All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
RE-MIND: A study comparing tafasitamab + lenalidomide versus a real-world lenalidomide monotherapy cohort of patients with R/R DLBCL
Lenalidomide (LEN), an immunomodulatory agent, has shown moderate efficacy in patients with relapsed/refractory (R/R) diffuse large B-cell lymphoma (DLBCL). Lenalidomide stimulates the proliferation and activation of natural killer cells in DLBCL and acts as a direct cytotoxic agent. Lenalidomide—while not approved in the US or the EU—can be used with or without rituximab, especially in the autologous stem-cell transplantation (ASCT)-ineligible setting. The single-arm phase II L-MIND study (NCT02399085), which investigated 12 cycles of lenalidomide plus tafasitamab (a CD-19 targeting monoclonal antibody) followed by tafasitamab monotherapy in adult patients with R/R DLBCL who were ineligible for ASCT, led to the recent approval of lenalidomide plus tafasitamab in this patient population. To better understand how tafasitamab contributed to the efficacy of this combination, Zinzani et al.1 generated a historical control for L-MIND using real-world data from patients treated with lenalidomide monotherapy (NCT04150328). The Lymphoma Hub is pleased to provide a summary of the key findings.
Study design
This was a retrospective, multicenter, observational study to generate a historical control for L-MIND. Study sites (US and EU) were chosen according to the geographic distribution of the subjects in L-MIND. Eligibility criteria were also aligned with L-MIND and included patients who were:
- ≥18 years with histologically confirmed DLBCL
- R/R after 1−3 prior systemic therapies, including ≥1 CD20-targeting regimen
- not candidates for high-dose chemotherapy (HDC) and subsequent ASCT
Patients were excluded if they had:
- central nervous system involvement
- received lenalidomide in combination with any other anti-lymphoma therapy
- prior treatment with lenalidomide, thalidomide, or ASCT
- known double- or triple-hit lymphoma
- a history of prior malignancy within the last 5 years
The baseline patient and disease characteristics were balanced between the tafasitamab + lenalidomide and lenalidomide monotherapy cohorts using estimated propensity score (ePS) matching for nine pre-specified covariates of prognostic importance. These included age, Ann Arbor stage, refractoriness to last therapy line, number of prior lines of therapy, history of primary refractoriness, prior ASCT, elevated lactate dehydrogenase (LDH), neutropenia, and anemia. Each patient in the combination (tafasitamab + lenalidomide) cohort was propensity score-matched with a single patient in the lenalidomide monotherapy cohort.
- The primary endpoint was investigator-assessed best overall response rate (ORR)—complete response (CR) or partial response (PR) as best response.
- Secondary endpoints included:
- CR rate
- disease control rate (DCR), defined as CR + PR + stable disease (SD)
- duration of response (DoR)
- overall survival (OS)
- progression-free survival (PFS)
- event-free survival (EFS)
- time-to-next-treatment (TTNT)
Results
Baseline characteristics
Following ePS matching, the primary analysis set (matched analysis set 25, or MAS25) comprised 76 patients in each cohort. The baseline characteristics for MAS25 were well balanced, with standardized mean differences (SMD) ≤0.13 for seven of the nine baseline characteristics (Table 1). The median lenalidomide dose intensity was 17.6 mg/day (interquartile range [IQR] 14.4−19.2).
Table 1. Balancing baseline characteristics for MAS25*
|
ASCT, autologous stem cell transplantation; LEN, lenalidomide; LDH, lactate dehydrogenase; mon, monotherapy; ULN, upper limit of normal. |
||
|
Balancing characteristic, % (unless otherwise stated) |
Tafasitamab + LEN |
LEN-mon |
|---|---|---|
|
Age |
|
|
|
<70 years |
43 |
41 |
|
≥70 years |
57 |
59 |
|
Ann Arbor stage |
|
|
|
I/II |
25 |
16 |
|
III/IV |
75 |
84 |
|
Refractoriness to last prior therapy |
45 |
45 |
|
Number of prior systemic treatment lines |
|
|
|
1 |
51 |
37 |
|
2−3 |
49 |
63 |
|
Primary refractoriness |
18 |
21 |
|
Prior ASCT |
12 |
8 |
|
Elevated LDH (>ULN) |
54 |
59 |
|
Neutropenia (cutoff <1.5 × 109/L) |
3 |
3 |
|
Anemia (cutoff <10 g/dL × 109/L) |
8 |
7 |
Efficacy
- Patients in the tafasitamab + lenalidomide cohort showed a significantly better ORR of 67.1% (95% CI, 55.4−77.5) versus 34.2% (95% CI, 23.7−46.0) in the lenalidomide monotherapy cohort (p < 0.0001) (Figure 1).
- CR rate was also significantly higher in the tafasitamab + lenalidomide cohort compared with lenalidomide monotherapy cohort (39.5%; 95% CI, 28.4−51.4 vs 13.2%; 95% CI, 6.5−22.9).
The median DoR was 20.5 vs 6.6 months in the tafasitamab + lenalidomide and lenalidomide monotherapy cohorts, respectively.
Figure 1. Best response rate*
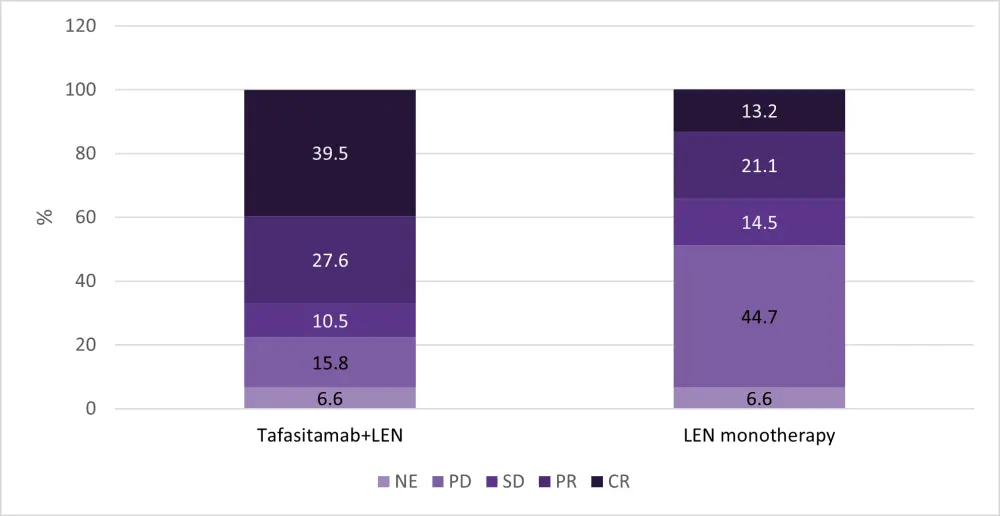
CR, complete response; LEN, lenalidomide; NE, not evaluable; PD, progressive disease; PR, partial response; SD, stable disease.
*Adapted from Zinzani et al.1
- OS was superior in the tafasitamab + lenalidomide cohort vs lenalidomide monotherapy cohort (median OS not estimable vs 9.4 months; p = 0.0026) at a median follow-up of 21.5 vs 20.9 months, respectively.
- Similarly, EFS was superior in the tafasitamab + lenalidomide compared to lenalidomide monotherapy cohort (median 12.1 months vs 4.0 months; p < 0.0001), at a median follow-up of 21.9 vs 15.4 months, respectively.
- PFS was also prolonged in the tafasitamab + lenalidomide compared to the lenalidomide monotherapy cohort (median 12.1 months vs 4 months; p = 0.0002), at a median follow-up of 19.7 vs 12.6 months, respectively.
- Median TTNT was likewise prolonged at 16.7 months in the tafasitamab + lenalidomide cohort compared with 5.1 months in the lenalidomide monotherapy cohort.
- ORR was consistently higher in the tafasitamab + lenalidomide cohort compared to the lenalidomide monotherapy cohort in the subgroup analyses, irrespective of age, disease stage, treatment history, and refractoriness (Table 2).
Table 2. Best ORR by subgroups MAS25*
|
ASCT, autologous stem cell transplantation; CI, confidence interval; LEN, lenalidomide; mon, monotherapy; ORR, overall response rate. |
||||
|
Characteristic |
Tafasitamab + LEN (n) |
ORR |
LEN-mon |
ORR |
|---|---|---|---|---|
|
Age |
||||
|
<70 years |
33 |
60.6 (42.1−77.1) |
31 |
38.7 (21.9−57.8) |
|
≥70 years |
43 |
72.1 (56.3−84.7) |
45 |
31.1 (18.2−46.7) |
|
Ann Arbor Stage |
||||
|
I/II |
19 |
63.2 (38.4−83.7) |
12 |
33.3 (9.9−65.1) |
|
III/IV |
57 |
68.4 (54.8−80.1) |
64 |
34.4 (23.0−47.3) |
|
Refractoriness to last therapy line |
34 |
64.7 (46.5−80.3) |
34 |
23.5 (10.8−41.2) |
|
Number of prior lines of therapy |
||||
|
1 |
39 |
74.4 (57.9−87.0) |
28 |
35.7 (18.6−55.9) |
|
2/3 |
37 |
59.5 (42.1−75.3) |
48 |
33.3 (20.4−48.4) |
|
History of primary refractoriness |
14 |
64.3 (35.1−87.2) |
15 |
37.5 (15.2−64.5) |
|
Prior ASCT |
9 |
77.8 (40.0−97.2) |
6 |
50.0 (11.8−88.2) |
Safety
- Safety data was not collected except to document the reason for change in lenalidomide treatment.
- All patients in the tafasitamab + lenalidomide cohort and 96% of patients in the lenalidomide monotherapy cohort discontinued lenalidomide permanently.
- Lenalidomide discontinuation occurred due to progressive disease (40 vs 63%), planned discontinuation (32% vs 9%), and adverse events (15% vs 9%) in the tafasitamab + lenalidomide cohort and lenalidomide monotherapy cohort, respectively.
- Overall, relapse, progression or death was experienced by 59% vs 83% of patients in the tafasitamab + lenalidomide and lenalidomide monotherapy cohorts, respectively.
Conclusion
While the long-term follow-up analysis of the L-MIND trial showed durable responses and a median OS of 31.6 months in patients with R/R DLBCL treated with tafasitamab + lenalidomide, the single-arm design of the trial did not allow for analysis of the clinical benefit provided by tafasitamab. This retrospective, observational study allowed the estimation of the additional treatment benefit attained by combining tafasitamab + lenalidomide compared with lenalidomide monotherapy in patients with R/R DLBCL who were not eligible for transplant, had historically poor prognosis, and were a difficult-to-treat population.
It is important to note that the authors of this study compared data from one patient population (patients treated with tafasitamab + lenalidomide in the L-MIND trial) with data from an entirely separate patient population (historical controls treated with lenalidomide monotherapy), and thus, measures were undertaken to reduce the bias inherent in this type of comparison. RE-MIND included several measures to reduce bias, including selecting patients from similar geographic regions, allowing only patients who started lenalidomide at 25 mg/day, and using ePS matching in a large pool of patients to allow for selection of the most closely matched population. While propensity score matching is not a replacement for randomized, controlled trials, this method has provided a valuable comparator cohort that demonstrates the clinical benefit of adding tafasitamab to lenalidomide in patients with R/R BLBCL who are ineligible for ASCT.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?