All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
The CAR-HEMATOTOX model for CAR T-cell hematotoxicity in R/R LBCL
Hematotocixity is a frequent adverse event related to chimeric antigen receptor (CAR) T-cell therapy. Despite an improvement in response rates in relapsed/refractory (R/R) B-cell malignancies, the utility of CAR T-cell therapy has been affected by its distinct toxicity profile.1 CAR T-cell-mediated hematotoxicity is a manifestation of cytokine release syndrome and a component of CAR T-cell-associated toxicity, which can predispose patients to infectious complications.2 There is a high incidence of Grade ≥3 neutropenia (30–38%), thrombocytopenia (21–26%), and anemia (5–17%) which persists after Day 21, highlighting the importance of hematotoxicity in the first year after CAR T-cell therapy. The underlying mechanism is poorly understood.1,2
Rejeski, et al. recently reported the results from their study in which they devised and validated a risk stratification tool (CAR-HEMATOTOX) to identify patients who are at risk of hematotoxicity. Rejeski presented the study data at the 16th International Conference on Malignant Lymphoma (16-ICML)2 and has also recently published the work in Blood.1
Study design and patient characteristics1,2
A multicenter retrospective analysis of 258 patients (intent-to-treat population) to assess patterns of hematopoietic reconstitution and to identify predictive markers. Patients were receiving either axicabtagene ciloleucel (n = 170) or tisagenlecleucel (n = 88) immunotherapy for R/R large B-cell lymphoma and were split into training and validation cohorts (see Figure 1).
Figure 1. Number of patients included in the training and validation cohorts*
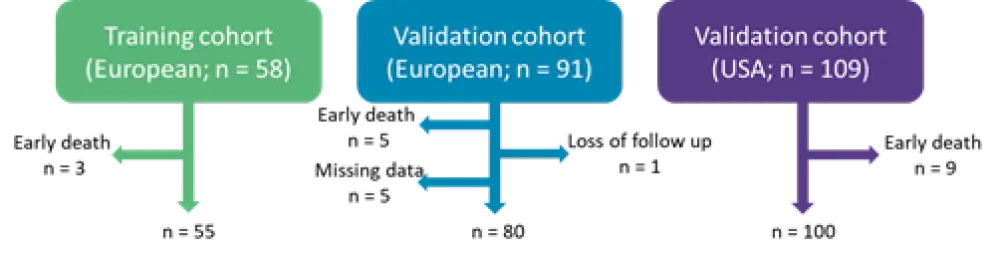
*Adapted from Rejeski, et al.1
The primary endpoint was clinically significant neutropenia (absolute neutrophil count [ANC] ≤500/µL) between Days 0 and 60.
At the time of lymphodepletion, there were differences between the US and European cohorts; the European cohort had a higher tumor burden, more inflammation, and decreased ANC (see Table 1).
Table 1. Patient characteristics at baseline*
|
ANC, absolute neutrophil count; CI, confidence interval; CRP, C-reactive protein; LDH, lactate dehydrogenase. |
||||
|
Characteristic |
All patients |
Training cohort |
European validation cohort |
USA validation cohort |
|---|---|---|---|---|
|
Age (range), years |
63 (19–83) |
59.5 (19–74) |
62 (27–83) |
64 (19–79) |
|
Complete blood count |
||||
|
Median ANC (95% CI), ANC/µL |
2,540 (2,310–2,730) |
2,005 (1,620–2,640) |
2,320 (1,840–2,660) |
3,050 (2,540–3,530) |
|
Median platelet count (95% CI), 109/L |
164 (152–178) |
152.5 (118–180) |
171 (146–200) |
164 (152–178) |
|
Median hemoglobin (95% CI), g/dL |
10.1 (9.7–10.4) |
10.1 (9.5–10.3) |
10.0 (9.3–10.6) |
10.3 (9.6–11.0) |
|
Markers of tumor burden and inflammation |
||||
|
Median LDH (95% CI), U/L |
276 (260–302) |
271 (245–381) |
302 (273–328) |
258 (232–297) |
|
Median CRP (95% CI), mg/dL) |
1.02 (0.80–1.40) |
1.55 (0.80–2.62) |
1.02 (0.76–1.50) |
0.81 (0.48–1.29) |
|
Median ferritin (95% CI), ng/mL |
501 (378–647) |
821 (576–1203) |
454 (310–647) |
378 (289–573) |
Patients across all three cohorts had a high incidence of hematotoxicity; 62% had severe thrombocytopenia, 69% had anemia, 91% had severe neutropenia, and 64% had prolonged neutropenia (≥21 days after CAR transfusion). The median duration of severe neutropenia was 9 days (95% confidence interval [CI]; 8–10 days).
Clinical phenotypes of neutrophil recovery1,2
The team found that neutropenia generally follows a bimodal curve, with recovery after G-CSF stimulation, followed by a second ‘dip’ in ANC.
Different patterns of recovery were observed, and patients in the training and European validation cohort could be divided into the following three groups:
- Quick recovery: sustained neutrophil recovery without a second dip in ANC <1,000/µL (n = 37)
- Intermittent recovery: neutrophil recovery with ANC above 1500 per µL, with a second dip of ANC to <1,000/µL (n = 78)
- Aplastic: continuous severe neutropenia with ANC <500/µL for ≥14 days (n = 34)
The pattern of thrombocytopenic depletion and recovery was quite different, with the lowest platelet count occurring between Days 21 and 60 following lymphodepletion. Platelet recovery is achieved by most patients around Day 90. This pattern suggests a different mechanism behind thrombocytopenia.
Biomarkers of prolonged neutropenia1
Univariate analysis of pre-lymphodepletion biomarkers identified markers associated with a low hematopoietic reserve (low baseline platelet count, hemoglobin, or ANC) or increased inflammation (elevated C-reactive protein) were significantly associated with prolonged duration of neutropenia.
CAR-HEMATOTOX1
A discriminatory multivariate model that could detect the binary outcome of severe neutropenia for <14 days or ≥14 days was developed using markers identified with an area under the curve (AUC) >0.6, a p value ≤0.1, and an odds ratio ≥2.5. Multivariate analysis of markers included in the model identified platelet count and ferritin as of particular importance, so they were weighted accordingly.
The CAR-HEMATOTOX model gives a score based on patient baseline features as described in Table 2. A final score of 0–1 is classed as low for severe neutropenia lasting ≥14 days, and a score ≥2 would be classed as high. In the training cohort, CAR-HEMATOTOX could discriminate for severe neutropenia lasting ≥14 days (AUC, 0.82; p < 0.001; sensitivity, 0.96; specificity, 0.67).
Table 2. CAR-HEMATOTOX model scoring based on baseline features*
|
ANC, absolute neutrophil count; CRP, C-reactive protein. |
|||
|
Baseline features |
0 point |
1 point |
2 points |
|---|---|---|---|
|
Platelet count, per µL |
>175,000 |
75,000–175,000 |
<75,000 |
|
ANC, per µL |
>1,200 |
<1,200 |
— |
|
Hemoglobin, g/dL |
>9.0 |
<9.0 |
— |
|
CRP, mg/dL |
<3.0 |
>3.0 |
— |
|
Ferritin, ng/mL |
<650 |
650–2,000 |
>2,000 |
CAR-HEMATOTOX was then tested in the two validation cohorts (European and USA), which were pooled together (n = 180). Using CAR-HEMATOTOX to divide patients into low- and high-score categories, 81% of the high-score group suffered with prolonged neutropenia (≥21 days after CAR transfusion), but only 42% of the low-score group had prolonged neutropenia (Table 3).
The primary endpoint of clinically significant neutropenia (ANC ≤500/µL) between Days 0 and 60 was seen for a total of 5.5 days (95% CI, 5–8) in the low-score group and 12 days (95% CI, 10–16) in the high-score group (Table 3), demonstrating the high negative predictive value of the score.
Table 3. Patients in CAR-HEMATOTOX high-/low-risk categories and relationship with outcomes*
|
CI, confidence interval. |
||||||
|
Outcome, % (unless otherwise stated) |
Training cohort (n = 55) |
Pooled validation cohort (n = 180) |
||||
|---|---|---|---|---|---|---|
|
High |
Low |
p value |
High |
Low |
p value |
|
|
Severe thrombocytopenia |
88 |
52 |
0.006 |
87 |
34 |
<0.001 |
|
Anemia |
91 |
61 |
0.02 |
96 |
40 |
<0.001 |
|
Neutropenia |
||||||
|
Severe |
100 |
96 |
0.4 |
99 |
79 |
<0.001 |
|
Profound |
100 |
65 |
<0.001 |
89 |
49 |
<0.001 |
|
Protracted, severe |
97 |
48 |
<0.001 |
88 |
46 |
<0.001 |
|
Protracted, profound |
50 |
0 |
<0.001 |
47 |
5 |
<0.001 |
|
Prolonged |
91 |
61 |
0.02 |
81 |
42 |
<0.001 |
|
Primary endpoint |
||||||
|
Duration of severe neutropenia (95% CI), days |
16.5 |
7.0 |
<0.001 |
12.0 |
5.5 |
<0.001 |
|
Binary endpoint |
||||||
|
Severe neutropenia ≥14 days |
66 |
4 |
<0.001 |
48 |
5 |
<0.001 |
Linear regression analysis of the two validation cohorts confirmed the discriminatory capacity of the CAR-HEMATOTOX score (USA cohort: AUC, 0.91; p < 0.001; European cohort: AUC, 0.77; p < 0.001). In terms of the clinical phenotypes of neutrophil recovery, most aplastic phenotypes fell within the high score group, whereas most of the quick recovery phenotypes were within the low score group. The study group also found that CAR-HEMATOTOX score was indicative of hospital stay, with those in the high score group having a longer hospitalization.
Conclusion
The authors concluded that real-world experience demonstrated the high incidence of delayed cytopenias following CAR T-cell therapy. They found that patients have different patterns of neutrophil recovery and can be separated into three groups (quick, intermittent, and aplastic).2 The CAR-HEMATOTOX model was reported to be easy to apply and demonstrates the importance of pre-CAR T-cell therapy bone marrow reserve and inflammation as key features affecting cytopenia.1,2 The study had limitations, in that it was retrospective, and had incomplete data around bone marrow infiltration and presence of dysplastic changes or clonal hematopoiesis. In addition, the team chose a lower cut-off score for the CAR-HEMATOTOX model, which yielded a highly sensitive tool with good negative predictive value; however, in the clinical setting, a higher cut-off may be necessary to improve specificity and positive predictive value.1 The group concluded that CAR-HEMATOTOX could be used for risk-stratification prior to treatment and could help guide prophylactic treatment and outpatient management.1,2
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?