All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ICML 2017 | Prognostic tools, CHRONOS-1, and pembrolizumab plus rituximab for relapsed patients – Follicular Lymphoma Session at 14-ICML
On Friday 16th June, during the 14th International Conference on Malignant Lymphoma (ICML), the LH attended the Follicular Lymphoma (FL) Session co-chaired by Brad S. Kahl, MD, (Washington University School of Medicine in St. Louis) and Eva Kimby, MD, (Karolinska University Hospital).
Abstract 104
The first talk was presented by Sarah Huet from Hospices Civils de Lyon, Pierre-Bénite, France, and was titled focused on Gene-Expression Profiling (GEP) in FL.
The talk began by stating that FL is associated with heterogeneous outcomes. GEP studies have highlighted the role of non-tumor subsets in FL and clinicogenetic models have recently been described. However, a predictor model able to accurately identify patients at higher risk of progression is still required.
The current study analyzed the gene-expression profiles of FL tumors taken at diagnosis in a discovery cohort of patients enrolled on the phase III PRIMA trial (NCT00140582). Huet outlined the objectives of this analysis:
- Supervised analysis – develop an expression-based predictor of Progression-Free Survival (PFS) applicable to Fixed Formalin Paraffin Embedded (FFPE) samples and evaluate this in independent cohorts
- Unsupervised analysis – biological interpretation
Huet gave some background on the PRIMA study, which enrolled 1,217 patients with newly diagnosed FL and evaluated the benefit of maintenance rituximab (n=507) compared to observation (n=513) after induction with R-CHOP, R-CVP, or R-FCM (Salles et al. Lancet. 2011).
An overview was given of how the predictive model was built:
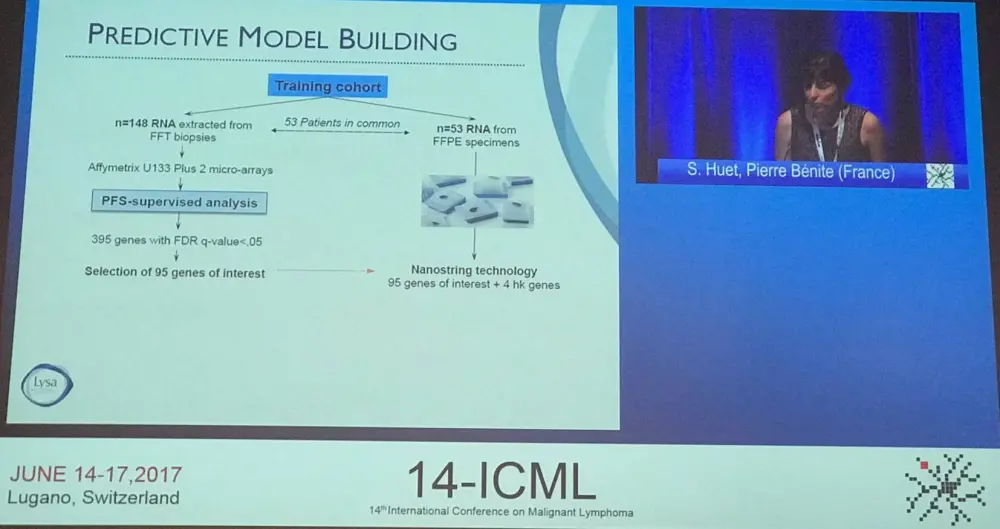
The expression of 395 genes was associated with the risk of progression. Twenty-three genes reflecting B-cell development, apoptosis, DNA damage response, cell migration (CXCR4, VCL, and RGS10), and cell cycle (USP44 and E2F5) were retained to build a predictive model. The model identified a population at increased risk of progression in the training cohort (P < 0.001).
Further validation of the model used NanoString technology (23 genes of interest plus 4 housekeeping genes) in FFPE samples from three independent international cohorts: a distinct validation set from the PRIMA trial (178 patients), the Mayo Clinic/Iowa SPORE project (201 patients), and the Barcelona Hospital Clinic (111 patients). All patients had received rituximab plus chemotherapy followed by either anti-CD20 maintenance or no maintenance. Of 490 FFPE samples, 461 passes quality control (94%) and were used in model validation.
In the entire validation cohort, 122/461 (26%) of patients were identified as being at high risk of progression. The median time to progression was 3.1 years in high-risk and 10.8 years in low-risk groups patients (P < 0.001). The risk of Lymphoma progression at 2 years (POD24) was two-times higher in high-risk patients (38% vs. 19%; P < 0.001). Multivariate analysis found that the score predicted PFS independently of anti-CD20 maintenance treatment and FL-IPI score (HR for combined cohort, 2.30; 95% CI, 1.72–3.08). Moreover, the model stratified patients with high-risk FL-IPI into groups with substantially distinct outcomes:
|
|
|
|
PFS |
||
|---|---|---|---|---|---|
|
FL-IPI |
Risk Group |
N (%) |
Median (yr) |
2-yr (%) [95% CI] |
5-yr (%) [95% CI] |
|
Low n=130 |
High-risk |
19 (15) |
NR |
79 [63–100] |
57 [39–85] |
|
Low-risk |
111 (85) |
R |
88 [83–94] |
81 [74–89] |
|
|
Intermediate n=151 |
High-risk |
42 (28) |
4.8 |
74 [61–88] |
45 [31–65] |
|
Low-risk |
109 (72) |
NR |
81 [74–89] |
61 [52–71] |
|
|
High n=173 |
High-risk |
59 (34) |
2.1 |
50 [39–65] |
26 [17–41] |
|
Low-risk |
114 (66) |
6.6 |
73 [65–82] |
56 [47–67] |
|
The additional unsupervised analyses of the training cohort expression data confirmed that microenvironmental features as well as tumor cells impact on FL prognosis. In particular, a centroblast-associated signature (ICA13_centroblast-like) had adverse prognostic significance, further strengthening the biological rationale of this model.
Huet concluded the talk by stating that the 23-gene expression score was applicable to routine FFPE samples and predicted PFS independently of FL-IPI and maintenance. The score was validated in three large independent cohorts and unsupervised analysis identified a signature that further supports the biological rationale beyond the PFS-derived model. Huet emphasized that the model will be tested further in patients who had received other therapeutic regimens to rituximab-chemotherapy and in those with low tumor burden.
Abstract 105
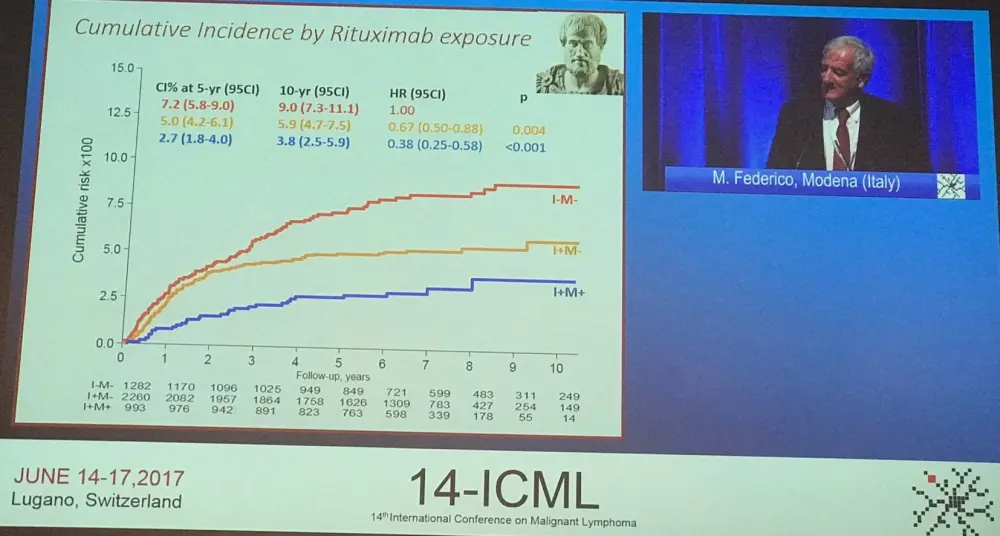
Prof. Massimo Federico from the University of Modena e Reggio Emilia, Modena, Italy, gave the second talk which discussed he risk of transformation in FL and the ARISTOTLE (Assessing the Risk of Transformation and Outcome of Follicular Lymphoma in the Immunochemotherapy Era) study.
The study is based on clinical trials or Lymphoma registries collected by 10 different European Lymphoma Groups. The present study has a time frame of 1997–2013 using biopsy proven Histologic Transformation (HT) reports by the participating institutions, and in which transformation was diagnosed as the first event after initial therapy (regardless of whether patients had been managed expectantly at diagnosis or not). The primary outcome measures are the cumulative risk of HT and Survival After Transformation (SAT).
So far 9,172 cases have been referred and 7,405 (81% of potentially) are assessable for the main endpoint, i.e. the transformation risk. Patients were excluded due to transformed FL (tFL) at diagnosis (n=22), lack of date of diagnosis or relapse (n=49), diagnosis earlier then 1997 or later than 2013 (n=1,767; 19%), and other reasons (n=1,255). At time of diagnosis, patients had a median age of 58 years, and low, intermediate, and high risk FL-IPI of 30%, 34% and 37%, respectively. A total of 4,531 first events (61% of assessable) were reported, 792 of which were confirmed by biopsy (17% of any event). Overall, 439 were classified as HT.
Initial treatment, as assessed in 7,335 patients, was Watch & Wait (W&W) in 941 patients (13%) and active treatment in 6,394 patients (87%).
|
Group |
Registries |
Trials |
Population based registries |
Total |
|---|---|---|---|---|
|
N (%) |
2760 (37) |
2552 (34) |
2093 (28) |
7405 |
|
CR % |
67 |
64 |
51 |
63 |
|
ORR % |
92 |
92 |
80 |
90 |
|
5-year OS % |
82 |
87 |
79 |
83 |
|
PFS24 |
20 |
29 |
33 |
27 |
|
Rituximab use |
80 |
82 |
75 |
80 |
The cumulative risk of biopsy proven HT as first event (n=413/7,335) at 5-years and 10-years was 5.5 (95% CI, 5.0–6.1) and 7.1 (95% CI, 6.4–8.0), respectively. The incidence rate x1,000 people per year is 9.0 (95% CI, 8.2–9.9). Cumulative risk at 5-years and 10-years in patients who had received active treatment was 5.3 and 6.7, compared to 7.4 and 10.4 in patients who underwent W&W (HR, 1.43; 95% CI, 1.10–1.85; P = 0.007). In patients who had not and had received rituximab, 5- and 10-year cumulative risk was 7.2 and 8.9 compared to 4.8 and 6.2 (HR, 0.65; 95% CI, 0.52–0.82; P < 0.001).
After a median follow-up of 4.6 years, 191/439 events were reported. Median SAT was 32 months (95% CI, 24–46) and 5-year and 10-year rates were 41% (95% CI, 36–46) and 32% (95% CI, 25–38), respectively. 5-year SAT rate in patients whose transformation took place more than one year after diagnosis was 45% (95% CI, 38–81) compared to 34% (95% CI, 26–42) in patients who transformed in less than one year (HR, 1.64; 95% CI, 1.27–2.10; P < 0.001).
Federico concluded the talk by stating that the ARISTOTLE study, despite its retrospective nature, indicates that the use of rituximab significantly reduces the risk of HT as a first event. Treatment and management of tFL remains challenging, although the outcomes of patients in this analysis do not appear as poor as those reported in the literature.
Abstract 106
A.S. Cottereau from Tenon Hospital, Paris, France, presented the next abstract based on pooled analysis from LYSA and FIL trials of a prognostic model for high tumor burden FL.
Advanced FL is characterized by frequent relapses and increasingly aggressive disease; around one-fifth of patients relapse less than 2 years from first-line therapy and 5-year survival is only around 50%.
Prognostic markers that are currently available to us, such as FL-IPI and FL-IPI2, do not accurately identify patients with high tumor burden or advanced stage FL. Models combining clinical and molecular data have been proposed, such as m7-FL-IPI. Of the recent prognostic imaging markers identified, End of Induction PET (Eoi PET) and Total Metabolic Tumor Volume (TMTV) computed on baseline PET show promise, and have out-performed the other current prognostic indices for early risk stratification. The current study presented by Cottereau aimed to assess the added value of a model built on these two imaging biomarkers.
Patients included in the FOLLCOLL study (pooling from three prospective trials: PRIMA, PETFOLL and FOLL05) were enrolled when they had both baseline PET, allowing the computation of TMTV, and Eoi PET. TMTV was calculated using a 41% SUVmax threshold; 510cm3 was defined as the optimal cut-off to predict PFS and OS; and Eoi PET positivity was defined as a Deauville Score ≥4.
Of the 1,819 patients included in the FOLLCOLL study, 159 patients were analyzed in the current study: median age was 56 years (range, 28–78; 37% were older than 60), 90.6% were Ann Arbor stage III/IV, 57.4% had an involved BMB, 36.5% a FL-IPI score 3–5, and 30.9% a FL-IPI2 score 3–5. 6 x R-CHOP followed by 2 x rituximab had been administered to 81% of patients, 14% had received R-CVP, and 5% R-FM; 10 patients (6%) had received rituximab maintenance.
Median TMTV was 260cm3 (IQR, 127–554) and 27.7% patients had a high TMTV (>510cm3). Moreover, 133 (83.6%) patients had negative Eoi PET. Median follow-up was 64 months; 71 PFS events and 14 deaths were reported resulting in 5-year PFS of 54.2% and 5-year OS of 91.9%. Patients with high compared to low TMTV had significantly poorer 5-year PFS (31.3% vs. 63.2%; HR, 2.9; 95% CI, 1.7–4.5; P < 0.001) and 5-year OS (83.8% v. 95.0%; HR, 3.9; 95% CI, 1.3–11.9; P = 0.0188). Median PFS for low versus high TMTV patients was NR and 33 months. Median OS for low versus high TMTV patients was NR and 79 months. Patients with positive compared to negative Eoi PET had significantly poorer 5-year PFS (26.9% vs. 59.6%; HR, 3.2; 95% CI, 1.9–5.5; P < 0.001) and 5-year OS (84.0% vs. 93.3%; HR, 4.4; 95% CI, 1.5–12.6; P = 0.0068). Median PFS in PET negative and positive patients was NR and 23.2 months. Median OS in PET negative and positive patients was NR and 74.1 months.
The frequency of positive Eoi PET was significantly higher in patients with high TMTV (29% vs. 11%; P = 0.01). Multivariate analysis found that high TMTV (HR, 2.3; 95% CI, 1.4–3.9; P = 0.001) and positive Eoi PET (HR, 2.3; 95% CI, 1.3–4.1; P = 0.0035) were independent prognostic factors of PFS. For OS, only Eoi PET was prognostic (HR, 3.25; 95% CI, 1.1–9.8; P = 0.0357).
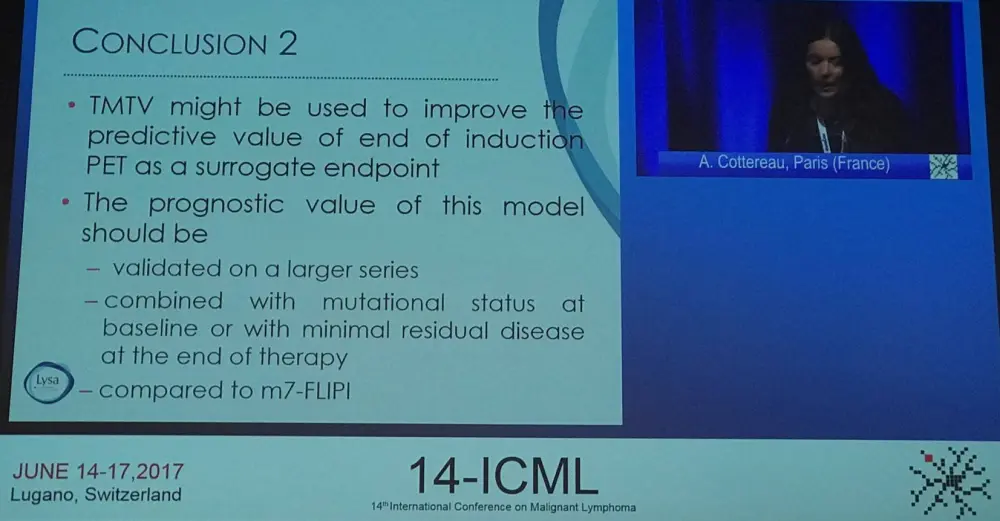
Combining TMTV and Eoi PET stratified patients into three groups: patients with no risk factors (negative Eoi PET and low TMTV, n=102) had a 5-year PFS of 67.5% vs. 33% (HR, 2.9; 95% CI, 1.8–4.9; P < 0.001) for patients with one risk factor (n=44) and 23.1% (HR, 4.6; 95% CI, 2.3–9.2; P > 0.001) for patients with both risk factors (n=13).
Cottereau concluded her part of this session with a succinct summary slide and suggested future work that should be completed to validate this prognostic model:
Abstract 107
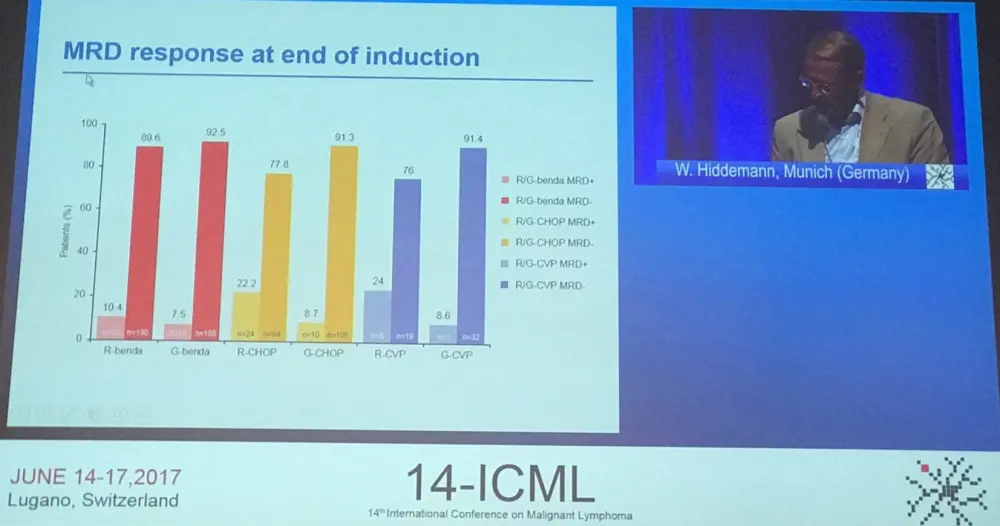
The fourth talk in this session was given by Wolfgang Hiddemann from the Ludwig-Maximilians University Hospital Munich, Munich, Germany, and conveyed updated results for each immunochemotherapy regimen used in the GALLIUM trial (NCT01332968) of newly diagnosed FL patients.
This phase III, open-label, randomized trial demonstrated that, after a median of 41.1 months of follow-up, obinutuzumab (G) significantly improved Investigator (INV; P = 0.0016) and Independent Review Committee (IRC; P = 0.0118) assessed 3-year PFS compared to rituximab (R) when combined with chemotherapy (chemo; CHOP, CVP, or bendamustine [B]). Grade 3–5 AEs (75.5% vs. 68.5%) and SAEs (47.2% vs. 41.2%) were more frequently reported in patients administered G-chemo than R-chemo. During this talk, Hiddemann presented updated results for each immunochemotherapy regimen, beginning with baseline characteristics:
|
N (%) |
B, n=686 |
CHOP, n=399 |
CVP, n=117 |
|---|---|---|---|
|
Median age, yrs (range) |
59 (23–88) |
58 (31–85) |
59 (32–85) |
|
Age ≥80 yrs |
23 (3.4) |
3 (0.8) |
4 (3.4) |
|
Male |
332 (48.4) |
177 (44.4) |
54 (46.2) |
|
Charlson Comorbidity Index score ≥1 |
163 (23.8) |
69 (17.3) |
22 (18.8) |
|
ECOG PS 2 |
24 (3.5) |
8 (2.0) |
6 (5.1) |
|
FL-IPI high risk (≥3) |
274 (39.9) |
187 (46.9) |
41 (35.0) |
|
Bulky disease (≥7cm) |
274 (39.9) |
206 (51.6) |
46 (39.3) |
1,202 FL pts were randomized. Baseline characteristics were generally balanced between the three chemo groups, although B and CVP patients had relatively more comorbidities, e.g. gastrointestinal and vascular disorders, than CHOP patients.
Investigator-assessed 3-year PFS in the ITT population remained superior for G-chemo relative to R-chemo (HR, 0.68; 95% CI, 0.54–0.87; P = 0.0016) with consistent HRs across chemo groups. By chemo analysis was not powered to demonstrate statistically significant differences between treatment arms.
INV-assessed responses and MRD responses at end of induction were then discussed:
|
Regimen |
ORR (%) |
CR (%) |
|---|---|---|
|
R-B |
79.4 |
60.6 |
|
G-B |
85.5 |
63.0 |
|
R-CHOP |
88.3 |
61.2 |
|
G-CHOP |
88.3 |
66.0 |
|
R-CVP |
66.7 |
20.0 |
|
G-CVP |
71.4 |
33.3 |
Hiddemann then focused on the incidence of AEs:
|
N (%) of pts reporting ≥1 event |
R-B (n=338) |
G-B (n=338) |
R-CHOP (n=203) |
G-CHOP (n=193) |
R-CVP (n=56) |
G-CVP (n=61) |
|---|---|---|---|---|---|---|
|
Any AE |
331 (97.9) |
338 (100) |
201 (99.0) |
191 (99.0) |
56 (100) |
61 (100) |
|
Grade 3–5 |
228 (67.5) |
233 (68.9) |
151 (74.4) |
171 (88.6) |
30 (53.6) |
42 (68.9) |
|
SAE |
160 (47.3) |
176 (52.1) |
67 (33.0) |
76 (39.4) |
19 (33.9) |
26 (42.6) |
|
Grade 5 (fatal) AE |
16 (4.7) |
20 (5.9) |
4 (2.0) |
3 (1.6) |
1 (1.8) |
1 (1.6) |
|
AE leading to treatment discontinuation |
48 (14.2) |
52 (15.4) |
31 (15.3) |
32 (16.6) |
9 (16.1) |
11 (18.0) |
The difference between treatment arms in grade 3–5 AEs and SAEs was more pronounced in patients treated with CHOP and CVP. Comparisons are confounded by imbalances in baseline patient and disease characteristics between chemo groups. Grade 3–5 AEs were more common in patients treated with CHOP (neutropenia, leukopenia, febrile neutropenia, infusion related reactions). However, SAEs and fatal AEs were more common with B. Many patients with fatal AEs had adverse risk factors such as aged 80 years or older, ECOG PS of 2, and CCI score of one or more. The frequencies of grade 3–5 second malignancies and infections were similar in G and R arms for CHOP and CVP groups but not for B.
Hiddemann concluded the talk by stating that outcomes of this updated analysis are consistent with that previously reported for the GALLIUM study:
- Clinically meaningful improvement in PFS in G-chemo arm
- Higher rates of grade 3–5 and SAEs in G-chemo group
- Imbalance mainly driven by cytopenias, infections, and infusion related reactions
- Similar incidence of AEs leading to discontinuation
The by chemo analysis was confounded by imbalances in baseline characteristics; there was no randomized comparison between chemo backbones. Despite this, a beneficial effect of G was apparent with all chemo backbones. Lastly, there was evidence to suggest that T-cell depletion was prolonged in bendamustine arms and so caution must be taken when using this drug.
Abstract 108
Martin Dreyling from the University Hospital of Munich, Munich, Germany, gave the next talk conveying results from the pivotal phase II CHRONOS-1 study (NCT01660451).
For patients with Relapsed/Refractory indolent Non-Hodgkin Lymphomas (iNHLs), including FL, treatment options are limited. Copanlisib is an intravenously administered pan-Class I Phosphatidylinositol 3-Kinase (PI3K) inhibitor with principal activity against PI3Kα and PI3Kδ isoforms.
The open-label, uncontrolled, phase II CHRONOS-1 study aimed to evaluate copanlisib in patients with iNHL (FL, MZL, SLL, WM) who had relapsed after, or were refractory to, two or more line of previous therapy (including rituximab and alkylating agent). Copanlisib at a dose of 60mg was administered by IV intermittently on days 1, 8, and 15 of a 28-day cycle. The primary efficacy endpoint was ORR per independent radiologic review. Archival tumor tissues were used for mRNA extraction and GEP.
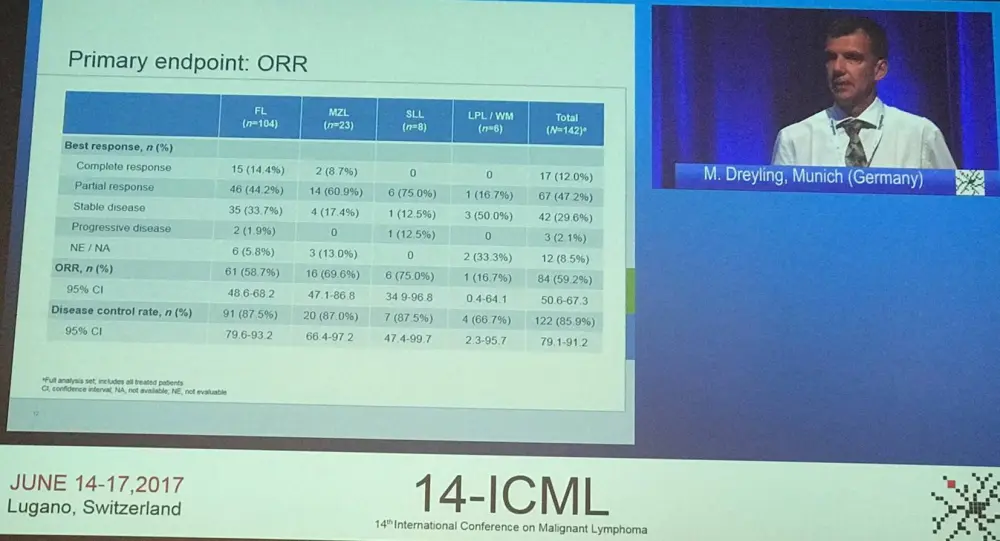
Overall, 212 patients were enrolled for screening, of which 70 failed. The full analysis set comprised 142 treated patients. Treatment is ongoing in 46 (32.4%) of these. Treatment was discontinued in the other 96 patients due to AEs (n=35), radiologic (n=31) or clinical (n=5) progressive disease, withdrawal by patient (n=16), physician decision (n=5), and other reasons (n=4). Patients had a median age of 63 years (range, 25–82), a median of 3 (range, 2–9) previous anti-cancer therapy lines, and a median time from most recent progression of 8.3 months (range, 1–73). The majority of patients (80.3%) had advanced-stage disease at study entry (stage III or IV) and FL was the most common histology (73.2%).
A median of 5.5 (range, 0.3–26) cycles of copanlisib were administered and median duration of treatment was 22 months (range, 1–105). The median percentage of planned dose was 96% (range, 51–103) and there were 105 dose interruptions that lasted a median duration of 1 week (range, 0–3). Over half (54.9%) of dose interruptions lasted less than 1 week. Dose reductions to 45mg and 30mg occurred in 37 and 8 patients, respectively. Nearly all dose interruptions/delays were due to AEs (91.4%). Discontinuation due to treatment-related AEs was reported for 23 patients (16.2%).
The most common treatment-related AEs were transient hyperglycemia (48.6%/40.1%) and hypertension (28.9%/22.5%). Other AEs included neutropenia (24.6%/19.0%), diarrhea (18.3%/4.2%), lung infection (14.1%/10.6%), pneumonitis (7.0%/1.4% [2 patients, grade 3]), and colitis (0.7%/0.7% [1 patient, grade 4]). Three deaths were thought to be drug-related: lung infection, respiratory failure, and thromboembolic event (0.7% each).
For the entire cohort, and the individual FL group, median PFS was 11.2 months. Median OS has not yet been reached.
In exploratory biomarker analysis, baseline FFPE tumor samples were analyzed by GeneCHIP® Human Gene 1.0 ST arrays (Affymetrix, Santa Clara, CA). A gene set enrichment analysis using 33 pathways such as BCR, PI3K, NH-kB, MAPK, apoptosis, and microenvironment signatures was performed in order to identify predictors of clinical sensitivity to copanlisib. It was found that the PI3K and BCR pathway gene expression levels were associated with response (P = 0.009 to 0.035; n=7).
Dreyling concluded his presentation by stating that copanlisib demonstrated encouraging efficacy in heavily pre-treated patients with iNHL, achieving an ORR of 59% with a 12% CR rate as well as a median DoR of 22.6 months and a median PFS of 11.2 months. Additionally, rate of elevation of hepatic transaminases, diarrhea, or pneumonitis were low, and so were rates of opportunistic/fatal infections.
Abstract 109
The last presentation in this session contained interim results from an open-label, phase II study of pembrolizumab plus rituximab in patients with relapsed FL (NCT02446457). This data was presented by Loretta J. Nastoupil, MD, from the University of Texas MD Anderson Cancer Center, Houston, TX, US.
FL tumors are infiltrated with anti-tumor T-cells. However, these cells are often impaired in their function via immune checkpoints such as the PD-1/PD-1L interaction. It has been found that blocking PD-1 improves anti-tumor T-cells’ ability to identify and kill tumor cells; blocking PD-1 on NK cells has been demonstrated to increase NK contribution to Antibody-Dependent Cellular Cytotoxicity (ADCC). Thus, combining pembrolizumab (anti-PD-1 antibody) and rituximab (anti-CD20 antibody) is thought to be synergistic, resulting in the activation of both innate and adaptive immunity. Nastoupil presented that pre-planned interim analysis from an open-label, non-randomized, single institution, phase II trial of pembrolizumab plus rituximab.
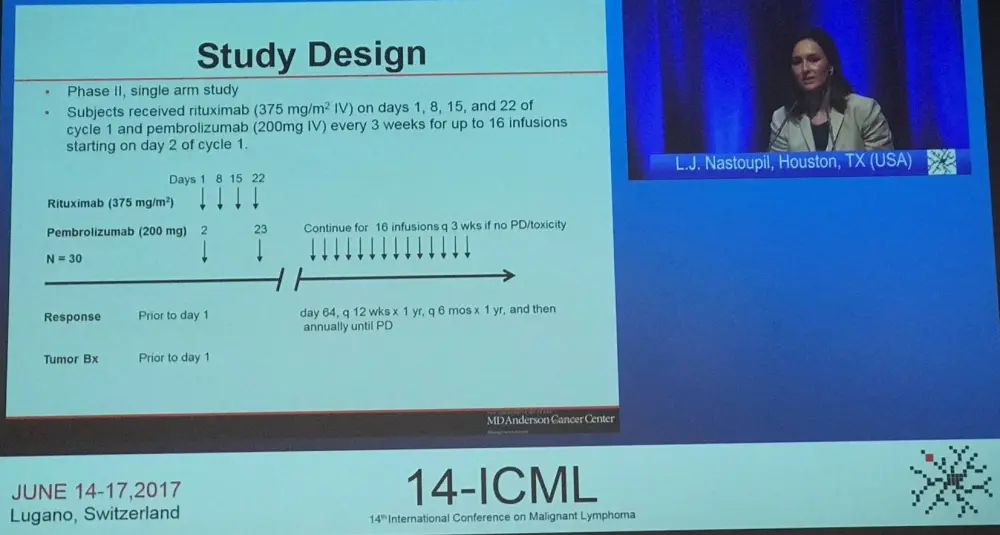
The study aimed to determine the ORR in patients with relapsed FL receiving this combination. Secondary outcome measures included CR rate, PFS, OS, safety, and tolerability. Patients were eligible if they were 18 years of age or older, had an ECOG PS of 0–1, FL grade 1–3a, relapsed after one or more prior lines of treatment, and had rituximab sensitive disease (had a CR or PR lasting ≥6 months after most recent rituximab therapy).
Overall, 32 patients were enrolled; 30 were evaluable for safety and 20 were evaluable for efficacy. Patients had a median age of 64 years (range, 43–84) and a median of 2 (range, 1–4) previous lines of therapy. Of the 30 patients evaluable for safety, 8 (27%) had an ECOG PS of 1, and 8, 16, and 6 patients had low-, intermediate-, and high-risk by FL-IPI. Four patients (13%) had stage II disease, 8 patients (27%) had stage III disease, and 18 (60%) had stage IV disease. Median follow-up was 8.2 months and thus far, no deaths have been reported.
ORR was 65% with CR achieved in 10 patients (CR rate = 50%) and PR in 3 patients. Furthermore, 3 patients have SD, but 4 have progressive disease as best response. Median DoR, PFS, and OS have not been reached.
Nastoupil summarized the treatment-related AEs, and emphasized that no grade 4 or higher AEs were observed:
|
AE (n=30) |
Grade 1 (%) |
Grade 2 (%) |
Grade 3 (%) |
|---|---|---|---|
|
Fatigue |
13 (43) |
3 (10) |
|
|
Eye pain/blurred vision/watery eye |
12 (40) |
1 (3) |
|
|
N/V |
6 (20) |
3 (10) |
2 (7) |
|
Diarrhea |
6 (20) |
3 (10) |
|
|
Dyspnea |
3 (10) |
1 (3) |
|
|
Rash |
3 (10) |
4 (13) |
|
|
Cough |
2 (7) |
2 (7) |
|
|
Lymphopenia |
2 (7) |
3 (10) |
1 (3) |
Discontinuation of study drug was reported in 4 patients due to immune related AEs: diarrhea (n=2), grade 2 rash (n=1), and grade 2 pneumonitis (n=1).
Additionally, 8 baseline tumor samples were tested using PD-L1 22C3 IHC pharmDx. PD-L1 was detected in histiocytes in all 8, but was present in 1–8% of tumor cells in 5 tumors. Moreover, an associated was found between CD8+ Teff score before treatment and CR.
Nastoupil concluded the talk by stating that pembrolizumab plus rituximab has achieved encouraging ORR and CR rates in relapsed FL patients. The combination also demonstrated a favorable toxicity profile. Further correlative studies on tumor and blood samples are ongoing but these interim results indicate that further investigation of this combination for relapsed FL should be carried out. An expansion to include patients with refractory FL is planned.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?