All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Anti-CD30 CAR T-cell consolidation after auto-HSCT in patients with high-risk CD30+ lymphoma: results from a phase I trial
High-dose chemotherapy followed by autologous hematopoietic stem cell transplantation (auto-HSCT) is the standard of care for patients with relapsed Hodgkin lymphoma.1 There is a need for alternative consolidation strategies after auto-HSCT in patients at a high risk of relapse. As previously covered by the Lymphoma Hub, anti-CD30 chimeric antigen receptor (CAR) T-cell therapy could be a promising posttransplant consolidation therapy for patients with CD30+ Hodgkin and non-Hodgkin lymphoma who are at high risk of relapse.1
Recently, results were published from a phase I trial (NCT02663297) assessing the safety of anti-CD30 CAR T-cell therapy as consolidation after auto-HSCT in patients with high-risk CD30+ lymphoma by Grover et al. in The Lancet Haematology. We summarize the key findings below.
Study design and patient population1
- Multicenter, single-arm, phase I dose escalation trial.
- Included patients aged ≥3 years with relapsed high-risk classical Hodgkin lymphoma or CD30+ non-Hodgkin lymphoma who were eligible for high-dose chemotherapy and auto-HSCT.
- Patients underwent conditioning with carmustine, etoposide, cytarabine, and melphalan (BEAM) followed by auto-HSCT.
- Patients received a single dose of CAR T-cells at one of three dose levels:
- Dose level 1: 2 × 107 cells/m2
- Dose level 2: 1 × 108 cells/m2
- Dose level 3: 2 × 108 cells/m2
- The primary endpoints were the maximum tolerated dose of CAR T-cells, safety, and tolerability.
- Secondary endpoints included progression-free survival and overall survival.
Key findings1
Patient characteristics
- In total, 18 patients received treatment, of which 11 had Hodgkin lymphoma, six had T-cell lymphoma, and one had grey zone lymphoma.
- The median age was 43 years (range, 16–76 years).
- Four, five, and nine patients were treated at Dose levels 1, 2, and 3, respectively.
Safety
- No dose-limiting toxicities were observed; Dose level 3 was established as the maximum tolerated dose
- No treatment-related deaths occurred.
- One patient treated at Dose level 3 experienced Grade 1 cytokine release syndrome (Table 1).
Table 1. Treatment-emergent adverse events*
|
Treatment-emergent adverse events, n |
Grade 1–2 |
Grade 3 |
Grade 4 |
|
*Adapted from Grover, et al.1 |
|||
|
Anemia |
1 |
1 |
0 |
|
Aspartate aminotransferase increased |
4 |
0 |
0 |
|
Cytokine release syndrome |
1 |
0 |
0 |
|
Diarrhea |
3 |
0 |
0 |
|
Dizziness |
2 |
0 |
0 |
|
Fatigue |
3 |
0 |
0 |
|
Headache |
2 |
0 |
0 |
|
Hypocalcemia |
2 |
0 |
0 |
|
Lymphocyte count decreased |
6 |
2 |
0 |
|
Nausea |
6 |
0 |
0 |
|
Neutrophil count decreased |
3 |
0 |
1 |
|
Platelet count decreased |
4 |
1 |
0 |
|
Rash maculopapular |
1 |
1 |
0 |
|
Vomiting |
2 |
0 |
0 |
|
White blood cell count decreased |
4 |
2 |
0 |
Efficacy
- After a median follow-up of 48.2 months, 44% of patients relapsed (Dose level 1, n = 3; Dose level 2, n = 1; Dose level 3, n = 4).
- Median progression-free survival was 32.3 months and not reached for all treated patients and patients with Hodgkin lymphoma, respectively.
- The median overall survival was not reached for all treated patients.
- The 2-year survival rates are shown in Figure 1.
- All patients with Hodgkin lymphoma are alive, while five patients with T-cell lymphoma have died (relapse, n = 4; unrelated lung cancer, n = 1).
Figure 1. 2-year progression-free survival and overall survival rates*
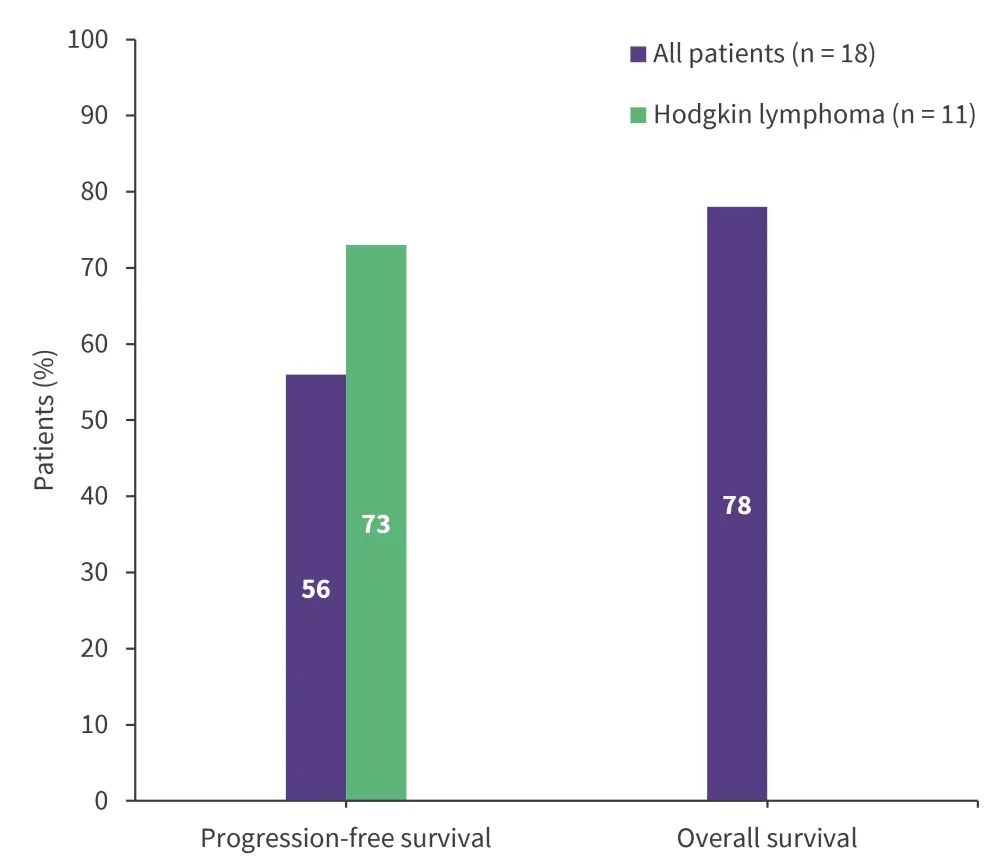
*Adapted from Grover, et al.
| Key learnings |
|
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?

