All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | Allogeneic transplantation using HLA-compatible donors is effective in younger high-risk CLL patients - an EBMT registry study
On 15th May 2017, during iwCLL, the second half of the “Additional Therapies for the Relapsed/Refractory CLL Patient” session was jointly chaired by Guillermo Dighiero (Unité d'Immunohématologie et d'Immmunopathologie, Institut Pasteur) and Federico Caligaris-Cappio (Università Vita-Salute San Raffaele).
During this session, Michael van Gelder from Maastricht University Medical Center, The Netherlands, gave a presentation titled “Allogeneic hematopoietic stem cell transplantation using HLA-compatible donors in younger high cytogenetic risk CLL patients results in very high long-term Progression-Free Survival and Low Non-Relapse Mortality and may therefore favorably compete with the sequential use of kinase- and BCL2 inhibitors – a report From the CMWP of EBMT.”
Current preferred treatment option for R/R CLL include:
- Kinase inhibitors: ibrutinib, idelalisib+rituximab
- BCL2 inhibitors: venetoclax
These achieve very high responses; however, relapses remain especially in high-risk CLL:
- Del(17p), TP53 mutation or del(11q) (median PFS with ibrutinib is 26 months)
- Up to 33% progress with Richter’s transformation
High-risk CLL patients generally respond to kinase and BCL2 inhibitors, either immediately or after failure on ≥1 kinase and/or BCL2 inhibitors. Short PFS has been reported after sequential use of kinase and/or BCL2 inhibitors.
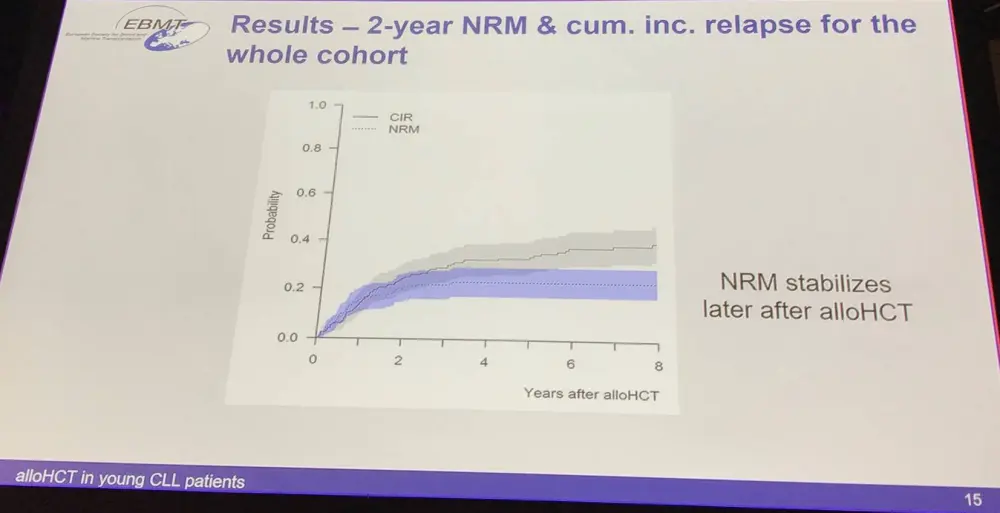
Allogeneic Hematopoietic Stem Cell Transplant (alloHCT) can result in very long PFS, independent of cytogenetics. But, Non-Relapse Mortality (NRM) is a downside; it depends on age, performance, remission status at time of alloHCT, HLA match and donor-patient relation, sex-mismatch, etc.
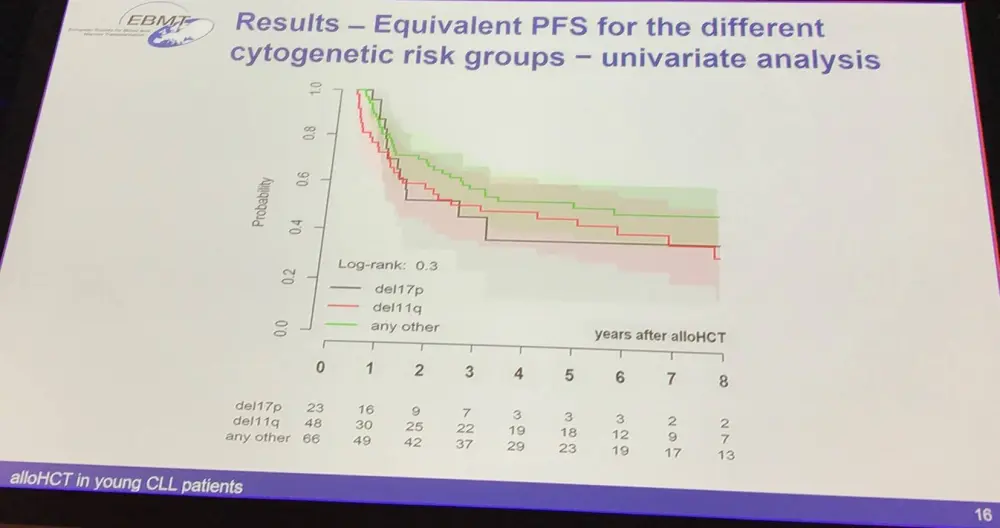
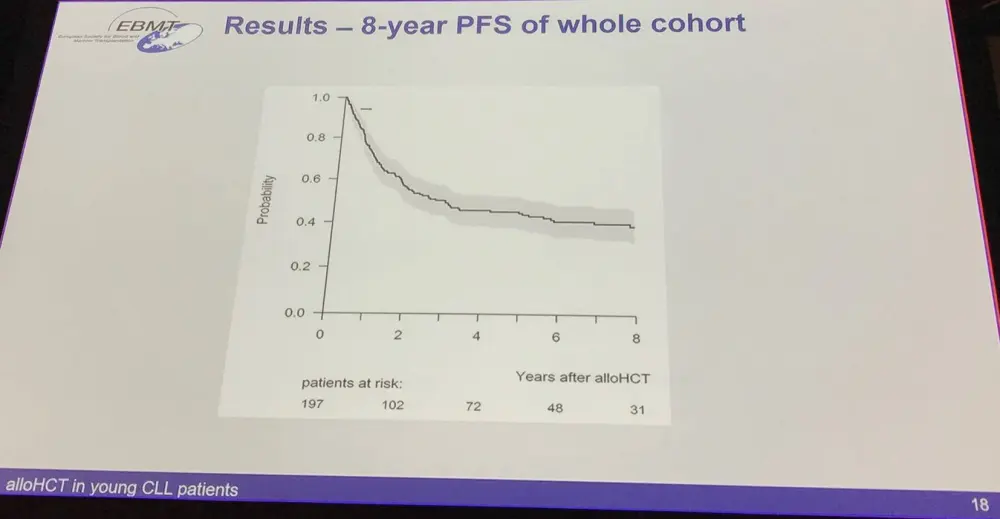
EBMT registry data of transplanted CLL patients was analyzed and focused on younger (<50 years old) high-risk CLL patients and aimed to identify factors that predict low 2-year NRM and high 8-year PFS. It also aimed to study the impact of del(17p)/del(11q) on PFS. Median follow-up was 90.4 months.
Patient and disease characteristicsRisk factor
Numbers
Age (years)
<45 years
80 (41%)
45–50 years
117 (59%)
Median
46 years
Prior Chemosensitivity
Purine-analogue refractory
67 (40%)
Relapse after chemo-immunotherapy
32 (19%)
Cytogenetics
Del(17p)
23 (17%)
Del(11q) and no del(17p)
48 (35%)
Median number of prior lines of therapy (range)
3 (0–10)
Previous autologous HCT
24 (12%)
Responsiveness at time of alloHCT
114 (62%)
Karnofsky (n=179)
90–100
152 (84%)
≤80
29 (16%)
Transplant characteristicsRisk factor
Numbers
Conditioning (n=194)
Non-myeloablative (2Gy TBI-based)
58 (30%)
Reduced intensity
89 (46%)
Myeloablative
47 (24%)
Donor type
Matched related
83 (42%)
Match unrelated
97 (49%)
Partially mismatched unrelated
17 (9%)
Patient-donor sex match (n=193)
Female donor for male patient
39 (20%)
CMV IgG in patient (n=180)
Positive
69 (38%)
Risk factor
HR (95% CI)
p-value
Age (in decades)
0.8 (0.4–1.6)
0.55
Cytogenetics
No del(17p) or del(11q)
1
Del(17p) and/or del(11q)
1.3 (0.6–2.9)
0.51
Donor type
HLA-identical sibling
1
Matched unrelated
2.5 (1.1–5.4)
0.03
Partially matched unrelated
4.0 (1.4–11.6)
0.01
Sex match
All other combination
1
Female donor for male patient
1.5 (0.7–3.3)
0.27
Risk factor
HR (95% CI)
p-value
Donor type
HLA-identical sibling
1
Matched unrelated
1.2 (0.8–1.8)
0.41
Partially matched unrelated
2.8 (1.5–5.2)
<0.01
Sex match
All other combination
1
Female donor for male patient
1.2 (0.7–1.9)
0.50
Using the Cox models for 2- and 8-year PFS:
Defining good and poor transplantation risk patientsGood risk patients
Poor risk patients
46 years old
Del(17p) and/or del(11q)
No prior autoHCT
Remission at the time of alloHCT
No remission at the time of alloHCT
HLA-matched sibling
No sex mismatch
Unrelated female donor
In conclusion, low-NRM risk factors can be identified (good transplant risk). Good transplant risk young CLL patients have a fairly good outcome: very low NRM and 8-year PFS of more than 50%.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?