/10/30 mgǁ |
— |
|
CMR by SUD subgroup |
72 |
67 |
67 |
— |
The safety profile of glofitamab was tolerable. The most common AE was CRS, occurring mostly in Cycle 1 or 2 (Table 4). CRS events were almost entirely Grade 1 or 2, and all had resolved at data cut-off. A single episode of Grade 3 CRS was observed in the 2.5/10/16 mg monotherapy cohort.
Table 4. CRS events by cohort and SUD subgroup*
|
CRS, cytokine release syndrome; SUD, step-up dose. |
||||
|
Adverse event, % |
Monotherapy cohort
|
Combination |
||
|---|---|---|---|---|
|
CRS rate |
66 |
79 |
||
|
Grade 1 |
47.2 |
52.6 |
||
|
Grade 2 |
17 |
26.3 |
||
|
Monotherapy cohort SUD subgroups |
||||
|
|
0.5/2.5/10/30 mg† |
2.5/10/16 mg and 2.5/10/30 mg ‡ |
|
|
|
CRS rate by SUD |
55.2 |
79.2 |
|
|
In conclusion, high response rates were achieved in patients with R/R FL both as a monotherapy or in combination with obinutuzumab. Given the short follow-up in this study, further follow-up is required to better assess safety and efficacy of glofitamab in this population.
Mosunetuzumab and lenalidomide as second line therapy for R/R FL
Morschhauser was busy at ASH; in addition to his other presentations, he presented an abstract with data from a phase 1b study investigating mosunetuzumab in combination with lenalidomide in patients with R/R Grade 1‒3a FL who had received at least one prior systemic therapy.7
Patients enrolled in the study (n = 29 as of the data cut-off) were to receive 12 cycles of mosunetuzumab and lenalidomide:
- Mosunetuzumab (via intravenous infusion) was given in SUD on Cycle 1 Day 1 (1 mg) and Cycle 1 Day 8 (2 mg); the target dose (30 mg) was given on Cycle 1 Day 15 and on Day 1 of Cycles 2‒12.
- Lenalidomide (oral) was administered on Days 1‒21 of Cycles 2‒12.
The primary endpoint was safety, and the secondary endpoints included assessment of response and long-term efficacy.
Regarding baseline characteristics:
- The median age was 59 years (range, 30‒79 years), and 13 patients (44.8%) were male.
- All patients had an ECOG Performance Status of 0 or 1.
- The median number of prior lines of therapy was 1 (range, 1‒6 lines of therapy).
- Three patients (10.3%) had POD24.
All patients were eligible for the safety evaluation at data cut-off:
- All patients had at least one any-grade AE.
- The most common AE was CRS, which occurred in eight patients (27.6%).
- All CRS events were Grade 1 (seven patients) or Grade 2 (one patient) and most occurred in Cycle 1.
- All CRS events resolved without sequelae, and no patients required tocilizumab, ICU admission, or high flow oxygen.
- Thirteen patients had Grade 3‒4 AEs and nine patients had serious AEs; no fatal AEs occurred.
- In total, 27 patients (93.1%) had AEs related to mosunetuzumab, and 23 patients (79.3%) had AEs related to lenalidomide.
- There were six AEs leading to dose delays of mosunetuzumab, and eight AEs leading to dose interruption or reduction of lenalidomide. One patient discontinued lenalidomide due to an AE.
- Seven patients (24.1%) reported Grade 3‒4 neutropenia; all events resolved.
The ORR was 89.7%, with 65.5% of patients achieving a complete metabolic response, and 24.1 achieving a partial metabolic response. In the three patients with POD24, the ORR was 100%.
The safety and efficacy results of mosunetuzumab + lenalidomide in this patient population are encouraging and support further investigation in a randomized phase III study.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content