All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | COMPLEMENT-2 trial: mutated NOTCH1 presents as a potential predictive marker of response to FC plus ofatumumab for R/R CLL
On 14th May 2017, during iwCLL, the fifth session took place titled “Additional Considerations for the Initial Treatment of CLL.” This session was chaired by Richard Furman (Weill Cornell) and Jae Park (Memorial Sloan Kettering Cancer Center).
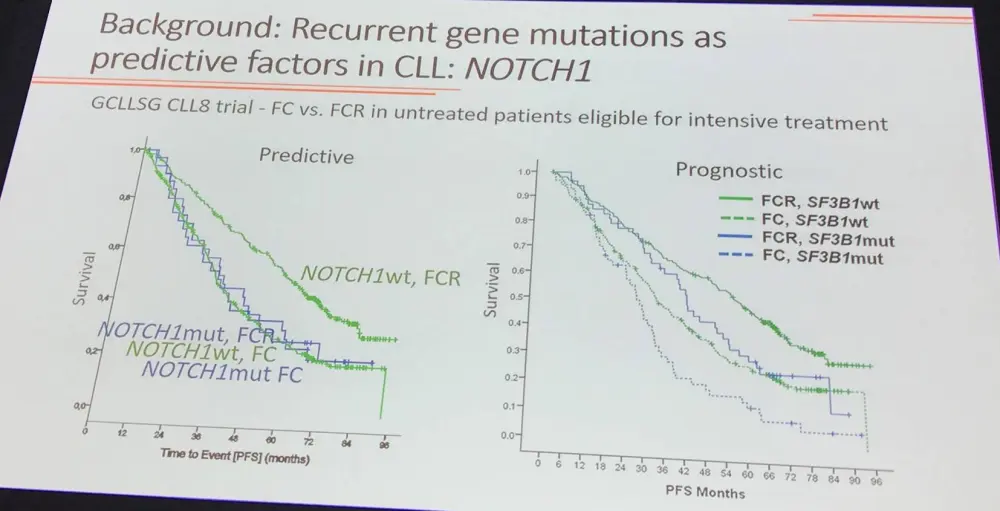
During this session, “NOTCH1 Mutation as a Predictive Factor in the Context of Fludarabine and Cyclophosphamide (FC) With or Without Ofatumumab Treatment” was presented by Eugen Tausch, MD, from Ulm University, Ulm, Germany.
The incidence and impact of TP53, SF3B1, and NOTCH1 mutations in the phase III COMPLEMENT-2 trial of FC vs. FC+ofatumumab in R/R CLL patients were assessed. Samples were available from 89% of patients (325/365) at study entry. Targeted Next Generation Sequencing (tNGS) was carried out for exons 2–11 of TP53, exons 14–16 and 18 of SF3B1, and exon 34 of NOTCH1; all mutations with a Variant Allelic Fraction (VAF) of more than 5% were considered.
Incidence, type and location of mutations:
- 221 mutations identified in 43.7% of pts (142/325)
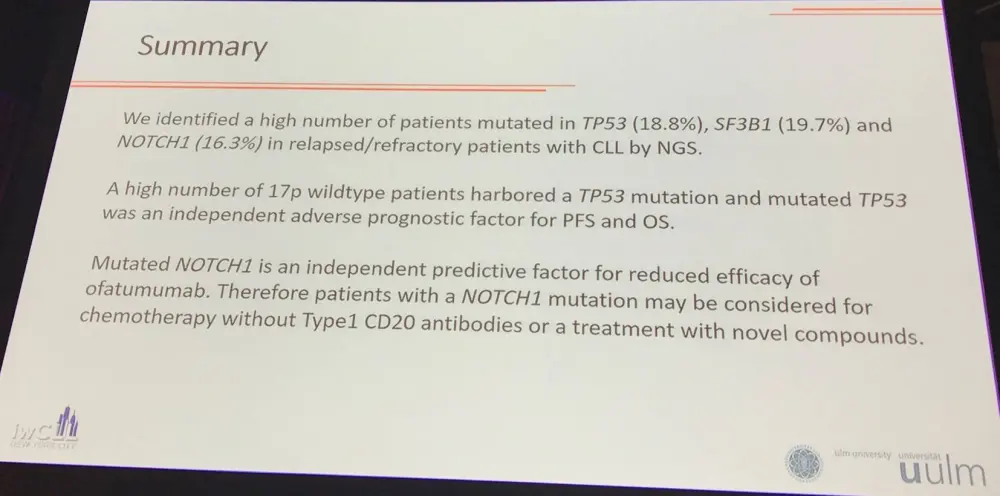
- Incidence: SF3B1 = 19.7%; TP53 = 18.8%; NOTCH1 = 16.3%
- TP53 = 96 mutations in 61 patients; SF3B1 = 69 mutations in 64 patients; NOTCH1 = 56 mutations in 53 patients
- 20/61 TP53 mutated pts harbored additional TP53 mutations; 4/64 SF3B1 mutated pts harbored additional SF3B1 mutations; 3/53 NOTCH1 mutated pts harbored additional NOTCH1 mutations
Associations with aberrations and clinical features:
- Mutated TP53 associated with del(17p), P < 0.01
- Mutated NOTCH1 associated with +12q (P < 0.01) and elevated β2M (P = 0.02)
- Mutated SF3B1 associated with FC+ofatumumab therapy (P < 0.01)
- There were no associations with IGHV, gender, age, Binet stage, ECOG performance state, B symptoms, or WBC
Response to therapy both treatment arms combined:
|
|
TP53 |
SF3B1 |
NOTCH1 |
|||
|---|---|---|---|---|---|---|
|
|
wt |
mut |
wt |
mut |
wt |
mut |
|
CR rate (%) |
19.9% |
11.7% |
19.9% |
12.5% |
19.2% |
14.3% |
|
OR rate (%) |
84.4% |
67.8% |
83.7% |
71.9% |
80.5% |
85.7% |
- Patients with mutated TP53 (P < 0.01) or mutated SF3B1 (P < 0.05) had worse OR to therapy
- Looking into both treatment arms separately did not add any significant result
- FC+ofatumumab achieved a significantly longer median PFS (28.1 months) than FC alone (18.8 months; HR, 0.67; P < 0.01)
- Patients with mutated TP53 (P < 0.01) or mutated SF3B1 (P < 0.05) had worse OR to therapy
Prognostic factors:
- Mutated TP53 was an adverse prognostic indicator for the whole cohort (HR, 1.93; P < 0.001) and both treatment groups separately (FC: HR, 2.14, P < 0.01; FC+ofatumumab: HR, 1.81, P = 0.002)
- Mutated TP53 associated with reduced OS (HR, 2.11, P < 0.01)
- Multivariate analysis:
- Prognostic factors for PFS included FC+ofatumumab therapy (HR, 0.66; P < 0.01), del(17p) (HR, 4.46; P < 0.01), unmutated IGHV (HR, 2.2; P < 0.01), and mutated TP53 (HR, 1.79; P < 0.01)
- Prognostic factors for OS included del(17p) (HR, 5.02; P < 0.01), unmutated IGHV (HR, 1.86; P = 0.01), and mutated TP53 (HR, 1.68; P = 0.04)
- Adding ofatumumab to FC was beneficial in pts with mutated TP53 (HR, 0.52; P = 0.02) and wild type TP53 (HR, 0.68; P = 0.02)
- Adding ofatumumab to FC only conferred benefit in wild type NOTCH1 pts (HR, 0.64; P < 0.01) and not mutated NOTCH1 pts (HR, 0.86; P = 0.67)
Eugen Tausch concluded the presentation with a concise summary slide:
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?