All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | Baseline left atrial abnormality independently predicts atrial fibrillation in CLL patients treated with ibrutinib
On 14th May 2017, during iwCLL, the fifth session took place titled “Additional Considerations for the Initial Treatment of CLL.” This session was chaired by Richard Furman (Weill Cornell) and Jae Park (Memorial Sloan Kettering Cancer Center).
During this session, a talk titled “Left Atrial Abnormality as a Predictor of Ibrutinib-Associated Atrial Fibrillation in Patients With Chronic Lymphocytic Leukemia: a Predictive Model” was given by Anthony Mato from the Hospital of the University of Pennsylvania, Philadelphia, PA, USA.
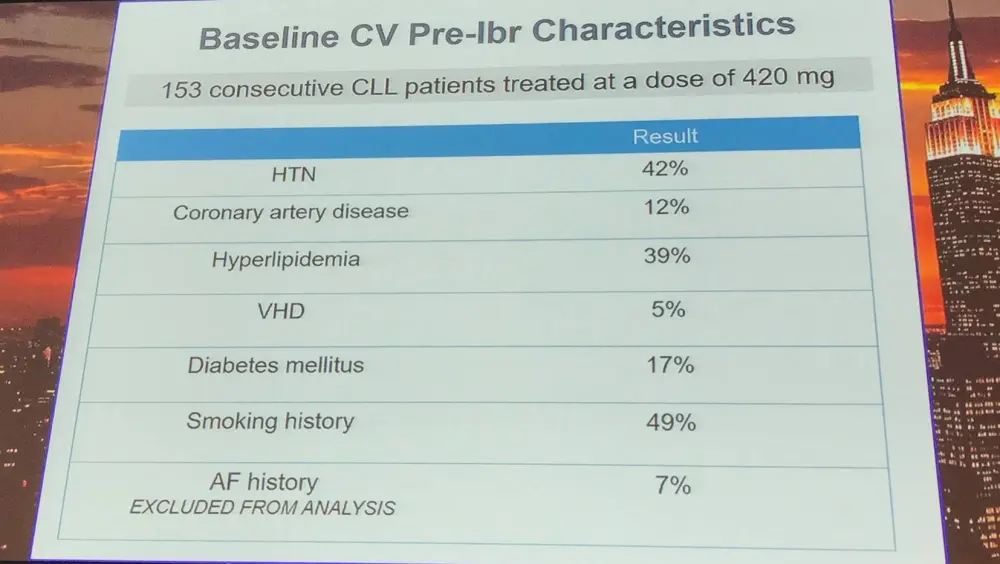
Results from long-term follow-up data indicate an approximate incidence of Atrial Fibrillation (AF) of 9–11% in CLL patients treated with ibrutinib. AF is the most frequent cause of ibrutinib interruption or discontinuation. Patients with AF are also more likely to experience Congestive Heart Failure (CHF), embolic Cerebrovascular Accident (CVA), and bleeding events. A higher risk of AF is associated with Hypertension (HTN), older age, mitral valve disease, and CHF. Left Atrial Abnormality (LAA) detected by ECG indicates remodeling of the left atrium (fibrosis, microscopic myocyte hypertrophy), which has been associated with AF development.
Anthony Mato presented results from a case-controlled, retrospective study of patients with CLL treated at two centers. Patients with pre-ibrutinib AF, no pre-treatment ECG, and receiving less than 420mg ibrutinib daily were excluded. The primary outcome was AF during ibrutinib therapy and secondary outcomes included time from ibrutinib exposure to AF, incidence of ibrutinib-associated HTN, and the association between baseline cardiovascular characteristics and AF.
Overall, 153 consecutive patients with CLL were treated at a dose of 420mg ibrutinib:
|
Characteristic |
Result (range) |
|---|---|
|
Median age at diagnosis |
61 |
|
Median age at ibrutinib initiation |
70 |
|
Media prior therapies |
2 (0–10) |
|
R/R CLL |
87% |
|
Del(17p) |
28% |
|
Del(11q) |
32% |
|
Complex karyotype (≥3) |
35% |
|
Median follow-up |
17 months |
|
Median time from diagnosis to ibrutinib |
73 months |
In total, 44 patients with pre-ibrutinib ECG were selected for LAA analysis: 20 cases and 24 controls. On univariate and multivariate analysis, baseline LAA independently predicted ibrutinib-associated AF:
- Univariate: OR = 9.1 (95% CI, 2.2–37.3; P = 0.002)
- Multivariate: OR = 6.6 (95% CI, 1.5–29.2; P = 0.01)
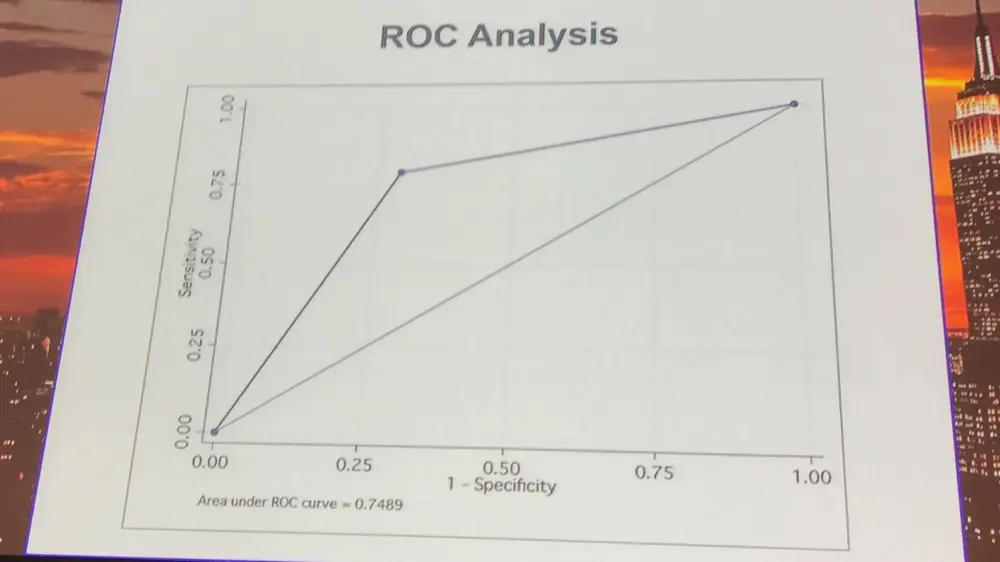
The test characteristics of the association between LAA and AF were also presented:
|
Characteristic |
Value |
95% CI |
|---|---|---|
|
Sensitivity |
79% |
54–94% |
|
Specificity |
71% |
49–87% |
|
Positive likelihood ratio |
2.7 |
1.4–5.3 |
|
Negative likelihood ratio |
0.30 |
0.1–0.74 |
|
Positive predictive value |
68% |
45–86% |
|
Negative predictive value |
81% |
58–95% |
No patient required electrophysiological intervention including cardioversion, ablation, or left atrial appendage occlusion device. The methods of AF management carried out during the study were presented:
|
Pharmacologic intervention |
Percentage |
|---|---|
|
ASA or anti-platelet |
40% |
|
Systemic anti-coagulation |
45% |
|
Anti-arrhythmic agent |
45% |
|
Rate control |
90% |
|
ACE/ARB |
40% |
|
Diuretic |
25% |
Anthony Mato then discussed limitations of the study which included the retrospective nature of the study, the fact that the cases and controls were not balanced for baseline cardiovascular characteristics, the small number of AF cases included, and the variable timing of pre-ibrutinib ECG. In addition, the results require validation in prospective studies.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?