All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Caribou Biosciences, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
Phase II results: MATRix-RICE therapy and ASCT in DLBCL with secondary CNS involvement
Patients with diffuse large B-cell lymphoma (DLBCL) and dissemination within the central nervous system (CNS) have a very poor prognosis, and the rarity of secondary CNS lymphoma makes randomized studies into treatment options challenging. Secondary CNS lymphoma is often associated with progression of systemic lymphoma, indicating the need for treatments that can penetrate the blood–brain barrier. In order to be curative, chemotherapeutic treatment of CNS lymphoma is usually followed by autologous hematopoietic stem cell transplant (ASCT).
In a prospective single-arm study, Andrés Ferreri and colleagues sequentially combined the standard regimens of MATRix (rituximab, methotrexate, cytarabine, and thiotepa) and RICE (rituximab, ifosfamide, carboplatin, and etoposide) followed by ASCT, to investigate whether this intensive, CNS-directed chemoimmunotherapy has potential as an efficacious and safe treatment option in patients with secondary CNS lymphoma. Here, we summarize key results from this phase II study (MARIETTA, NCT02329080), which were published in Lancet Hematology.1
Methods
This international, single-arm, phase II study included patients from 24 hospitals in Italy, the UK, the Netherlands, and Switzerland. Patients aged 18–70 years, with histologically confirmed DLBCL, CNS involvement at presentation or relapse, and Eastern Cooperative Oncology Group Performance Status (ECOG-PS) ≤ 3 were eligible. Apart from high-dose methotrexate or ASCT, prior treatment for systemic lymphoma was permitted, and patients with high-grade transformation from indolent lymphoma, or double- or triple-hit lymphoma were also included. Exclusion criteria were:
- Previous organ transplantation
- Other forms of immunosuppression
- HIV infection
- Primary CNS lymphoma
Primary outcome was 1-year progression-free survival (PFS). Secondary outcomes were overall and complete response (CR) rate prior to ASCT according to the Revised Response Criteria for Malignant Lymphoma, duration of response, overall survival (OS), and safety. Differences in PFS between patients with CNS dissemination at diagnosis and patients with CNS involvement at relapse were analyzed post hoc.
Treatment regimen
Figure 1 shows a schematic of the treatment schedule used in this study.
Figure 1. Study design (adapted from Ferreri et al.1)
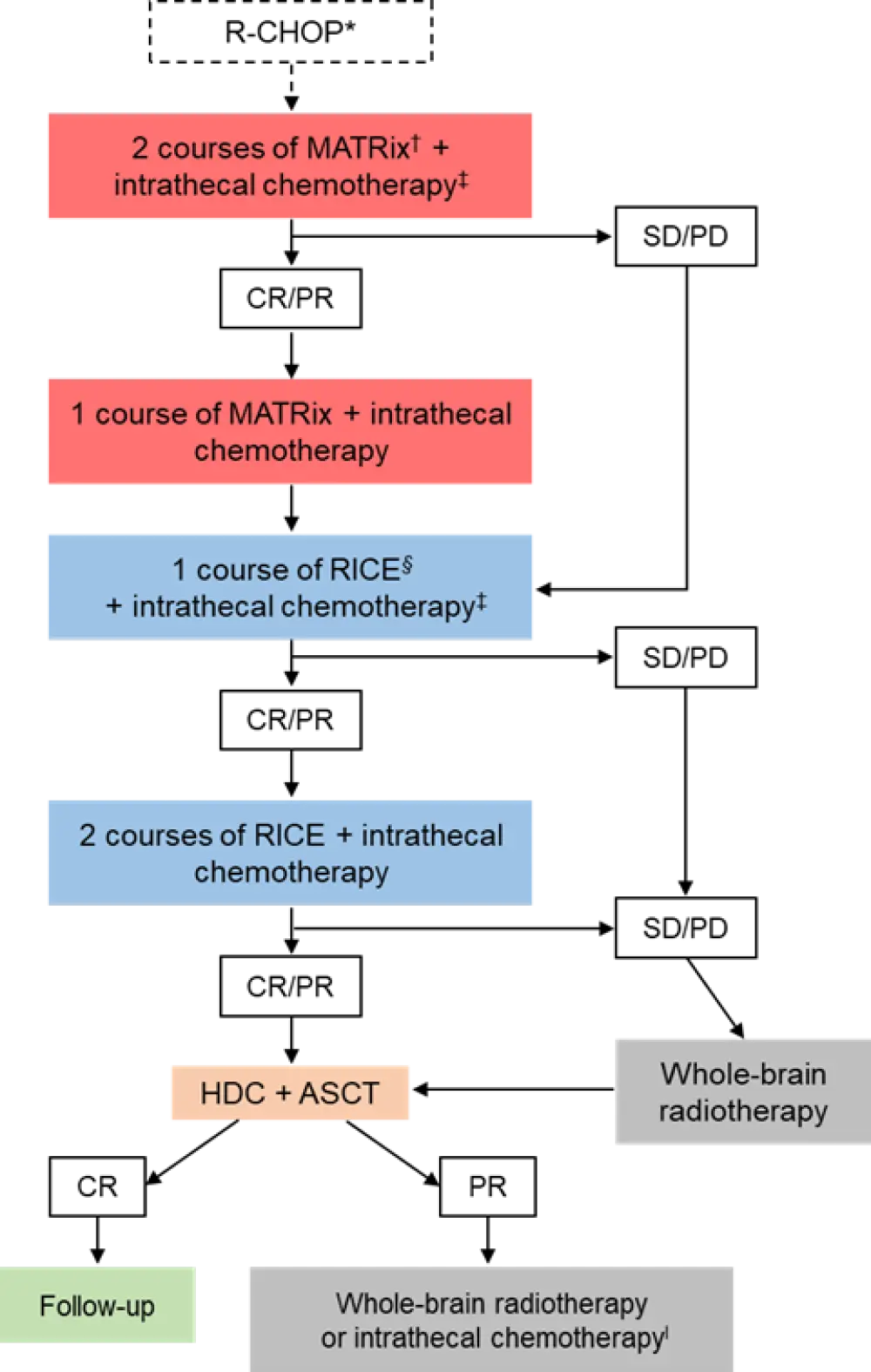
ASCT, autologous hematopoietic stem cell transplant; CR, complete response; CSF, cerebrospinal fluid; HDC, high-dose chemotherapy; PR, partial response; PD, progressive disease; SD, stable disease.
*Chemotherapy-naïve patients with extensive and life-threatening extra-CNS disease initially received 1 or 2 courses of R-CHOP (rituximab 375 mg/m2, cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, and vincristine 1.4 mg/m2 on Day 1, and prednisolone 75 mg on Days 1–5).
†MATRix: rituximab 375 mg/m2 on Day 0, methotrexate 3.5 g/m2 on Day 1, cytarabine 2 g/m² twice daily on Days 2 and 3, and thiotepa 30 mg/m² on Day 4.
‡All patients received intrathecal cytarabine 50 mg or conventional triple-drug chemotherapy (methotrexate 12 mg, cytarabine 50 mg, and hydrocortisone 50 mg) on Day 5 of every MATRix course and on Day 4 of every course of RICE.
§RICE: rituximab 375 mg/m² on Day 1, etoposide 100 mg/m² on Days 1–3, and ifosfamide 5 g/m² with mesna support and carboplatin area under the curve of 5 in 500 mL on Day 2.
ΙPatients with residual disease in brain parenchyma after ASCT received whole-brain radiotherapy. Those with residual disease in CSF after ASCT received additional intensified intrathecal chemotherapy.
Key findings
Overall, 79 patients were enrolled, of which 75 had evaluable data and received the first course of MATRix. Patient characteristics for these patients are shown in Table 1. There were 32 patients with CNS involvement at diagnosis and were therefore naïve to chemotherapy, whereas 43 patients had received prior chemotherapy but subsequently relapsed with either isolated CNS involvement (n = 15) or concomitant CNS and systemic disease (n = 28).
Table 1. Patient characteristics (adapted from Ferreri et al.1)
|
CNS, central nervous system; CSF, cerebrospinal fluid; ECOG-PS, Eastern Cooperative Oncology Group Performance Status; IPI, International Prognostic Index; LDH, lactate dehydrogenase; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone. |
|
|
Characteristics |
N = 75 |
|---|---|
|
Median age, years (range) |
58 (23–70) |
|
Male, n (%) |
38 (51) |
|
CNS disease at enrollment, n (%) |
|
|
IPI, n (%) |
|
|
Prior treatment, n (%) |
43 (57) |
|
Refractory to prior treatment, n (%) |
20 (47) |
Table 2 summarizes patient survival. At one year, 42 patients were progression free, with a PFS of 58%. Survival was improved for patients who received ASCT (PFS, 100%). Univariate analysis revealed that patients with disease localized to the CNS at presentation (71%; 95% CI, 69–73; n = 32) had significantly improved PFS compared to patients with CNS involvement at relapse (28%; 95% CI, 11–47; p = 0.0031; n = 43).
Table 2. Survival rates following MATRix-RICE treatment and ASCT (adapted from Ferreri et al.1)
|
ASCT, autologous hematopoietic stem cell transplant; CI, confidence interval; CNS, central nervous system; IQR, interquartile range; OS, overall survival; PFS, progression-free survival. |
|
|
Outcome |
All patients |
|---|---|
|
1-year PFS, % (95% CI) |
58 (55–61) |
|
Median follow-up, months (IQR) |
29 (20–40) |
|
2-year PFS, % (95% CI) |
46 (39–53) |
|
OS, % (95% CI) |
|
Progressive and relapsing disease was very aggressive, with 25 patients (33%) showing progressive disease at every step of treatment and 11 (24%) of the 46 responders at follow-up experiencing tumor relapse. Median survival after relapse was 1 month (IQR, 1–3).
Secondary endpoints
Response rates are shown in Figure 2. Nine (28%) patients required R-CHOP treatment in the study prior to initiating MATRix. Of the 49 (65%) patients who responded to induction with MATRix-RICE, 29 (39%) obtained a CR and 20 (27%) achieved a partial response, of which eight (40%) had residual CNS disease, six (30%) had residual extra-CNS disease, and six (30%) had both.
Figure 2. Response to MATRix-RICE treatment and ASCT1
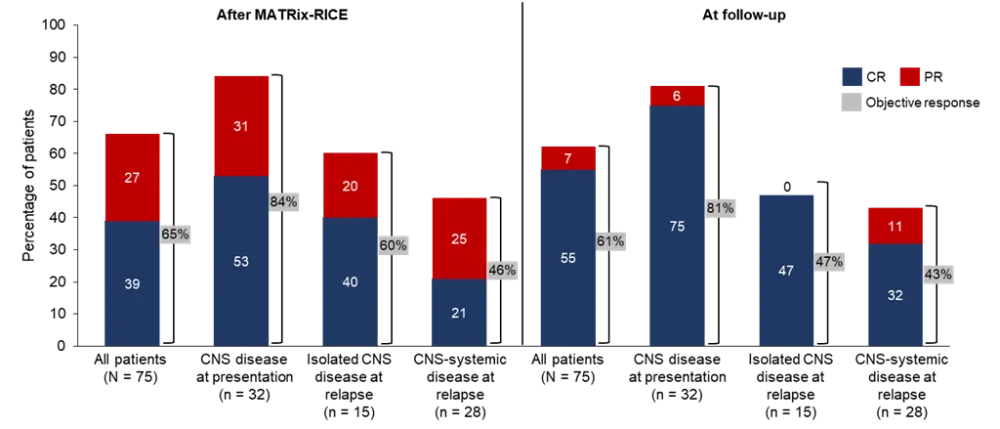
CNS, central nervous system; CR, complete response; MATRix, rituximab, methotrexate, cytarabine, and thiotepa; PR, partial response; RICE, rituximab, etoposide, ifosfamide, and carboplatin.
Twelve of the MATRix-RICE responders were not eligible for ASCT, with four remaining relapse-free at 18–28 months. Of the 37 responders who did advance to ASCT, ten and 12 subsequently achieved a CR and partial response, respectively. Overall, 13 (37%) patients received whole-brain radiotherapy during the study and, of these, seven experienced a complete or partial response.
Of the 46 patients (61%) who had an objective response at the end of study follow-up, 41 (55%) achieved a CR. Median duration of response was 26 months (IQR, 16–37).
Post-hoc analyses
Univariate analysis revealed that 2-year PFS was significantly improved in patients with CNS dissemination at diagnosis (71%; 95% CI, 69–73; n = 32) compared to patients with CNS involvement at relapse (28%; 95% CI, 11–47; n = 43; p = 0.0031).
Safety
Adverse events experienced during the study are summarized in Table 3. The majority of Grade 3–4 adverse events (AEs) were hematological, with infections being the most common non-hematological AE experienced at ≥ Grade 3 (19%). Serious AEs were reported for 42 (52%) patients. The most frequent serious AEs were febrile neutropenia (n = 39) and infections (n = 25), followed by bleeding (n = 4), bowel perforation (n = 2), acute renal failure (n = 2), and acute neurotoxicity (n = 2). Fatal AEs occurred in four (5%) patients; all were due to sepsis and arose during MATRix treatment courses.
Table 3. Adverse events (adapted from Ferreri et al.1)
|
AE, adverse event; NT, neurotoxicity. |
||||
|
AE, n (%) |
Grades 1–2 |
Grade 3 |
Grade 4 |
Grade 5 |
|---|---|---|---|---|
|
Hematological |
|
|
|
|
|
Non-hematological |
|
|
|
|
Treatment interruptions due to toxicity occurred only during MATRix treatment; these were transient in five patients and permanent in four. Dose reductions were indicated in 24 (32%) patients across 32 courses of MATRix.
Conclusion
In patients with DLBCL with secondary CNS involvement, who often have a very poor prognosis, the sequential combination of MATRix and RICE followed by ASCT showed promising 1-and 2-year survival rates, and the authors proposed that the intensified chemotherapy regimen can produce durable responses in these patients. Furthermore, patients who progressed to ASCT following MATRix-RICE therapy displayed encouraging survival rates. Notably, chemotherapy-naïve patients with CNS involvement at initial lymphoma diagnosis achieved better survival rates than those with CNS dissemination upon relapse, suggesting that MATRix-RICE therapy may be particularly beneficial in this subset of patients. The safety profile of the combination treatment was adequate, with no major safety concerns raised during the study. Thus, the authors concluded that these results indicate a new and much-needed therapy option for patients with secondary CNS lymphoma.
The study was limited by the rarity of secondary CNS lymphoma, hence randomized trials to support single-arm studies are impractical. In addition, patient heterogeneity may have led to an interpretation bias. Patients older than 70 years were also excluded from the study, therefore the use of MATRix-RICE therapy in these older patients should not currently be considered. Moreover, there was no centralized review of imaging, with response assessments performed by local investigators, again generating a potential interpretation bias.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?