All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
Predicting response to BCR and BCL-2 therapies using MRD assessment in patients with CLL
Undetectable measurable residual disease (uMRD) has been demonstrated as an independent prognostic marker for longer progression-free survival (PFS) and overall survival (OS) in patients diagnosed with chronic lymphocytic leukemia (CLL). While new agents for CLL treatment, including BCL-2 and BCR inhibitors, have provided marked improvements in patient survival, uMRD status and the associated long-term outcomes are notably less conclusive when compared with data on standard chemotherapy.1
In response to this, Wierda et al.1 published a systematic literature review in Leukemia & Lymphoma investigating the relationship between MRD response and clinical outcomes in relation to BCL-2 and BCR inhibitor therapies. We summarize their findings below.
Study design
Data search, screening, extraction, and summary were conducted as outlined in Figure 1. All publications reporting data on MRD and treatment outcomes using quantitative and/or qualitative assessments between January 2010 and December 2021 were included in the initial search.
Figure 1. Data search, screening, extraction, and summary methods*
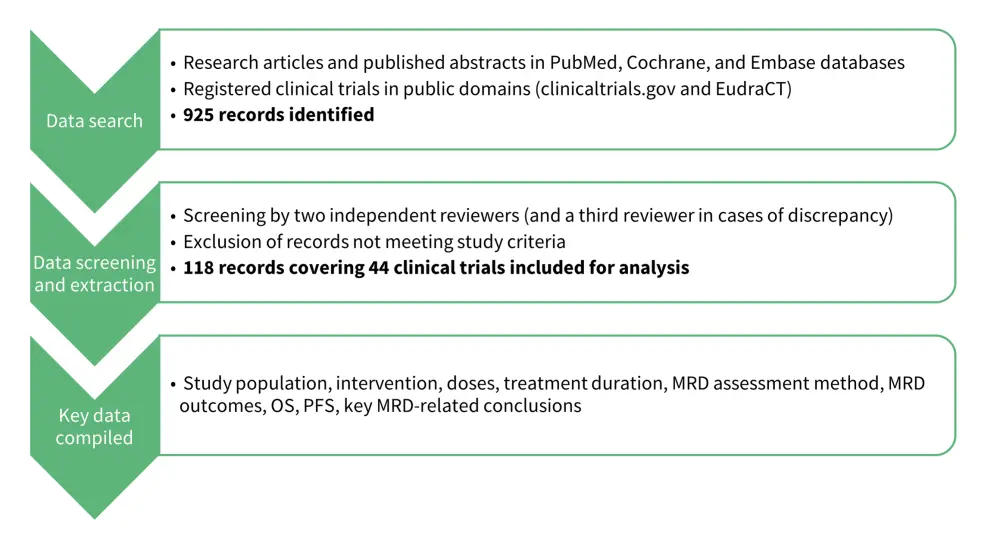
MRD, measurable residual disease; OS, overall survival; PFS, progression-free survival.
*Adapted from Wierda, et al.1
BCR therapy
The relationship between uMRD rate, progression-free survival (PFS), and overall survival (OS) outcomes with BCR therapy in CLL is currently inconclusive. Key findings from several trials investigating this relationship are shown in Figure 2.
Figure 2. Key findings from clinical trials investigating BCR therapy*
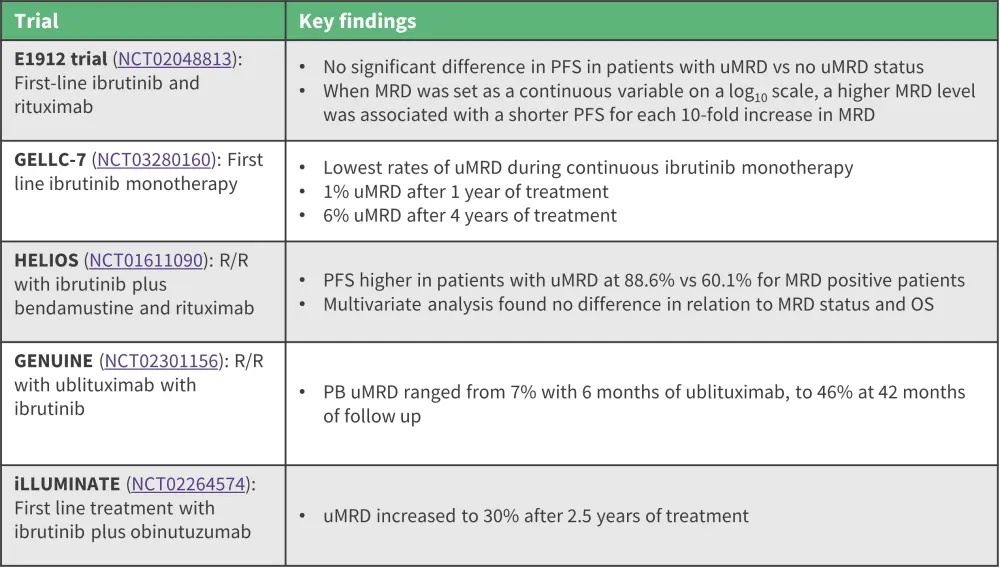
MRD, measurable residual disease; OS, overall survival; PB, peripheral blood; PFS, progression-free survival; uMRD, undetectable measurable residual disease.
*Adapted from Wierda, et al.1
BCL-2 therapy
Similarly, the relationship between BCL-2 therapies, uMRD, and patient outcomes is inconclusive. Figure 3 highlights several clinical trials involving BCL-2 treatment and their key findings in relation to the rates of uMRD, PFS, and OS.
Figure 3. Key findings from clinical trials investigating BCL-2 therapy*
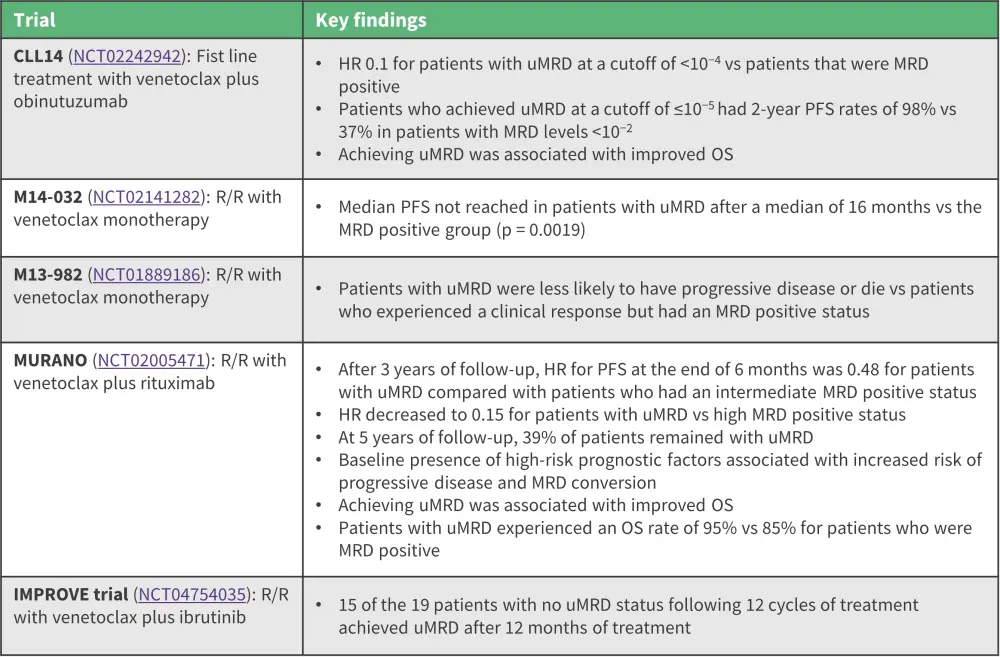
HR, hazard ratio; OS, overall survival; PFS, progression free survival; uMRD, undetectable measurable residual disease.
*Adapted from Wierda, et al.1
Combination therapy
The effect of BCR and BCL-2 therapy in combination on uMRD also remains unclear. Key findings of the effects of combination therapy on rates of uMRD, OS, and PFS are shown in Figure 4.
Figure 4. Key findings from clinical trials investigating combination therapy*
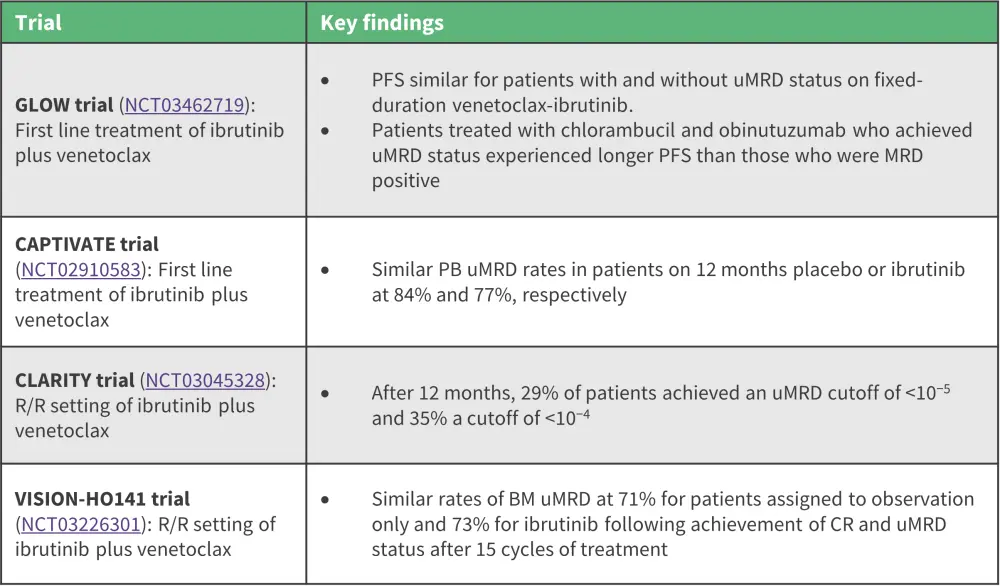
BM, bone marrow; CR, complete response; PFS, progression-free survival; MRD, measurable residual disease; PB, peripheral blood; uMRD, undetectable residual disease.
*Adapted from Wierda, et al.1
uMRD as a prognostic factor
- In the E1912 trial (NCT02048813), MRD-positive status in the absence of complete response (CR) after 12 months of treatment showed significantly lower PFS when compared with CR together with uMRD status.
- Undetectable MRD status was associated with similar PFS independent of CR status.
- In the CLL14 trial (NCT02242942), patients with uMRD experienced improved PFS compared with patients who were MRD positive, independent of clinical response.
- In the MURANO trial (NCT02005471), relapsed/refractory patients who achieved uMRD also experienced an improvement in PFS after continuous treatment at the 3-year follow-up.
- Patients treated with venetoclax-rituximab combination therapy who achieved a partial clinical response showed similar PFS rates to those achieving a CR and uMRD.
- Patients who showed a partial response and had detectable MRD had inferior PFS compared with patients with a partial response and uMRD.
- At the 4-year follow-up, MRD status was found to have no effect on PFS in patients with CR but incomplete hematologic recovery.
Conclusion
Measurable residual disease remains an important prognostic tool for patients diagnosed with CLL. Patients treated with BCL-2 inhibitors experienced both favorable and prolonged responses together with high rates of uMRD. Achievement of uMRD is regularly associated with sustained PFS and OS, independent of clinical response status. In comparison, BCR therapies had low rates of uMRD achievement, although uMRD remained associated with improved PFS.
However, due to the nature of this analysis, publication and immortal-time bias could not be ruled out despite the screening of published data by two independent reviewers. Future trials should aim to investigate MRD-guided treatments with the addition of longer follow-up periods to further evaluate the impact of MRD assessment on OS.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?
