All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | Expression of ROR1 in Chronic Lymphocytic Leukemia
On 14th May 2017, the “Role of the B-Cell Receptor and Other Signaling Pathways in CLL” took place at iwCLL, and was co-chaired by Nicholas Chiorazzi (The Feinstein Institute for Medical Research, Manhasset, NY, USA) and Kostas Stamatopoulos (Center for Research and Technology Hellas, Thessaloniki, Greece).
Thomas J. Kipps, MD, PhD, from the University of California, San Diego, Moores Cancer Center, California, USA, gave a presentation during this session titled “ROR1: An Orphan Becomes Apparent.”
Receptor Tyrosine Kinase-Like Orphan Receptor 1 (ROR1) is primarily expressed during embryogenesis. It is an evolutionarily conserved, type-I membrane protein and has tyrosine-kinase-like and Ser/Thr-rich domains.
It has been reported that ROR1 is expressed on both ZAP-70+ and ZAP-70- CLL cells, as well as on CLL cells that have either Unmutated (U-) or Mutated (M-) IGHV. In contrast, ROR1 is not expressed on normal CD5+ B-cells. ROR1 is expressed on hematogones; a minor subpopulation of precursor B-cells (≤0.25% of normal marrow) that are CD45-dimCD10+CD19+, similar to pre-B ALL. Their numbers are higher in pediatric marrow S/P myeloablative Rx.
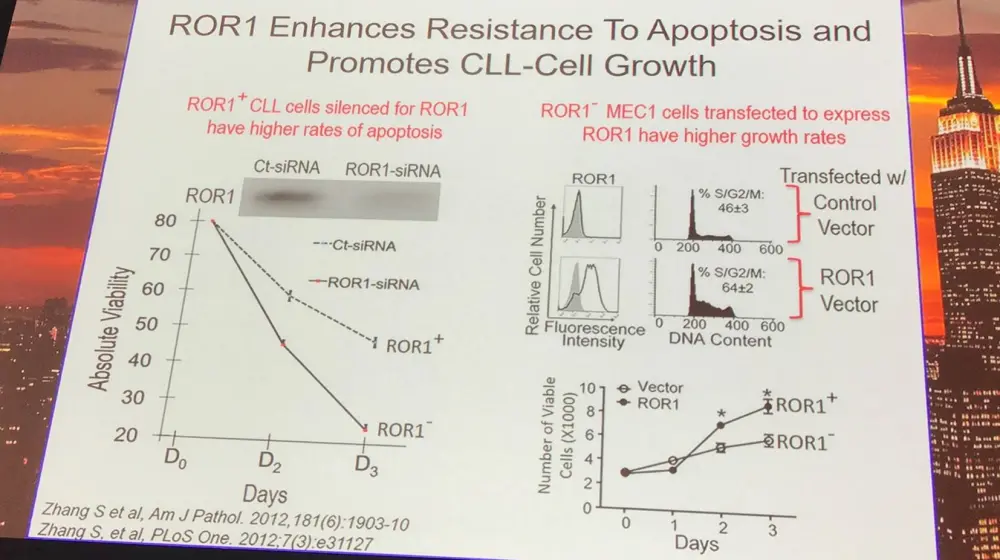
The extracellular domain of ROR1 has been reported to bind with Wnt5A, inducing non-canonical Wnt signaling and promoting CLL-cell proliferation, migration, and survival. ROR1 also enhances disease progression in vivo.
Early gene therapy trials in CLL found that autologous CLL vaccines could induce host anti-leukemia responses; some patients who responded well produced anti-CLL antibodies, which reacted to ROR1 and blocked Wnt5a signaling. This resulted in an anti-CLL activity independent of antibody-dependent cytotoxicity. UC-961 (cirmtuzumab) is a high-affinity, humanized, anti-ROR1 monoclonal antibody that blocks ROR1-dependent Wnt5a signaling.
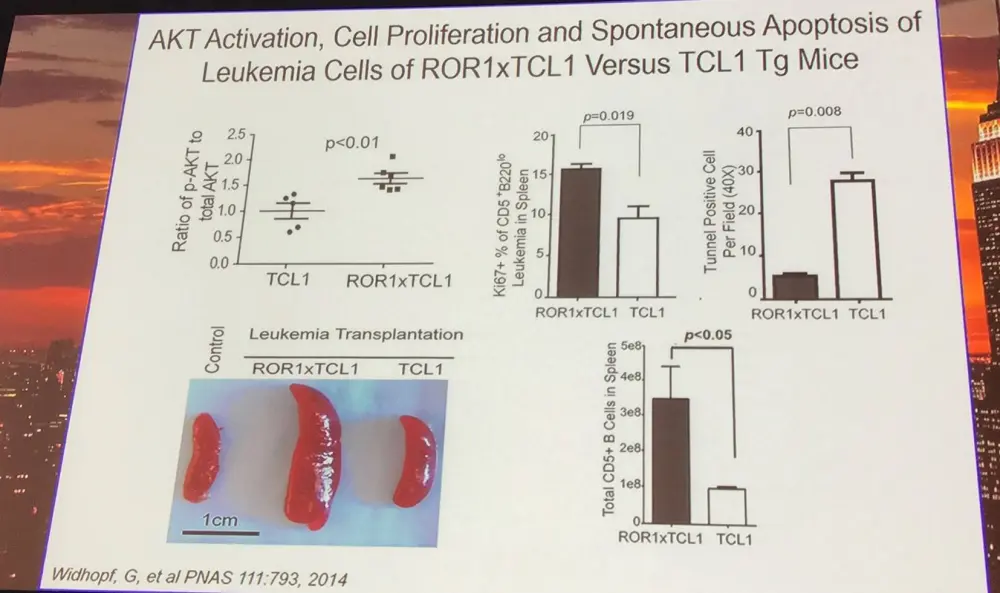
In TCL1 transgenic mice, ROR1 interacts with TCL1 an accelerated CD5+ B-cell lymphomagenesis. Moreover, in ROR1xTCL1 vs. TCL1 leukemia cells, genes which contribute to tumor cell viability are increased whereas those for tumor cell adhesion are decreased.
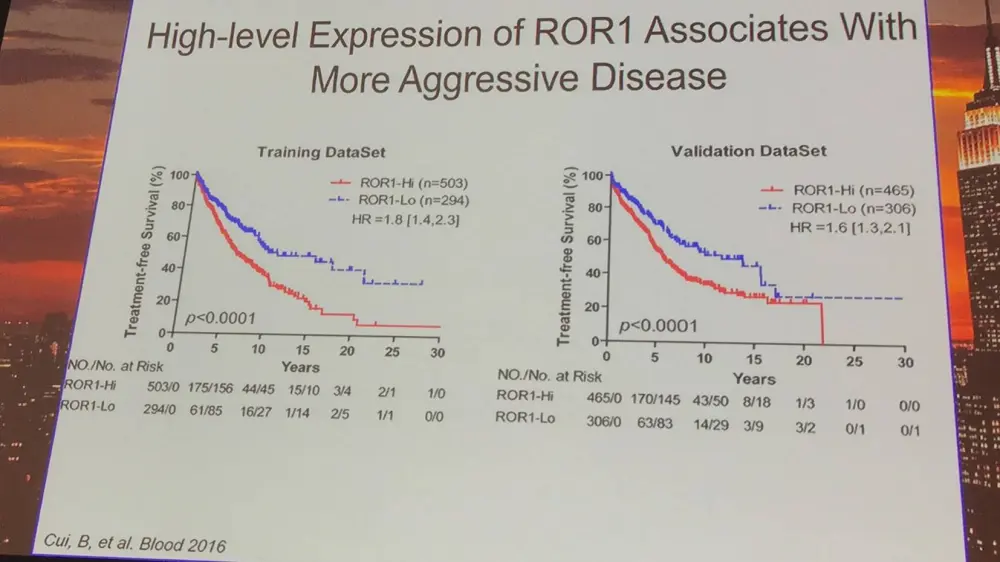
Additionally, Cui et al. found that the expression level of ROR1 on cells differs between patients; higher expression of ROR1 is associated with more aggressive disease.
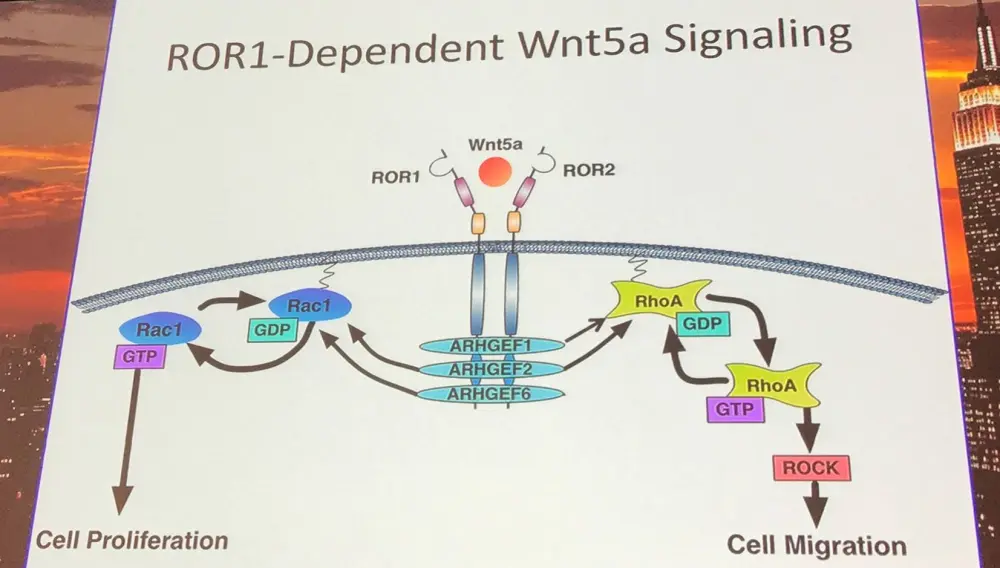
Wnt5a induces Rac1 and RhoA, as well as enhances CLL proliferation and migration, which can be blocked by anti-ROR1 (Yu et al. 2016).
ROR1 associates with 14-3-3ζ, which is encoded by YWHAZ on chromosome 8 and plays a key role in a number of cancers. It takes the form of approximately 30kDa homo- or heterodimers; each monomer has 9 antiparallel alpha helices and 4 of these form an amphipathic binding site. It interacts with AKT1, p53, Raf kinases, and many pro-apoptotic proteins such as BAX, BAD, NOXA, and caspase-2. It serves as a central player in many signal pathways controlling apoptosis, transcription, metabolism, cell cycle, and cellular senescence. Currently under development are synthetic/natural inhibitors that interfere with 14-3-3ζ-client interactions. ROR1 serine-857 is needed for binding to 14-3-3ζ. It has been found that Wnt5a induces association of ROR1 with ARFGEF2 via 14-3-3ζ. Additionally, in MEC1-ROR1 cells, knock-out of 14-3-3ζ impairs activation of RhoGTPases and engraftment.
Injections of UC-961 are well tolerated with no dose limiting toxicities reported. Primarily stable disease at low and brief dosing, while still achieving biological and clinical activity: redistributive lymphocytosis 100% to 50%), reduction of marrow infiltrate (>90% to <30%), and decrease in lymph node size (sum: 32.8 to 25.3cm2).
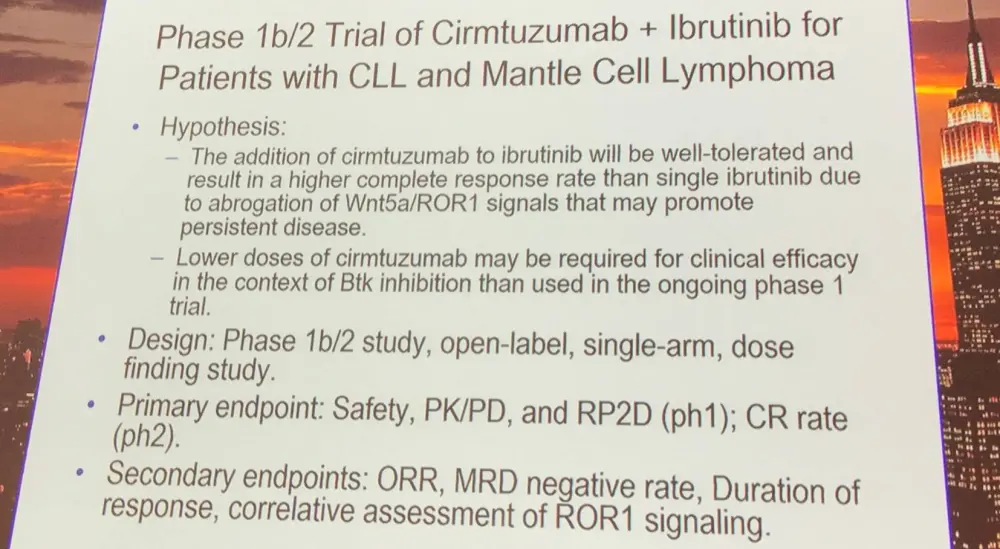
Ibrutinib cannot inhibit the capacity of Wnt5a to enhance CLL proliferation in response to CD154 and IL-4/10. However, there is potential for synergistic activity of ibrutinib and cirmtuzumab; the combination clears engrafted ROR1+ leukemia cells in mice.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?