All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Treatment with ublituximab plus ibrutinib versus ibrutinib alone: A phase III randomised trial (GENUINE) for patients with relapsed or refractory high-risk CLL
The addition of anti-CD20 monoclonal antibody therapy to the Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib, is being investigated to improve outcomes for patients with high-risk chronic lymphocytic leukemia (CLL); however, the optimal ibrutinib/anti-CD20 monoclonal antibody combination is currently unknown.
Ublituximab is a second-generation, glycoengineered anti-CD20 monoclonal antibody (mAb) that binds to a unique epitope on CD20, resulting in improved FcγRIIIA binding and superior antibody-dependent cellular cytotoxicity, compared with the first-generation anti-CD20 mAb rituximab.1 The safety and efficacy of ibrutinib combined with ublituximab for the treatment of relapsed/refractory (R/R) high-risk patients with CLL has been investigated in the phase III GENUINE trial (NCT02301156). Initial results from the trial were previously reported by the Lymphoma Hub. Here, we provide a summary of the final analysis, published by Jeff Sharman and colleagues in The Lancet Haematology.2
Study design
The study consisted of two arms; a combination therapy cohort of patients treated with ublituximab and ibrutinib, and a monotherapy cohort of patients treated with ibrutinib alone.
Inclusion criteria
Patient selection was based on the following criteria:
- Aged 18 years or older.
- Eastern Cooperative Oncology Group (ECOG) performance status of 2 or lower.
- Received at least two cycles of at least one standard treatment regimen.
- Presence of high-risk cytogenetics with at least one of the following: del(17p), del(11q), or TP53 mutation.
- Measurable lymphadenopathy.
- Adequate organ function.
The trial design is summarized in Figure 1.
Figure 1. Trial design*
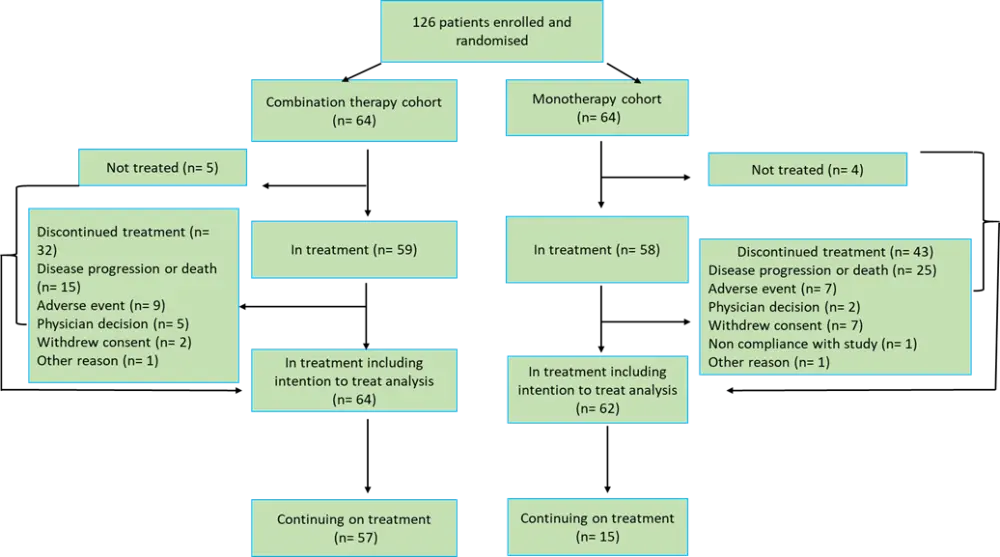
*Adapted from Sharman et al.2
The ublituximab administration routine is briefly described in Table 1. Oral ibrutinib was administered daily at a dose of 420 mg until disease progression, unacceptable toxicity, or withdrawal of consent. A reduction in ibrutinib dose was permitted in the case of Grade 3 or worse nonhematologic events, Grade 3 or worse neutropenia with infection or fever, or Grade 4 hematologic toxicities.
The median ibrutinib treatment duration was 31.5 months (IQR, 12.4–39.5) in the ublituximab plus ibrutinib group, and 17.0 months (IQR, 5.2–35.3) in the ibrutinib group. The median ublituximab treatment duration in the ublituximab plus ibrutinib group was 30.3 months (10.3–38.1).
Table 1. A summary of ublituximab administration routine*.
|
h, hour; mins, minutes. |
||
|
Cycles (28 days each) |
Administration days |
Ublituximab dose (intravenous) |
|---|---|---|
|
1 |
1 |
≤150 mg, over 4 h |
|
2 |
750 mg, over 4 h |
|
|
8 |
900 mg, over 3 h |
|
|
15 |
900 mg, over 3 h |
|
|
2 – 6 |
1 |
900 mg, over 90 mins |
|
Maintenance, every 3 cycles |
— |
900 mg, over 90 mins |
Study end points
- The primary endpoint was independent review committee (IRC)-assessed overall response rate (ORR), encompassing patients who has achieved a partial response (PR), complete response (CR), or complete response with incomplete marrow recovery (CRi). Response assessments were carried out at the end of Cycles 2, 4, and 6, and then after every 3 cycles for the under-treatment cohort and every 3 months for patients in follow-up.
- Due to delayed accrual, the study was not powered for secondary endpoints, however, the following aspects were analysed: progression-free survival (PFS), minimal residual disease (MRD) negativity rate (less than 1 CLL cell per 10,000 leukocytes), CR rate, duration of response, time to response, and safety profile.
- Post-hoc analyses included: ORR including PR with lymphocytosis; PFS according to mutational status, MRD status, and response; and overall survival (OS) at 48 months.
Patient characteristics
Most of the patient characteristics were well balanced between study arms (Table 2). The presence of bulky disease (≥5 cm) at baseline was more common in the combination therapy cohort (48%) compared with the monotherapy cohort (28%), and the TP53 mutation and/or 17p deletion were more common in the monotherapy cohort (60%) compared with the combination therapy cohort (47%).
Table 2: Patient characteristics in both arms of the study*.
|
ECOG, Eastern Cooperative Oncology Group; IGHV, immunoglobulin heavy-chain variable region gene; TP53, tumor protein P53 gene. |
||
|
Characteristic |
Ublituximab plus ibrutinib |
Ibrutinib monotherapy |
|---|---|---|
|
Age, years (range) |
66 (62–74) |
67 (62–74) |
|
Sex, % |
||
|
Male |
69 |
74 |
|
ECOG performance status, % |
||
|
0–1 |
98 |
97 |
|
Rai stage III–IV, % |
51 |
44 |
|
Bulky disease (≥5 cm) at baseline, % |
48 |
28 |
|
Genetic abnormalities, % |
||
|
17p deletion |
44 |
48 |
|
IGHV unmutated†, % |
83 |
84 |
|
Time since diagnosis, years (range) |
7.1 (3.6–10.1) |
5.3 (3.3–8.2) |
|
Previous lines of therapy, n (range) |
1 (1–2) |
1 (1–2) |
Study outcomes
- In the intention-to-treat (ITT) population, ORR and ORR including PR with lymphocytosis were 83% and 86%, respectively, for the combination therapy cohort, and 65% and 73%, respectively, for the ibrutinib monotherapy cohort (Table 3).
Table 3. IRC-assessed ORR in the ITT and treated populations*.
|
CR, complete response; CRi, CR with incomplete marrow recovery; IRC, independent review committee; ITT, intention-to-treat; MRD, minimal residual disease; ORR, overall response rate; PR, partial response. |
||||||
|
Outcomes |
ITT group |
Treated group |
||||
|---|---|---|---|---|---|---|
|
Ublituximab plus ibrutinib |
Ibrutinib |
p value |
Ublituximab plus ibrutinib |
Ibrutinib |
p value |
|
|
ORR, % |
83 |
65 |
0.020 |
90 |
69 |
0.0060 |
|
CR |
17 |
3 |
0.016 |
19 |
3 |
0.020 |
|
CRi |
2 |
2 |
2 |
2 |
|
|
|
PR |
64 |
60 |
|
69 |
64 |
|
|
PR with lymphocytosis |
3 |
8 |
|
3 |
9 |
|
|
Stable disease |
3 |
13 |
|
3 |
14 |
|
|
ORR including PR with lymphocytosis, % |
86 |
73 |
0.066 |
93 |
78 |
|
|
MRD negativity, % |
42 |
6 |
< 0.0001 |
46 |
7 |
|
|
Peripheral blood |
41 |
6 |
44 |
7 |
|
|
|
Bone marrow |
2 |
0 |
2 |
0 |
|
|
- In the ITT population, rates of CR (with or without incomplete marrow recovery) were 19% for the combination therapy cohort and 5% for the monotherapy cohort (p = 0.016). In the treated population, the CR rates (with or without incomplete marrow recovery) were 20% and 5% (p = 0.024) in the combination therapy and monotherapy cohorts, respectively.
- MRD negativity was 42% in the combination therapy cohort and 6% in the monotherapy cohort (p < 0.0001).
- After a median follow-up of 41.6 months, median PFS was not reached for the combination therapy cohort and was 35.9 months for the monotherapy cohort (HR 0.46; 95% CI, 0.24−0.87; p = 0.016).
- Patients with del(17p) or TP53 mutation treated with ibrutinib monotherapy experienced worse PFS than patients without these genetic features. The same negative impact on PFS was not observed for patients with del(17p) or TP53 mutation in the combination therapy group.
- Patients with del(11q) had improved PFS compared with patients with del(17p) or TP53 mutation, and the addition of ublituximab to ibrutinib offered no survival benefit for these patients.
- An OS rate of 83% (95% CI; 65.9−91.5) was observed in the combination therapy group, and 69.2% (95% CI; 54.1−80.3) in the monotherapy group. The median OS was not reached for all patients (in combination and monotherapy cohorts) as well as for patients with del(17p), TP53 mutation, or both (in combination and monotherapy cohorts).
Safety
Grade ≥3 adverse events were experienced in 76% of patients receiving ublituximab plus ibrutinib and 83% of patients receiving ibrutinib monotherapy.
- Pneumonia was the most common serious adverse event, with 10% and 7% of cases in the combination and monotherapy groups, respectively. Incidence of atrial fibrillation was 7% vs 2%, sepsis was 7% vs 2%, and febrile neutropenia was 5% vs 2%.
- The most common adverse event possibly related to treatment was febrile neutropenia (5% patients in the combination therapy group and none in the monotherapy group). This was followed by pneumonia (3% in each group), atrial fibrillation (3% vs 2%), dysphagia (3% vs none), sepsis (3% vs none), and pleural effusion (none vs 3%).
Limitations
- Patient selection was carried out at small community centres with limited testing facilities. Therefore, it is possible that eligible patients could have been overlooked for study enrollment.
- The need for commercial acquisition of ibrutinib may have acted as a barrier for many eligible patients.
- As previous line of therapy was used to group patients instead of high-risk features, an uneven distribution of TP53 mutations among the two treatment groups may have impacted the study outcomes.
- A modification in study design to evaluate ORR-only instead of long-term outcomes resulted in a lack of data on the optimal duration, and long-term impact of maintenance therapy.
Conclusion
The results from this study further support the use of newer anti-CD20 antibodies with BTK inhibitors to treat patients with CLL. The major finding was the increased depth of response achieved by adding ublituximab to ibrutinib for the treatment of high-risk patients with CLL. The enhanced potency of the ibrutinib/ublituximab combination was also evident from the higher number of patients reaching MRD negativity, at more rapid rates, and improved PFS compared with ibrutinib therapy alone.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?