All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
AACR 2017 | Poster 2447/4 – The mutational landscape of chemo-refractory Burkitt Lymphoma
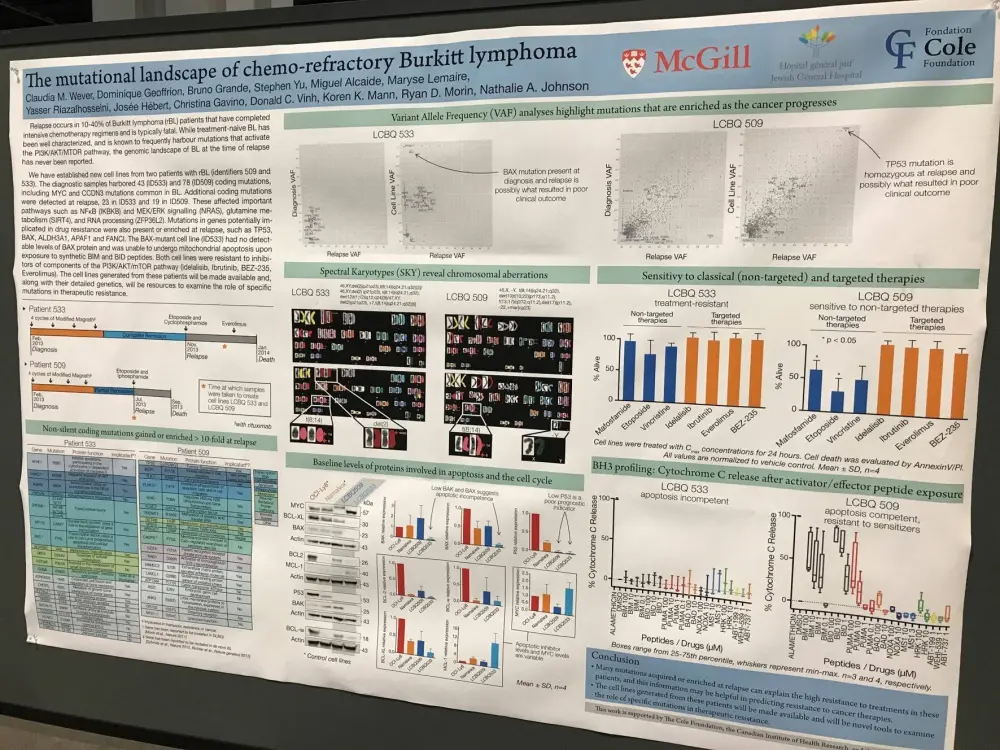
On Monday 3rd April during this year’s American Association for Cancer Research (AACR) annual meeting, a poster (2447 / 4) by Claudia M. Wever, from McGill University, Montreal, QC, Canada, et al. titled “The mutational landscape of chemo-refractory Burkitt lymphoma” was presented.
Burkitt Lymphoma (BL) is rarely re-biopsied at time of relapse, and so the mutational landscape of relapsed BL is very ill defined. Two, young, male patients experienced relapse after completion of intensive chemotherapy within 3 months. The group aimed to identify mutations which may have contributed to therapy resistance as well as to create cell lines from the two patients in order to study the tumors in more detail.
Tumor cells from the two patients underwent whole exome sequencing at time of diagnosis (T1) and relapse (T2); unaffected peripheral blood was used to exclude germline variants. Samples from T2 were used to create the novel cell lines (CLs) which were sequenced and karyotyped.
Key Highlights:
- Total number of coding mutations:
- In first patient: T1 = 78, T2 = 84, CL= 63
- In second patient: T1= 43, T2 = 66, CL= 70
- All samples had multiple missense mutations (5–7) in MYC and had evidence of clonal heterogeneity
- First patient:
- Harbored a TP53 (R248) mutation that was clearly selected for during chemotherapy, where the variant allele fraction increased from 2–93% between T1 and T2
- Missense mutations were acquired by 19 genes at T2 including: CD14, GSTM3, BCR, and ELMO3
- In CL, several genomic rearrangements were reported by karyotyping: Y,t(8;14)(q24.21;q32), del(10)t(10;22)(p1?3;q11.2), t(13;17)(q3?2;q11.2), del(17)(p11.2), and -22
- Second patient:
- Multiple frameshift mutations present in T1, T2, and CL; found in CCND3, BAX, ARID1A, ARID1B, DDX5, DETD1B, TSFM, SP3, and TFAP4
- T2 and CL had additional acquired missense or nonsense mutations in ZFP36L2, CCL7, FAM13C, and IKBKB
- CL had 3 dominant clones by karyotype
- In CL, the rearrangements observed were: del(2)(p21p23), t(8;14)(q24.21;q32), t(1;12)(q12;q24), and +7
- The frameshift mutations in ZFP36L2 and BAX were homozygous in CL
The group stated that, to their knowledge, “these are the first BL cell lines that have been well-characterized with respect to the serial acquisition of mutations after exposure to chemotherapy and with knowledge of germline variants.” The poster concluded by stating that their CLs are a useful tool which will enable oncogene co-operation, clonal evolution, chromatin remodeling, RNA processing, and apoptosis to be studied in BL.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?