All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Caribou Biosciences, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
Mogamulizumab versus vorinostat in patients with mycosis fungoides and Sézary syndrome: Efficacy and safety based on baseline blood involvement
Mycosis fungoides (MF) and Sézary syndrome (SS) are closely related cutaneous non-Hodgkin T-cell lymphomas. MF is the most common form of cutaneous T-cell lymphoma, with an indolent course that can progress to leukemic disease. SS is rarer and manifests with both skin and blood disease at diagnosis and has poor prognosis. Diagnosis and staging for MF and SS involves assessment of the skin (tumor), lymph nodes, visceral organs (metastasis), and peripheral blood, referred to collectively as TNMB staging. Adaptation to include blood classifications (B0–2 staging) was implemented in 2007, as blood involvement was identified as a prognostic factor.1
Therapeutics are limited, with hematopoietic stem cell transplantation presenting the only potentially curative option, though it is associated with serious risks. Alternatively, the potential for targeted therapies has been explored. Mogamulizumab is a monoclonal antibody that binds and blocks CC chemokine 4 (CCR4) receptors expressed on T cells to prevent trafficking of malignant cells to the skin. The recent phase III MAVORIC trial (NCT01728805) demonstrated greater clinical benefit in relapsed/refractory MF or SS with mogamulizumab compared with vorinostat, a histone deacetylase inhibitor. Further post hoc analysis was recently published by Cowan et al. in the Journal of the European Academy of Dermatology and Venereology, correlating overall response rate (ORR), progression-free survival (PFS), and time-to-next-treatment (TTNT) with the extent of blood involvement at baseline.1
Study Design
MAVORIC study design
The MAVORIC trial was a multicenter, phase III, open-label, randomized controlled study comparing mogamulizumab with vorinostat in patients with relapsed/refractory MF and SS Stages Ib–IVb for whom one prior line of therapy had failed to yield a result.
Patients were randomized 1:1 to receive either mogamulizumab or varinostat:
- Intravenous mogamulizumab (1 mg/kg) was given weekly for the first 28-day cycle, then on Days 1 and 15 of subsequent cycles.
- Oral vorinostat 400 mg was given once daily.
Post hoc analysis
The aim of the post hoc analysis was to assess PFS, ORR, TTNT, skin response, and frequency of treatment-emergent adverse events (TEAEs) in patients in each treatment arm stratified by baseline blood classification B0, B1, or B2. Blood classification was in line with thresholds defined by the international consensus guidelines.
Methods
To assess PFS and ORR, skin and blood were assessed every 4 weeks, with response in blood determined using flow-cytometry. Skin response was assessed using the Modified Severity-Weighted Assessment Tool (mSWAT), a technique that involves assessment of cutaneous T-cell lymphoma lesions (patches, plaques, and tumors) in 12 body regions according to size (using body surface area), multiplying by the assigned weighting factor, and summating for a total mSWAT score.2
Median percentage change in mSWAT per treatment cycle and best overall response by percentage change in mSWAT were examined.
Lymph node and visceral disease were evaluated by computed tomography scans at 4 weeks, then every 8 weeks for the first year, and every 16 weeks thereafter. Tumor cell burden was evaluated each treatment cycle using absolute counts by flow cytometry of CD4+CD7− and CD4+CD26− cells, and CD4:CD8 ratios for each B class.
Results
Patient characteristics
Patient characteristics for each blood involvement level are summarized in Table 1.
Table 1. Patient characteristics*
|
ABC, absolute blood count; MF, mycosis fungoides; Mog; mogamulizumab; SS, Sézary syndrome; T-Score, degree of skin involvement according to TNMB staging; Vor, vorinostat. |
||||||
|
Characteristic, % (unless otherwise stated) |
B0 |
B1 |
B2 |
|||
|---|---|---|---|---|---|---|
|
Vor |
Mog |
Vor |
Mog |
Vor |
Mog |
|
|
Median age (range), years |
58.5 |
56.5 |
65.0 |
61.0 |
68.0 |
69.0 |
|
Female |
30.6 |
43.8 |
45.2 |
29.0 |
49.5 |
44.0 |
|
Disease type |
|
|
|
|
|
|
|
MF |
98.4 |
98.4 |
87.1 |
93.5 |
11.8 |
14.3 |
|
SS |
1.6 |
1.6 |
12.9 |
6.5 |
88.2 |
85.7 |
|
Clinical stage |
|
|
|
|
|
|
|
Ib–IIa |
48.4 |
40.6 |
61.3 |
32.3 |
0 |
0 |
|
IIb–IV |
51.6 |
59.4 |
38.7 |
67.7 |
100 |
100 |
|
T-score |
|
|
|
|
|
|
|
1 |
1.6 |
1.6 |
3.2 |
0 |
2.2 |
0 |
|
2 |
48.4 |
40.6 |
61.3 |
32.3 |
21.5 |
20.9 |
|
3 |
32.3 |
42.2 |
19.4 |
25.8 |
3.2 |
3.3 |
|
4 |
17.7 |
15.6 |
16.1 |
41.9 |
73.1 |
75.8 |
|
ABC CD4+CD7− (/µL), median |
110 |
100 |
200 |
170 |
1,070 |
1,270 |
|
ABC CD4+CD26− (/µL), median |
140 |
130 |
260 |
250 |
2,350 |
2,150 |
|
CD4:CD8 ratio, median |
2.99 |
2.30 |
2.93 |
2.74 |
19.43 |
22.43 |
Survival outcomes based on baseline tumor burden
After a median follow-up of 17 months, PFS was significantly greater for mogamulizumab vs vorinostat in the overall study population (7.70 vs 3.10 months; p < 0.0001). PFS was significantly longer in patients with B1 (8.63 vs 2.53 months; p < 0.0142) and B2 (11.17 vs 3.30 months; p < 0.0001) blood involvement.
PFS was not significantly different between treatment arms (4.70 vs 4.37 months; p = 0.9480) in patients with B0 disease. ORR in the overall study population was significantly greater in the mogamulizumab group compared with the vorinostat group (28.0% vs 4.8%; p < 0.0001). ORR was also significantly greater in patients with B2 involvement for the mogamulizumab arm versus vorinostat (37.4% vs 3.2%). Median TTNT in the overall study population was significantly superior for mogalizumab versus varinostat (11.0 vs 2.5 months; p < 0.0001). TTNT was significantly longer in mogamulizumab-treated patients for blood involvement levels B1 (12.63 vs 3.07 months; p = 0.0018) and B2 (13.07 vs 3.53 months; p < 0.0001).
PFS, ORR, and TTNT outcomes stratified by blood involvement are summarized in Figure 1.
Figure 1. PFS, ORR and TTNT between treatment arms as stratified by blood involvement*
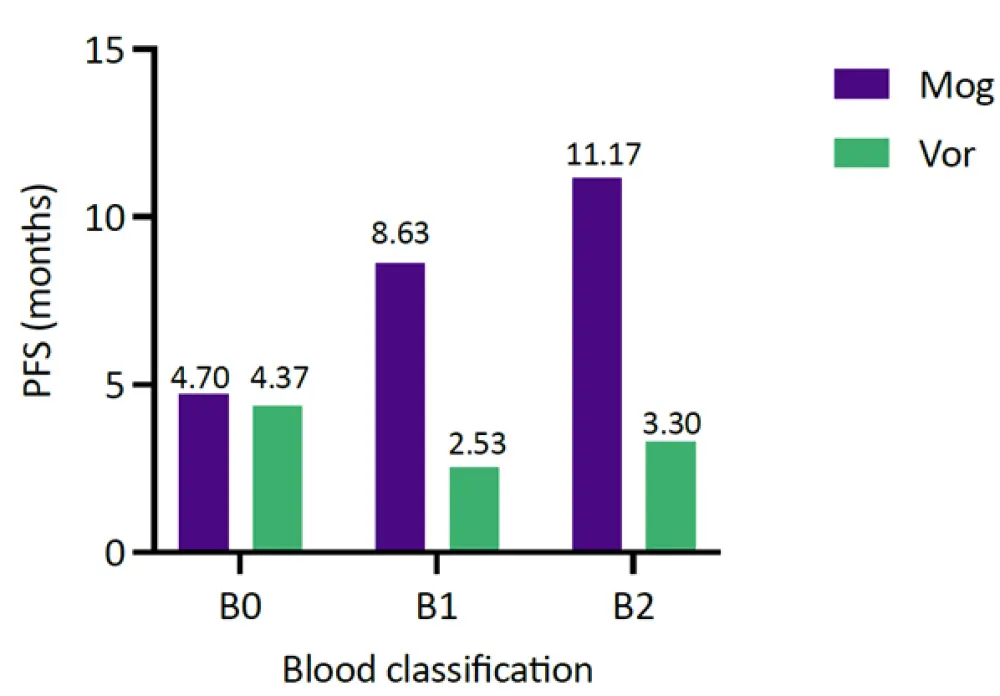
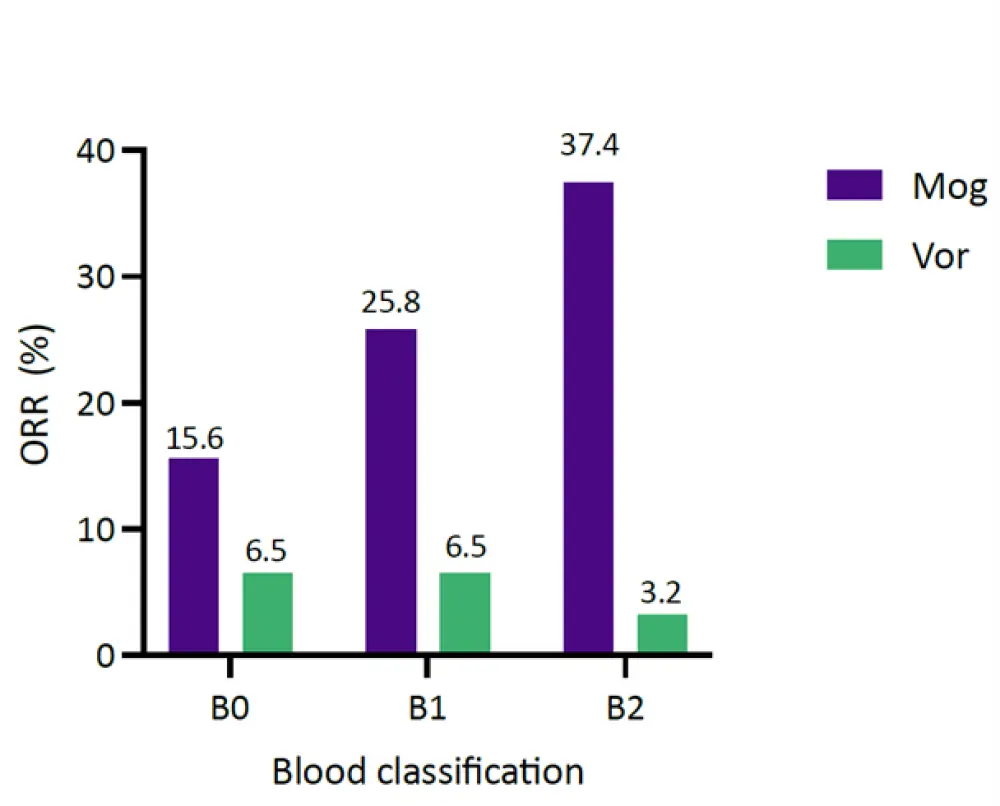
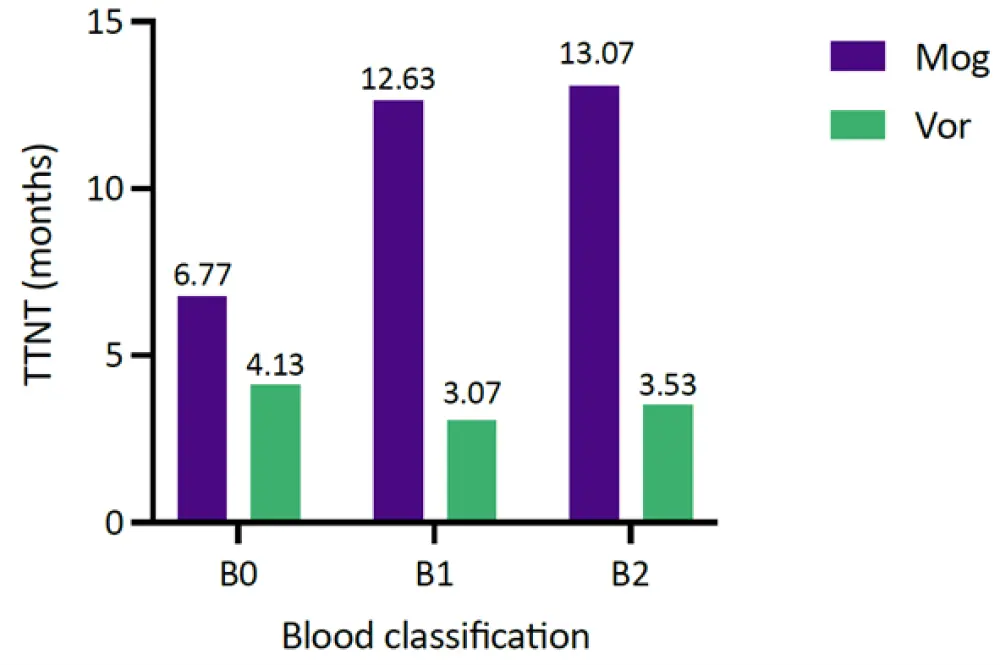
Mog, mogamulizumab; ORR, overall response rate; PFS, progression-free survival; TTNT, time to next treatment; Vor, vorinostat.
*Data from Cowan, et al.1
Skin response
Over 12 treatment cycles, patients treated with mogamulizumab had greater improvement in mSWAT score at B1 and B2 when compared with vorinostat. Further analysis revealed 17.6% of patients with B2 level involvement treated with mogamulizumab had 100% improvement compared with 3.2% of patients treated with vorinostat.
Patients with B1 and B2 blood involvement treated with mogamulizumab had significantly greater rates of complete and partial response (45.2% vs 56.0%, respectively) compared with patients with B0 involvement (25.0%).
Blood tumor burden
Median absolute CD4+CD26− cell counts were dramatically reduced in Cycle 1 and sustained across all treatment cycles with mogamulizumab compared with vorinostat, irrespective of baseline blood involvement level. Absolute CD4+CD26− cell counts were most significantly reduced in patients with B2 involvement, and these patients also had the largest median percent change in cell counts from baseline.
CD4:CD8 cell ratios were dramatically reduced in Cycle 1 and maintained or improved across all treatment cycles with mogamulizumab treatment in patients with B1 and B2 involvement. In patients with B0 and B1 involvement treated with vorinostat, CD4:CD8 ratios gradually increased across treatment cycles, while patients with B2 involvement had unpredictable responses.
Treatment-related TEAEs
Notably, Grade ≥3 treatment-related TEAEs were more common in vorinostat-treated patients across all blood involvement levels compared with the mogamulizumab treatment arm. Treatment-related TEAEs are summarized in Table 2.
Table 2. Treatment-related TEAEs stratified by blood involvement level*
|
TEAEs, treatment-emergent adverse events. *Data from Cowan, et al.1 |
||||||
|
Treatment-related TEAEs, n (%)† |
Vorinostat |
Mogamulizumab |
||||
|---|---|---|---|---|---|---|
|
B0 |
B1 |
B2 |
B0 |
B1 |
B2 |
|
|
Any grade |
93.5 |
96.8 |
96.8 |
51 |
25 |
80 |
|
Grade ≥3 |
29 |
45.2 |
35.5 |
17.2 |
25.8 |
30.8 |
Three of the 31 patients with B1 involvement in the vorinostat arm had a Grade 5 event; the only Grade 5 event reported in the mogamulizumab arm was for one patient with B2 level involvement. Two out of 184 patients with B2 blood involvement treated with mogamulizumab had tumor lysis syndrome: one Grade 1 and the other Grade 3.
Conclusion
Overall, post hoc analysis of the MAVORIC trial demonstrated improved efficacy in patients with MF and SS treated with mogamulizumab compared with vorinostat when stratified by baseline blood involvement. PFS, ORR, and TTNT were greater for the mogamulizumab arm versus vorinostat, while skin and blood tumor burden improvement was also greater for patients with blood involvement levels B1 and B2. Additionally, mogamulizumab appeared to be safer, with fewer Grade >3 TEAEs.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In patients with R/R LBCL who progress after CAR‑T, which of the following data would most strengthen your confidence in considering BV+R2?