All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Symposium | Optimizing outcomes before and after CAR T-cell therapy in patients with large B-cell lymphoma
Featured:
 Ulrich Jäger
Ulrich JägerDo you know... According to the 2021 best practice recommendations of the EBMT, JACIE, and EHA for the management of cytokine release syndrome (CRS), what is the first management step once Grade 2 CRS is confirmed?
During the European Hematology Association (EHA) 2024 Hybrid Congress, the Lymphoma Hub and Multiple Myeloma Hub held a joint satellite symposium entitled: Sequencing immune-based therapies in B-cell malignancies. Here, the Lymphoma Hub is pleased to share a real-world patient case, real-world evidence and experience, and treatment optimization of chimeric antigen receptor (CAR) T-cell therapy in patients with large B-cell lymphoma (LBCL), presented by Ulrich Jäger, Medical University of Vienna, Vienna, AT.
Symposium | Optimizing outcomes before and after CAR T-cell therapy in patients with large B-cell lymphoma
Listen to the podcast here:
Symposium | Optimizing outcomes before and after CAR T-cell therapy in patients with large B-cell lymphoma
In this presentation, Jäger started by sharing a case study from 2009 of a 50-year-old male with complicating treatment for an underlying myeloproliferative disease (essential thrombocythemia) who later developed diffused LBCL in 2020 and was treated with axicabtagene ciloleucel (axi-cel) in second-line in 2021.1,2 The patient is still in complete response from lymphoma after 3 years and does not need treatment for his myeloproliferative disorder. Platelet counts are still within the normal range.
Jäger then discussed real-world experiences of CAR T-cell therapy in lymphoma using EBMT registry data (Figure 1) and clinical trials (Table 1), before exploring key considerations when optimizing CAR T-cell therapy outcomes (Figure 2).
Figure 1. CAR T-cell therapy in the EBMT registry: A) underlying diagnosis and B) academic vs commercial products*
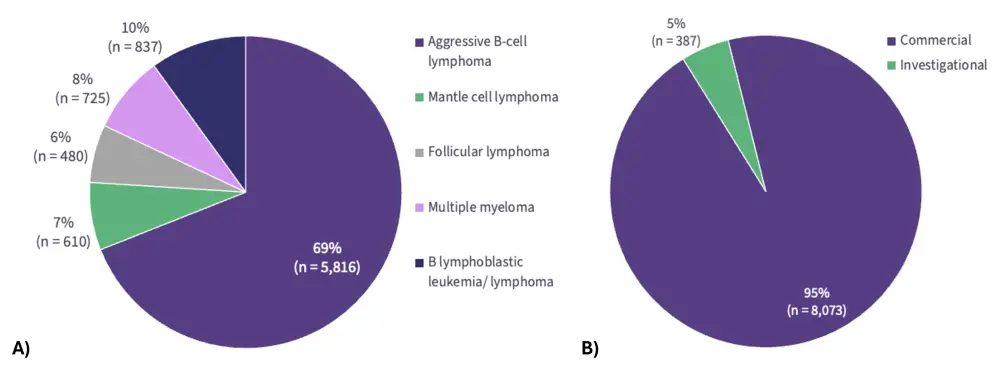
CAR, chimeric antigen receptor; EBMT, European Society for Blood and Marrow Transplantation.
*Data provided by Sureda A.
Table 1. Efficacy outcomes of CAR T-cells in R/R LBCL*
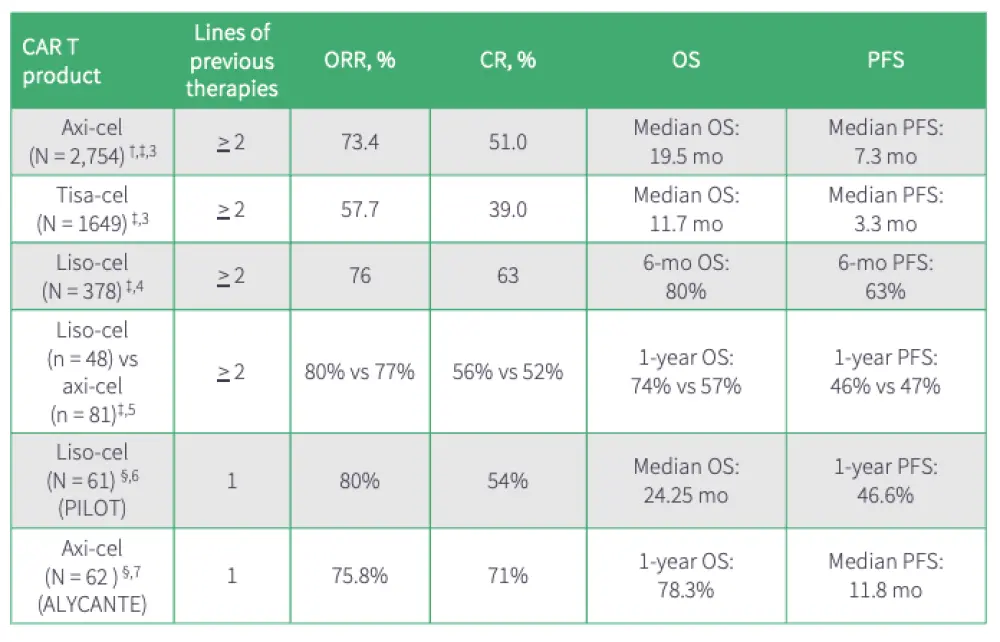
Axi-cel, axicabtagene ciloleucel; CAR, chimeric antigen receptor; CR, complete response; HSCT, Hematopoietic stem cell transplantation; LBCL, large B-cell lymphoma; liso-cel, lisocabtagene maraleucel; mo, month; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; R/R, relapsed/refractory; tisa-cel, tisagenlecleucel.
* Data from Jacobson CA, et al.3 Crombie JL4. Portuguese A5, Sehgal A6, Houot, R, et al.7
†Included patients who would have been ineligible for the clinical trial; ‡ real-world studies; §trials from patients who are ineligible for HSCT.
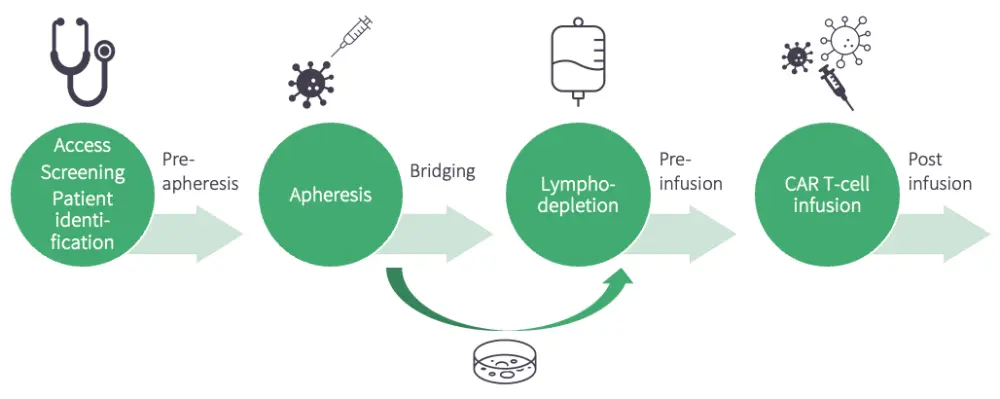
Figure 2. CAR T-cell therapy optimization
Watch the presentation to learn more about:
- The safety and efficacy of lisocabtagene maraleucel (liso-cel) and axi-cel in the real world.
- Factors affecting the response to CAR T-cell therapy, such as incidence of cytopenias, inflammatory markers, and differentiated CD3+CD27‑CD28‑ T cells.
- Key considerations to optimize CAR T-cell therapy outcomes.
Key points
- A considerable proportion of patients with relapsed/refractory (R/R) LBCL treated in real-world settings are ineligible for clinical studies.3-7
- The 2021 best practice recommendations by the EBMT, JACEI, and EHA for the management of adults and children receiving CAR T-cell therapy suggest early intervention and management strategies of cytokine release syndrome (CRS)8:
- Grade 1 CRS: in the absence of improvement within 3 days and the absence of other differential diagnoses, consider tocilizumab
- Grade 2–4 CRS: alert local intensive care unit
- Real-world experiences of axi-cel and liso-cel in second-line R/R LBCL showed that liso-cel had5:
- Lower rates of any-grade CRS (88% vs 62%; p < 0.001)
- Lower rates of any-grade ICANS (56% vs 32%; p = 0.010)
- Fewer days with fever (median, 5 vs 2 days; p < 0.001)
- Fewer Grade 3 CRS (2.1% [no Grade 4/5 events] vs 7.4% [2.5% Grade 4 events])
- Numerically lower severe cytopenias (93% vs 72%; p = 0.002)
- Barriers listed by patients in preparation for CAR T-cell therapy include access to clinical trials/registries, access to emergency treatment room, waiting time, communication between local hospital and CAR T team, and their mental and physical health.
- Real-world outcomes can be optimized at various steps of CAR T-cell therapy treatment; for example:
- Precise patient selection criteria play a key role in improving outcomes.
- Effective bridging ensures low tumor burden at infusion, and lymphodepletion is also associated with improved tumor microenvironment, contributing to better prediction and management of toxicity.
- Incidence of cytopenias, inflammatory markers, and differentiated CD3+CD27‑CD28‑ T cells affects the response to CAR T-cell therapy.
- After CAR T-cell therapy administration, management should include prediction and treatment of hematotoxicity and non-relapse mortalities.
- Bispecific antibodies showed promising outcomes, with an overall response rate of up to 63%, with CR rates of 39% in the treatment of patients who relapse after CAR T-cell therapies.9
This independent educational activity was supported by Bristol Myers Squibb. All content was developed independently by the faculty. The funder was allowed no influence on the content of this activity.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?