All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | Final results of the phase II ICLL03 RICAC-PMM trial of RIC allo-SCT for high-risk patients
On 15th May 2017, during iwCLL, the second half of the “Additional Therapies for the Relapsed/Refractory CLL Patient” session was jointly chaired by Guillermo Dighiero (Unité d'Immunohématologie et d'Immmunopathologie, Institut Pasteur) and Federico Caligaris-Cappio (Università Vita-Salute San Raffaele).
Olivier Tournilhac, MD, PhD, from CHU Estaing, Clermont-Ferrand, France, gave a talk titled “RIC allogeneic stem cell transplantation for high risk CLL followed by pre-emptive MRD-based immune intervention. Phase II ICLL03 RICAC-PMM trial: final results” during this session.
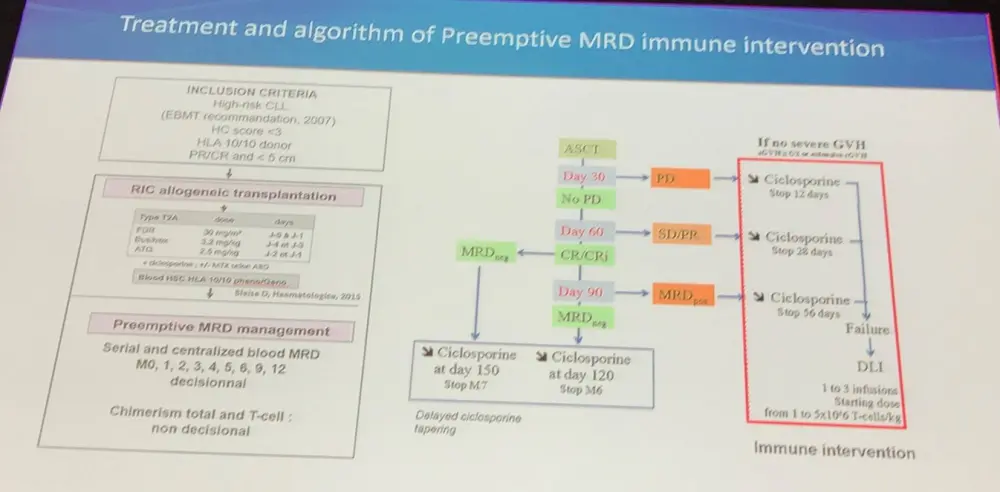
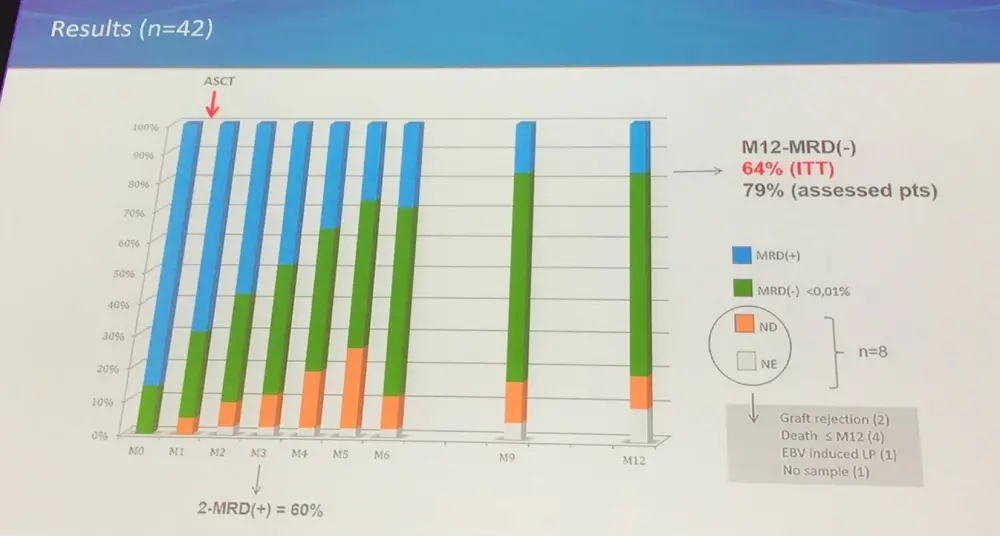
The ICLL003 RICAC-PMM study (NCT01849939) is a multicenter, phase II study by the FILO and SFGM-TC groups, and aimed to increase the rate of MRD-negativity at 12 months post-ASCT using a pre-emptive, MRD based, immune intervention algorithm. MRD-negativity was assessed by 10 color flow cytometry, and was defined as <0.01% (10-4) in blood and bone marrow. Between September 2012 and February 2015, 43 patients were included from 16 centers in France; 42 patients were included in the analysis (1 patient had no ASCT, due to donor comorbidities).
At transplantation:
- Median age = 58 years (range, 40–68)
- Time from diagnosis to transplant = 4.4 years (range, 0.2–14.7)
- Median number of prior therapies = 2 (range, 1–5) including at last line: alemtuzumab (n=17), immunochemotherapy (n=21), and BCR inhibitor (n=4)
- Response: PR = 78%; CR/CRi = 22%
- Pre-ASCT MRD = 0.78% (0.005–70) and undetectable in 6 patients
- Allogeneic transplantation per the EBMT 2007 criteria
|
*including 1 patient with complex karyotype but 17p deletion, eventually ruled out (TP53 wild type) |
|
|
Del(17p) first-line* |
11 (26%) |
|
Del(17p) R/R |
16 (38%) |
|
Relapse <2 years, following fludarabine combination and no del(17p) |
15 (36%) |
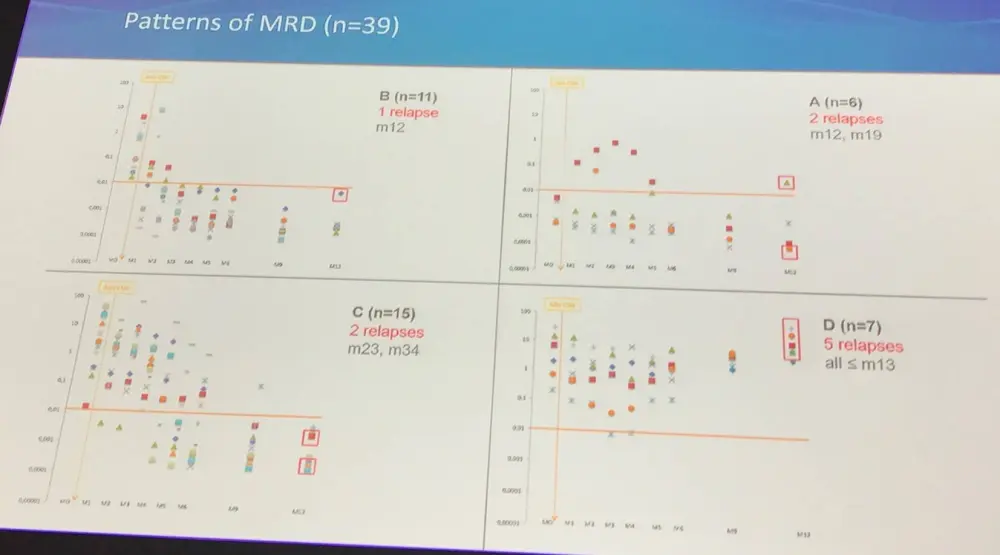
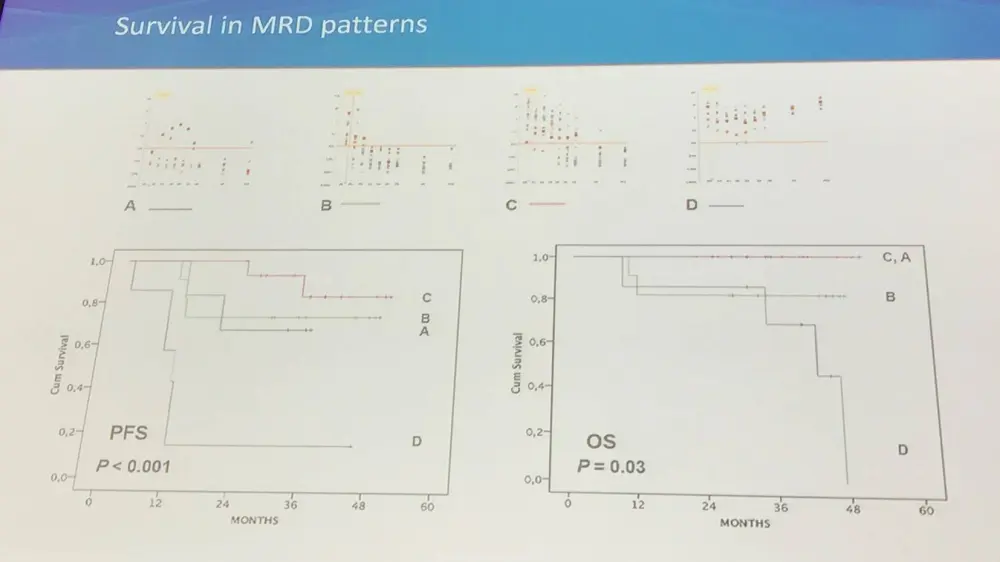
A: M0 MRD(-); B: M0 MRD (+), no need of immune intervention; C: M0 MRD(=), immune intervention - CSA withdrawal; D: M0 MRD(+), immune intervention – CSA withdrawal and DLI
At 24 months:
- Follow-up = 36 months (19–53)
- PFS = 66.7% (95% CI, 51.5–79.0%)
- OS = 90.5% (95% CI, 77.9–96.2%)
- NRM = 7.1% (95% CI, 3.1–11.1%)
- 7 deaths reported, 4 due to toxicity and 3 due to Richter syndrome
In terms of safety:
- aGvHD ≥Grade 2 in 26% of patients; Grade 3 in 10%
- Limited cGvHD in 38% of patients (95% CI, 23–53); Extensive cGvHD in 23% of patients (95% CI, 10–36)
- Including cGvHD in 2 patients following immune intervention (n=1 DLI, n=1 CSA withdrawal)
- 4 toxic deaths reported (CMV/EBV in month 1, GvHD in months 6 and 10, and pulmonary aspergillosis/pneumocystosis infection in month 9)
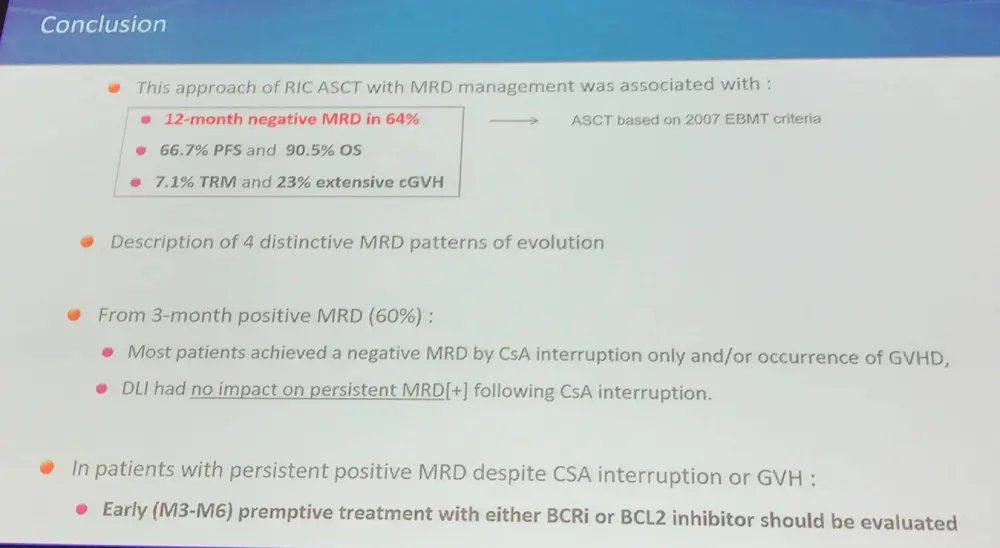
Olivier Tournilhac concluded his talk with a concise summary slide:
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?