All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Phase I results suggest a tolerable safety profile for avadomide and obinutuzumab in patients with R/R B-cell NHL
Featured:
 Gilles Salles
Gilles SallesRelapsed and/or refractory (R/R) disease is not rare in patients with non-Hodgkin lymphoma (NHL), and poor prognosis frequently makes the treatment of these patients a challenge. Cereblon modulators induce degradation of transcription factors, such as zinc finger proteins Ikaros and Aiolos, and the cereblon modulator lenalidomide has demonstrated synergistic clinical antitumour activity in patients with R/R NHL when administered in combination with an anti-CD20 monoclonal antibody.
Jean-Marie Michot et al. conducted a phase 1b study, CC-122-NHL-001 (NCT02417285), to investigate the safety and activity of a next-generation cereblon modulating agent, avadomide (CC-122), in combination with obinutuzumab, an anti-CD20 monoclonal antibody. The trial was carried out in patients with R/R B-cell NHL who had not previously received lenalidomide, or were refractory to lenalidomide. Study results have been recently published in The Lancet Haematology, and here we summarize the key points.1
Study design
- This was a multi-center, phase Ib dose escalation and dose expansion study (see Table 1).
- The dose expansion phase was done at a recommended phase II dose and excluded patients with R/R diffuse large B-cell lymphoma (DLBCL).
Table 1. A summary of inclusion criteria for dose escalation and expansion phases1
|
FL, follicular lymphoma; NHL, non-Hodgkin lymphoma; R/R, relapsed/refractory. |
|||
|
|
Dose escalation (n = 38) |
Dose expansion (n = 35) |
|
|---|---|---|---|
|
Inclusion criteria |
CD20+ tumor |
CD20+ tumor |
|
|
Confirmed B-cell NHL |
Confirmed FL (Grade 1, 2, or 3a) |
||
|
R/R NHL with > 2 previous standard therapy regimens* or autologous stem-cell transplantation† |
R/R disease following > 1 previous standard systemic regimen‡ |
||
|
R/R indolent NHL following > 1 previous standard systemic regimen‡ |
FL1 cohort (n = 4) R/R FL following > 2 cycles of lenalidomide-based therapy |
FL2 cohort (n = 31) Patients with R/R FL who were lenalidomide-naïve and received > 1 standard therapy |
|
- Eligibility criteria were as follows:
- Aged ≥ 18 years
- Measurable disease (with at least one lesion > 1.5 cm in the transverse diameter)
- Eastern Cooperative Oncology Group (ECOG) performance status of 0–1
- Sufficient hematological, hepatic, and renal function
- The expansion part did not include patients with DLBCL according to the preliminary safety and efficacy data obtained during phase Ia.
- Primary endpoint was safety and tolerability of the combination. Secondary endpoints included preliminary antitumor activity through tumor response, duration of response, and progression-free survival (PFS), and the pharmacokinetic parameters of avadomide.
Study treatments
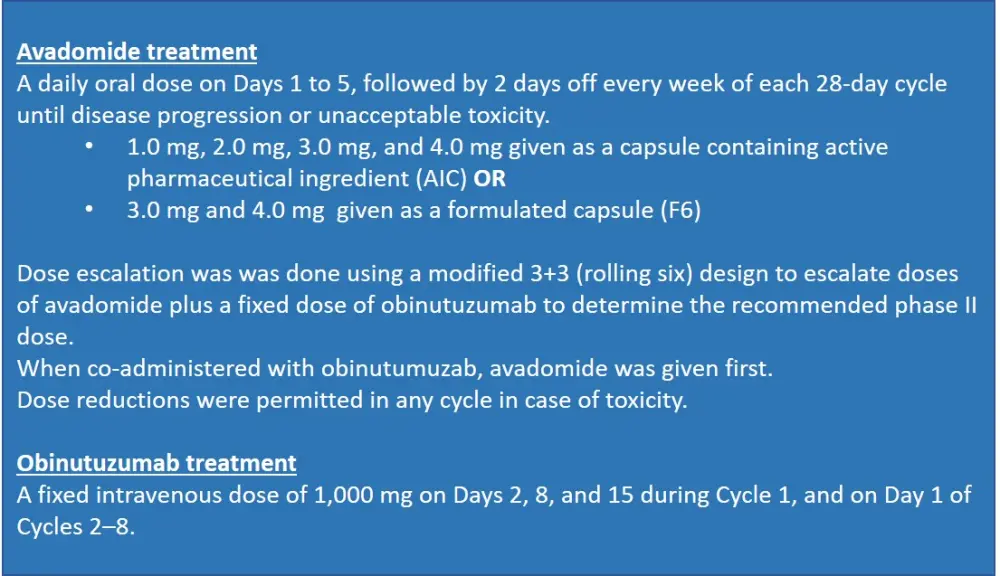
Avadomide and obinutuzumab administration is detailed in Figure 1. Granulocyte colony-stimulating factor (G-CSF) prophylaxis was not allowed, however, G-CSF support was used to treat neutropenia.
Figure 1. Study treatments1
Patients
By the cutoff date of March 27, 2019, a total of 73 patients had been treated. The median age was 61 years (range, 26–83), with 37% of patients (n = 27) being > 65 years old. More than half (58%) of the patients had advanced stage (III–IV) disease. Patient characteristics are provided in Table 2.
Table 2. Baseline characteristics
|
DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma. |
|
|
Characteristic |
Study population (N = 73) |
|---|---|
|
Disease type |
n (%) |
|
FL Bendamustine refactory Rituximab refractory Double refractory* Early relapse† Standard risk High risk FL DLBCL Marginal zone lymphoma |
53 (73) 3 (6) 26 (49) 16 (30) 17 (32) 31 (58) 22 (42) 19 (26) 1 (1) |
|
Previous stem-cell transplantation Patients with FL Patients with DLBCL |
26 (36) 17 (23) 9 (12) |
|
Bone marrow involvement |
13 (18) |
|
Number of previous systemic treatments |
|
|
Median, n (range) 1 2 > 2 |
3 (1–11) 8 (11) 22 (30) 43 (59) |
Results
Of the 73 patients who received study treatment, 30% were still on treatment at the cutoff date. The median treatment durations for avadomide and obinutuzumab were 30 weeks (range, 1–172) and 28 weeks (range, 1.1–34), respectively. Correspondingly, median number of treatment cycles for avadomide and obinutuzumab in the escalation phase were 7.5 and 6.5, respectively.
Safety
At least one dose interruption was observed in most patients (90%). The most common reason for dose reduction was adverse events (AEs). 29% of patients required one dose reduction, while 10% required two reductions. Seven patients discontinued treatment due to diarrhea, worsening of fatigue, toxoplasmosis, secondary tumor, and colitis, which were suspected to be related to avadomide treatment. Dose-limiting toxicities included Grade 4 neutropenia (n = 1 in the 3.0 mg AIC cohort; see Figure 1), Grade 3 sepsis (n = 1 in the 3.0 mg F6 cohort; see Figure 1), and Grade 5 tumor flare (n = 1 in 4.0 mg F6 cohort). Most treatment-emergent AEs were Grade 1/2 in severity. The ten most common AEs of any grade were:
- diarrhea (30% Grade 1–2; 3%, Grade 3)
- pyrexia (27% Grade 1–2; 1% Grade 3)
- asthenia (27%, Grade 1–2)
- constipation (21%, Grade 1–2)
- cough (21%, Grade 1–2)
- muscle spasms (19%, Grade 1–2)
- thrombocytopenia (18% Grade 1–2; 19% Grade 3; 4% Grade 4)
- anemia (18% Grade 1–2; 5% Grade 3)
- bronchitis (18% Grade 1–2; 1% Grade 3)
- nausea (16%, Grade 1–2).
In the dose escalation phase, the maximum tolerated dose and the non-tolerated dose were not established. Therefore, based on safety and pharmacokinetic–pharmacodynamic data, the Safety Review Committee established the recommended phase II dose: an oral dose of 3.0 mg avadomide given on a 5–7-day dosing schedule in combination with 1,000 mg obinutuzumab (intravenous) given on Days 2, 8, and 15 in Cycle 1 and on Day 1 in Cycles 2–8.
A summary of safety analysis results is provided in Table 3.
Table 3. Safety outcomes1
|
AE, adverse event; AML, acute myeloid leukemia; CRS, cytokine release syndrome; SAE, serious adverse event; TEAE, treatment-emergent adverse event. |
||
|
Outcome |
Patients (N = 73) |
|
|---|---|---|
|
Treatment discontinuation, n (%) Disease progression, n AEs, n Physician decision, n Patient withdrawal, n |
51 (70) 28 8 5 4 |
|
|
Deaths,* n |
2 |
|
|
SAEs, n (%) Infusion-related reaction Pyrexia Cytokine release syndrome |
— 5 (7) 4 (5) 4 (5) |
|
|
Patients experiencing avadomide-related SAEs, n (%) Febrile neutropenia Pyrexia Neutropenia |
23 (32) 3 (4) 3 (4) 2 (3) |
|
|
Patients experiencing obinutuzumab-related SAEs, n (%) CRS |
20 (27) 4 (5) |
|
|
Most common Grade 3–4 TEAEs, n (%) |
Grade 3 |
Grade 4 |
|
Neutropenia |
19 (26) |
22 (30) |
|
Thrombocytopenia |
14 (19) |
3 (4) |
|
Most common avadomide-related Grade 3–4 TEAEs, n (%) Neutropenia Thrombocytopenia Pneumonia |
— 16 (22) 11 (15) 4 (6) |
— 21 (29) 1 (1) ― |
|
Most common obinutuzumab-related Grade 3–4 TEAEs, n (%) Neutropenia Thrombocytopenia Infusion-related reactions |
— 17 (23) 8 (11) 4 (6) |
— 15 (21) 3 (4) ― |
Efficacy
- Median duration of follow-up was 253 days.
- Overall response rate (ORR) in all patients was 68% (95% CI, 56.6–78.9) with a median duration of response of 18.9 months (95% CI, 9.7–25.8).
- Both complete and partial response rates were 34% for the entire study population (N = 73), and best response rates among study cohorts are shown in Figure 2.
- ORR in standard-risk and high-risk patients with FL was 81% (range, 62–92) and 68% (range, 45–86), respectively.
- The overall median PFS in all patients was 16.2 months (range, 10.9–22.5), with a median PFS in patients with R/R FL and with R/R DLBCL of 16.6 months (range, 11.4–24.9) and 4.7 months (range, 1.8–13.8), respectively.
- Median PFS was 16.4 months in lenalidomide-naïve patients with R/R FL; it was not reached in four patients who had previously received lenalidomide. The 12-month PFS was 71.9% for lenalidomide-naïve and 75% for lenalidomide-treated patients.
- Tumor volume was reduced in 90% of patients (n = 66) after two cycles of treatment.
Figure 2. Best response rates among study cohorts1
CR, complete response; ORR, overall response rate; PR, partial response.Conclusion
The combination of avadomide and obinutuzumab has demonstrated a safety profile similar to each agent as monotherapy, and AEs were considered manageable and tolerable. The most common treatment-related AEs included thrombocytopenia, neutropenia, diarrhea (avadomide), infusion-related reactions, and pyrexia (obinutuzumab). Preliminary efficacy data were promising with a high ORR seen at all doses, and especially in patients who experienced early relapse. Pharmacokinetic properties of avadomide were dose proportional, and similar to those observed in preclinical studies. Overall, this study may provide a basis for further evaluation of cereblon modulators with novel anti-CD20 antibodies in patients with FL, who relapse or are refractory to rituximab-containing regimens.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?