All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
AACR 2020 | Ibrutinib plus rituximab as a first-line treatment for patients with follicular lymphoma
Rituximab, an anti-CD20 monoclonal antibody, single agent or in combination with chemotherapy is used as a first-line treatment of follicular lymphoma (FL). Although rituximab-based regimens lead to high overall response rates (ORR), they are associated with significant toxicity. Rituximab in combination with targeted therapies could potentially have more acceptable toxicity profile.
Nathan Fowler and colleagues investigated the efficacy and safety of rituximab in combination with ibrutinib, a Bruton’s tyrosine kinase (BTK) inhibitor, in a phase II study.1 The study results were recently published in the British Journal of Haematology.
Study design
An open-label, non-randomized, multicentre, phase II study PCYC-1125-CA (NCT01980654) consisted of the main study arm and an exploratory arm. The aim of the main study was to evaluate efficacy and safety of rituximab plus ibrutinib, while the smaller exploratory study looked to explore biomarkers during ibrutinib therapy before administration of rituximab. The study design is presented in Figure 1.
Figure 1. Treatment schema.
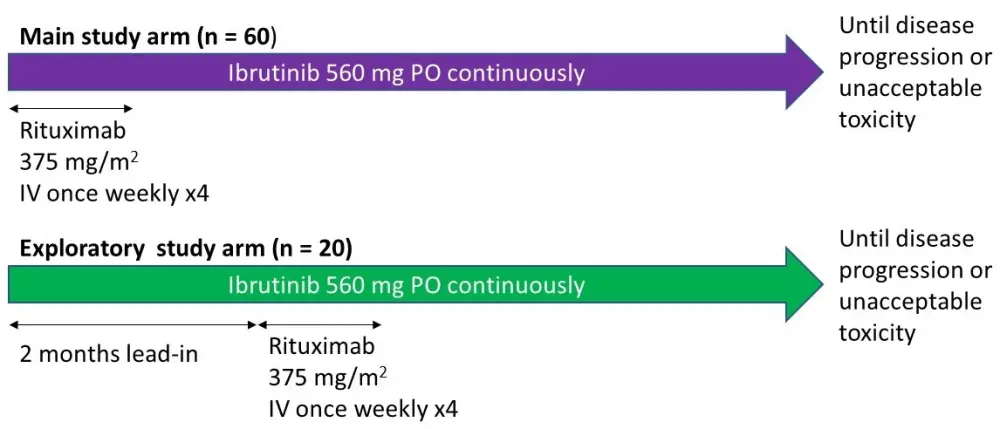
IV, intravenous; PO, administered orally
Patient eligibility criteria
- Age ≥ 18 years
- Previously untreated FL (Grade 1–3A) with stage II–IV disease
- Life expectancy > 3 months
- At least one measurable lesion ≥ 2 cm detected by computed tomography (CT) scan
Endpoints
- Primary
- ORR (compared to the average ORR of 53% with first-line rituximab for FL from two comparable studies 2,3)
- Secondary
- Duration of response (DOR)
- Progression-free survival (PFS)
- Overall survival (OS)
Results
- In total, 80 patients took part in the study. Baseline patient characteristics are presented in Table 1
- Treatment exposure
- Ibrutinib was administered to all patients, with the median duration of 25.5 (0.8–41.9) months in the main study arm and 28.9 (1.0–35.0) months in the exploratory arm
- All patients in the main study arm and 17 of 20 patients in exploratory study arm received rituximab
Table 1. Baseline patient characteristics
|
ECOG, Eastern Cooperative Oncology Group; FLIPI, Follicular Lymphoma International Prognostic Index |
||
|
Characteristic |
Main study (n = 60) |
Exploratory study (n = 20) |
|
Age, years Median (range) ≥ 65 years old, % |
58 (32–84) 30 |
55 (30–75) 40 |
|
Male gender, % |
47 |
60 |
|
Disease grade, % 1 2 3a |
32 58 10 |
55 40 5 |
|
ECOG performance status, % 0 1 |
78 22 |
60 40 |
|
FLIPI score, % Low risk (0–1) Intermediate risk (2) High risk (3–5) |
12 38 50 |
5 45 50 |
|
Bulky disease, % ≥ 5 cm ≥ 7 cm ≥ 10 cm |
38 20 3 |
15 5 5 |
Efficacy
- The median follow-up in the main study arm and the exploratory study was 34 (5.8–42+) months and 29 (4–35) months, respectively
- The ORR
- In the main arm, the ORR of 85% (95% CI, 73–93) was higher than the 53% null hypothesis of rituximab alone for previously untreated patients with low-grade FL
- In the exploratory arm, the ORR was 75% (95% CI, 51–91)
- The best responses are presented in Figure 2
- The median time to response was 2.7 (1.1–16.5) months in the main arm and 4.3 (1.8–18.0) months in the exploratory arm
Figure 2. Response rates.
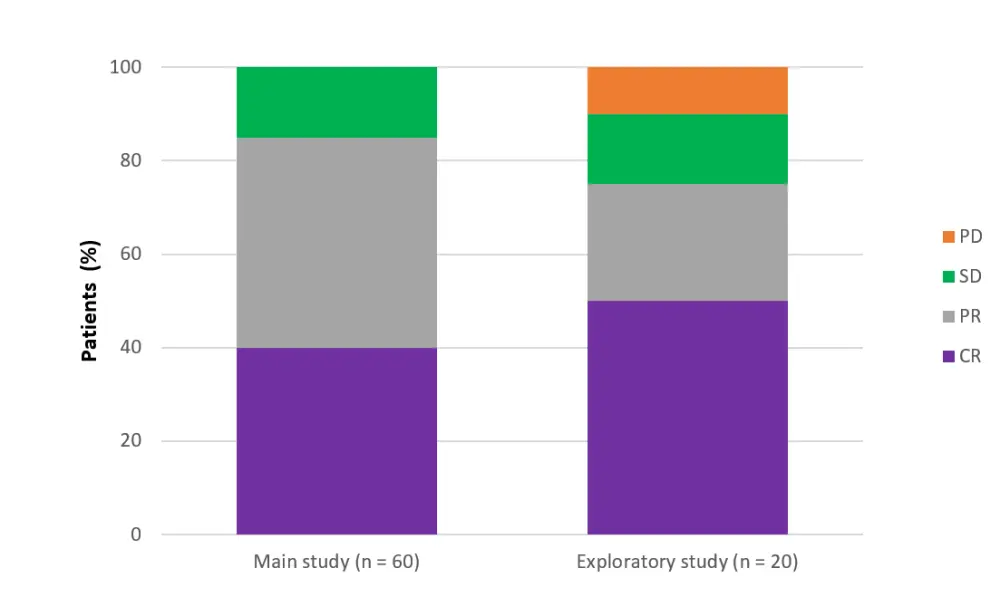
CR, complete response; ORR, overall response rate; PD, progressive disease; PR, partial response; SD, stable disease
- DOR was not reached
- main arm – 95% CI, 30.2 months–not estimable [NE], after a median follow-up of 30.5 months
- exploratory arm – 95% CI, 24.6 months–NE, after a median follow-up of 22.1 months
- The median PFS
- 41.9 months (95% CI, 31.6–41.9) in the main arm
- Not reached (95% CI, 23.5 months–NE) in the exploratory arm
- The 30-month OS rate
- 97% (95% CI, 87–99) in the main arm
- 100% (95% CI 100–100) in the exploratory arm
- An analysis based on FLIPI scores revealed
- Reduction in tumor burden across all risk scores, with response rates (78–100%) in both arms
- The median PFS and OS in patients with low- or intermediate-risk FLIPI scores were not reached in either arm
- In patients with high-risk FLIPI scores, the median PFS and OS were 41.9 months in the main study arm and not reached in the exploratory arm
Safety
- The frequency of treatment-emergent adverse events (TEAEs) was similar between treatment arms
- All patients experienced AEs, and 64% experienced a Grade 3/4 TEAE (Table 3).
- Serious TEAEs occurred in 25% of patients, mainly pyrexia (6%) and pneumonia (5%)
Table 3. Selected safety summary
|
TEAE, treatment-emergent adverse event |
|||
|
TEAE |
Main arm (n = 60) |
Exploratory arm (n = 20) |
Total (n = 80) |
|
Any Grade 3/4 TEAE, % |
62 |
70 |
64 |
|
Grade 3 and 4 TEAEs reported in > 5% of patients in any arm, % Fatigue Diarrhea Myalgia Maculopapular rash Arthralgia Pyrexia Urinary tract infection |
12 2 5 5 3 3 2 |
5 20 10 10 10 15 10 |
10 6 6 6 5 6 4 |
|
Any serious TEAE, % |
18 |
25 |
20 |
|
Any Grade 5 TEAE, % |
3 |
0 |
3 |
|
Dose modifications due to Grade 3/4 TEAE, % Ibrutinib dose reduction Withholding of rituximab dose |
10 2 |
20 5 |
13 3 |
|
Discontinuation due to a Grade 3/4 TEAE, % Ibrutinib Rituximab |
18 0 |
5 0 |
15 0 |
Conclusions
The results of this study demonstrated clinical activity and durable responses with the combination of ibrutinib and rituximab in patients with first-line FL. The safety profile of the combination was manageable and consistent with that of single-agent ibrutinib and rituximab. However, additional studies are required to establish whether combination of ibrutinib with rituximab is superior to rituximab alone in this setting.
Future directions
The currently ongoing phase III PERSPECTIVE (PCYC-1141-CA, NCT02947347) clinical trial will evaluate ibrutinib-rituximab combination as a first-line treatment for FL in elderly patients or those with comorbities.4 The study aims to recruit around 440 patients who are aged ≥ 70 years or who are aged 60–69 years with comorbidities (creatinine clearance 30–59 mL/min and/or ECOG performance status of 2), who in the first part of the study, will be randomized 3:1 to
- Ibrutinib (once daily) plus rituximab (4 weekly cycles followed by rituximab maintenance)
- In the second part of the study, patients would be randomized 1:1 to
- Ibrutinib once daily
- Placebo
- In the second part of the study, patients would be randomized 1:1 to
- Placebo plus rituximab (4 weekly cycles followed by rituximab maintenance)
- In the second part of the study, all patients will receive placebo
The primary endpoint in both study parts is PFS.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?