All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | Ibrutinib plus FCG induces a higher rate of MRD negative remission in the bone marrow than FCG alone in patients with newly diagnosed CLL/SLL
On 14th May 2017, during iwCLL, the fifth session took place titled “Additional Considerations for the Initial Treatment of CLL.” This session was chaired by Richard Furman (Weill Cornell) and Jae Park (Memorial Sloan Kettering Cancer Center).
Nitin Jain, from the University of Texas MD Anderson Cancer Center, Houston, Texas, USA, gave a presentation titled “Ibrutinib, fludarabine, cyclophosphamide, and obinutuzumab (GA101) (iFCG) for previously untreated patients with Chronic Lymphocytic Leukemia (CLL) with mutated IGHV and non-del(17p)” during this session.
Results of this phase II trial (NCT02629809) were presented; the primary endpoint of the study was CR/CRi with negative MRD in bone marrow.
Eligibility criteria:
- Previously untreated CLL/SLL meeting iwCLL treatment criteria
- Adult patients (≥18 years old)
- Mutated IGHV
- No del(17p) or mutated TP53
- Adequate organ function
- ANC >500/µl
- Platelet >50,000/µl
- ALT and AST ≤2.5 x ULN
- Total bilirubin ≤1.5 x ULN
- GFR ≥30ml/min
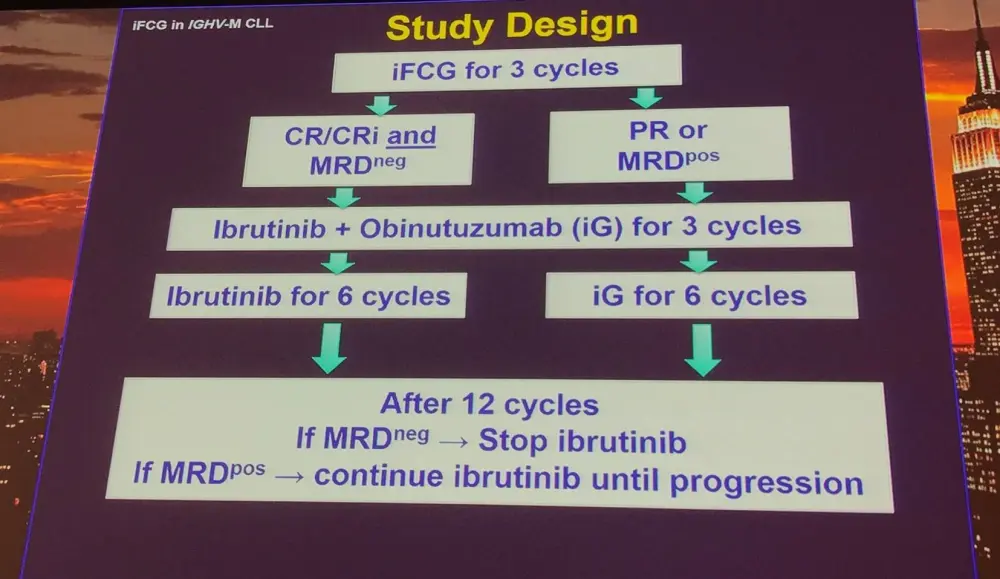
Treatment:
- 3 courses of iFCG:
- Ibrutinib 420mg once daily continuously starting C1D1
- Obinutuzumab 100mg C1D1, 900mg C1D2, 1,000mg C1D8, 1,000mg C1D15, 1,000mg C2D1, 1,000mg C3D1
- Fludarabine 25mg/m2 daily for 3 days each course
- Cyclophosphamide 250mg/m2 daily for 3 days each course
Response evaluation:
Response were measured as outlined by the iwCLL 2008 criteria:
- Blood, marrow, and CT scans: every 3 months during first year, then Q6 months
- Any lymph node >1.5cm on CT: PR
- MRD assessed by 4 color flow cytometry in bone marrow (sensitivity 10-4)
Trial status (9th May 2017):
- The first patients enrolled in April 2016
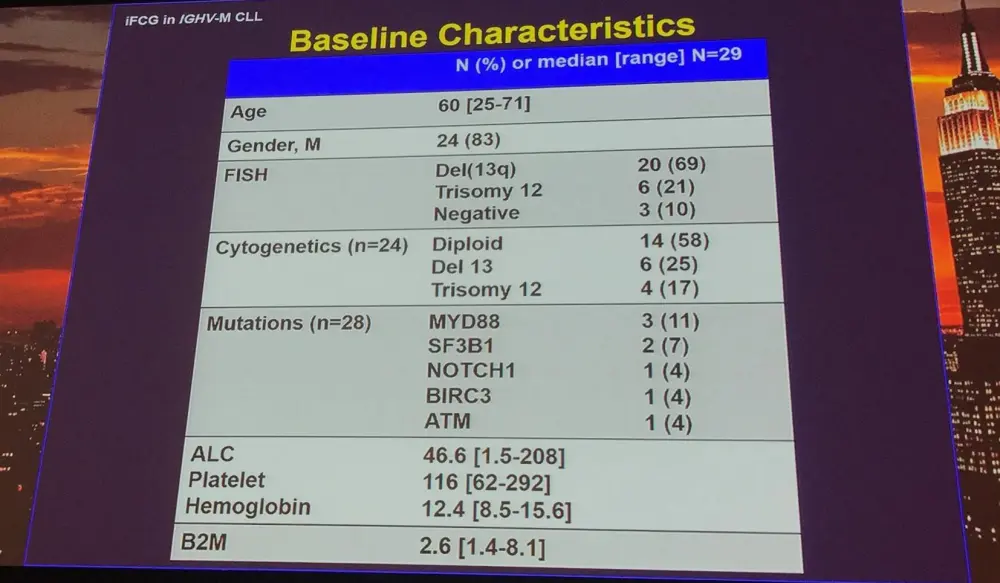
- 29 patients have initiated treatment
- 24 patients have completed 3 cycles of iFCG (1 off study after 3 cycles due to pulmonary MAC infection)
- 4 patients are receiving iFCG cycles
- 1 patient who received C1D1 obinutuzumab (100mg) and one dose of ibrutinib (420mg) is now off study (grade 3 Infusion Related Reaction [IRR] and grade 4 thrombocytopenia)
- Median follow-up = 8.3 months (range, 0.9–13.3)
Clinical response:
|
|
3 months |
|
|---|---|---|
|
|
N=24 (%) |
BM MRD (%) |
|
ORR |
24/24 (100) |
20/24 (83) neg |
|
CR/CRi |
10/24 (42) |
All neg |
|
PR |
14/24 (58) |
10/14 (71) neg |
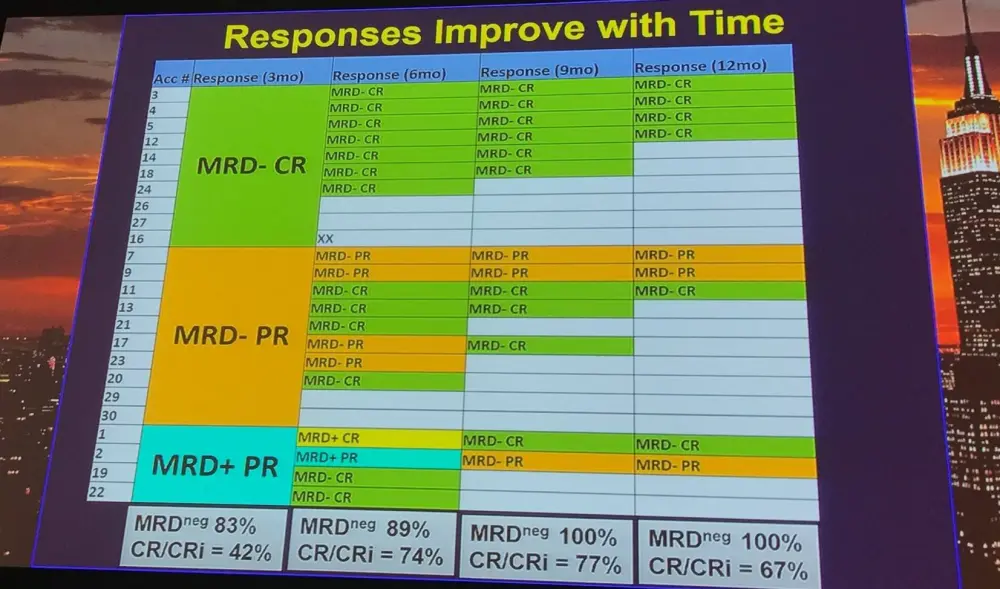
After 3 cycles, a higher proportion of patients treated with iFCG were MRD negative (83%) compared to patients who received FCR (26%).
Moreover, a higher pre-treatment β2M correlated with a lower rate of MRD negativity after 3 cycles of iFCG (P = 0.035):
|
|
n |
BM MRD negativity (%) |
|---|---|---|
|
β2M ≥4 |
6 |
50 |
|
β2M<4 |
18 |
94 |
Toxicities:
|
*9 patients (31%) had grade 2 IRR |
||
|
|
N (%) |
|
|---|---|---|
|
|
G3 |
G4 |
|
Neutropenia |
9 (31) |
12 (41) |
|
Thrombocytopenia |
12 (41) |
1 (3) |
|
ALT/AST |
3 (10) |
1(3) |
|
Atrial fibrillation |
1 (3) |
|
|
Arthralgia |
1 (3) |
|
|
IRR* |
1 (3) |
|
Reported infections included: neutropenic fever (n=4), as well as PCP pneumonia, pulmonary MAC infection, acute cholecystitis, and herpes zoster (n=1 each).
Dose reductions were reported in 57% of patients for FC and 18% of patients for ibrutinib. Treatment delay >2 weeks was reported in 35% of patients (due to thrombocytopenia, transaminitis, and infection).
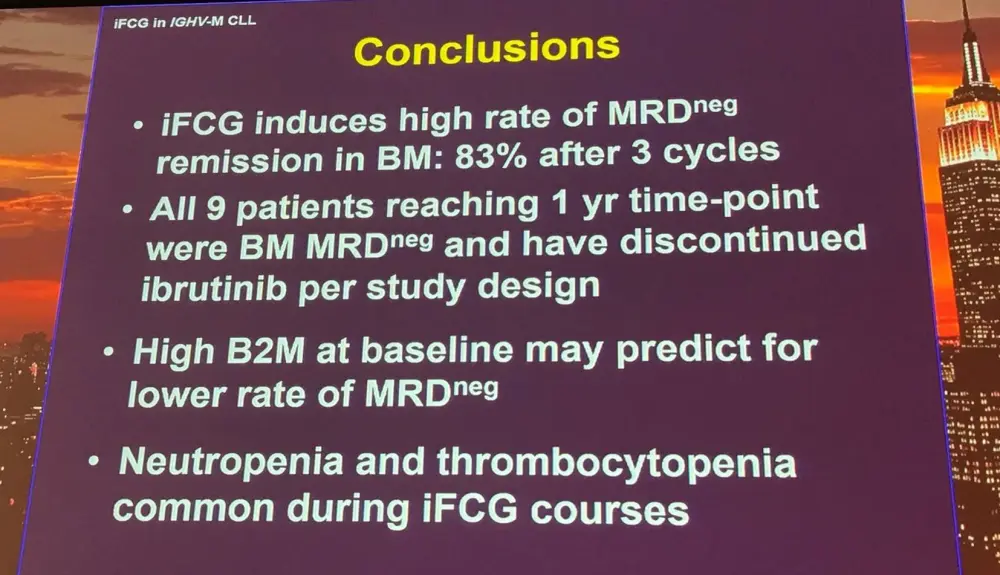
Nitin Jain finished his talk with a concise conclusion slide:
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content