All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Johnson & Johnson, Roche and sobi, and supported through educational grants from Bristol Myers Squibb, Incyte and Lilly. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Nivolumab monotherapy in R/R cHL: 12-month follow up of phase 2 Checkmate 205 trial
On 3–6 December 2016, the Annual Meeting & Exposition of the American Society of Hematology (ASH) took place in San Diego, CA.
On Monday 5th December, an oral abstract session was held between 4:30pm and 6:00pm in the “Hodgkin Lymphoma and T/NK Cell Lymphoma – Clinical Studies Program: Oral and Poster Abstracts” category. This session was moderated by Stephen Ansell, MD, PhD, of the Mayo Clinic, and Anas Younes, MD, of the University of Texas M.D. Anderson Cancer Center.
Abstract #1110 was presented during this session, titled “Checkmate 205 Update with Minimum 12-Month Follow Up: A Phase 2 Study of Nivolumab in Patients with Relapsed/Refractory Classical Hodgkin Lymphoma” by John Timmerman, MD, of the University of California at Los Angeles, CA, and colleagues.
The phase 2 CheckMate 205 study (NCT02181738) aims to evaluate the safety and efficacy of nivolumab monotherapy in patients with classical Hodgkin Lymphoma (cHL) who have relapsed after Autologous Stem Cell Transplant (ASCT). Data presented in this abstract concerned the 80 patients in cohort B (patients who had received brentuximab vedotin after failing ASCT) and 63 patients in cohort A (patients who relapsed after ASCT but were BV-naïve):
Cohort B
- Median age was 37 years (18–72) and median number of prior therapies was 4 (3–15)
- Median follow-up duration = 15.4 months (1.9–18.5)
- Number of patients who remained on therapy = 43 (54%)
- 95% of evaluable patients demonstrated a reduction in tumor burden
- IRRC-assessed ORR = 68% (95% CI, 56%, 78%)
- CR = 8% (3%, 16%); PR = 60% (48%, 71%)
- IRRC-assessed median PFS = 14.8 months (95% CI, 11.3 month, NA); 12-month PFS = 54.6% (95% CI, 40.9%, 66.4%)

- 12-month OS = 94.9% (median OS not reached)
- The most common reasons for discontinuation of nivolumab were disease progression (n=19), ASCT (n=7) and AEs (n=5)
- The most common grade 3–4 drug-related AEs = increased lipase (8%), neutropenia (5%), and increased aspartate aminotransferase (4%)
- The most common SAEs (all ≤4%) = tumor progression, meningitis, pneumonia, pyrexia, arrhythmia, and infusion reaction

Cohort A
- 93% of evaluable patients demonstrated a reduction in tumor burden
- IRRC-assessed ORR = 68% (95% CI, 55%, 79%)
- CR = 22% (14/22); PR = 46% (29/63)

- Median time to response = 2 months (range 2–6)
- Median DoR = not reached
- Median PFS = not reached
- Estimated 9-month PFS = 68%; estimated 9-month OS = 97%

It was concluded that monotherapy with nivolumab in relapsed cHL has an acceptable safety profile and longer remissions were observed, including PRs, in this report of an extended 12-month follow-up.

Abstract:
Introduction: Nivolumab, a fully human IgG4 monoclonal antibody targeting programmed death receptor-1, has recently been FDA approved for classical Hodgkin lymphoma (cHL) that has relapsed or progressed after autologous stem cell transplantation (ASCT) and post-transplantation brentuximab vedotin (BV). CheckMate 205 (NCT02181738) is a phase 2, international, multicohort study evaluating nivolumab monotherapy in patients with cHL after failure of ASCT. At minimum 6 months' follow-up of Cohort B (205B) which included patients who had received BV after disease recurrence following ASCT, objective response rate (ORR) per independent radiologic review committee (IRRC) was 66% and 6-month progression-free survival (PFS) was 77%, with an acceptable safety profile (Younes et al. Lancet Oncol 2016; Jul 20 [Epub ahead of print]). Here we report outcomes with longer follow-up (minimum 12-month follow-up) in 205B. Primary results from Cohort A, which enrolled patients who relapsed after ASCT but were BV-naïve, will also be presented for the first time as data were not available at time of abstract submission.
Methods: CheckMate 205 was designed to evaluate the efficacy and safety of nivolumab monotherapy in patients with cHL who relapsed after ASCT in 3 cohorts: 205A (BV-naive patients; n = 63); 205B (BV after failed ASCT; n = 80); 205C (BV at any time prior to study drug; n = 100). Nivolumab was given at 3 mg/kg intravenously every 2 weeks until disease progression or unacceptable toxicity in 205A and 205B. The primary endpoint was IRRC-assessed ORR.
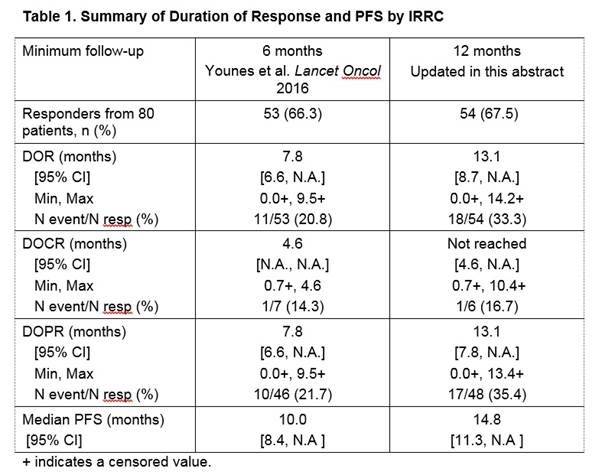
Results: 80 patients were treated in Cohort 205B; the median age was 37 years (range 18—72). Patients had received a median of 4 prior regimens (range 3—15). At data cut-off (April 2016) with median duration of follow-up of 15.4 months (range 1.9—18.5), 43 patients (54%) still remained on therapy. IRRC-assessed ORR for patients in 205B was 68% (95% confidence interval [CI], 56%, 78%). CR and partial response (PR) rates per IRRC were 8% (3%, 16%) and 60% (48%, 71%), respectively. With longer follow-up, the median duration of response was prolonged to 13.1 months (95% CI, 8.7, not reached; range, 0.0+, 14.2+). The median duration of CR (DOCR) was not reached (95% CI, 4.6, not available [NA]; range, 0.7+, 10.4+) and the median duration of PR was 13.1 months (95% CI, 7.79, NA; range, 0.0+, 13.4+) (Table 1). IRRC median PFS was 14.8 months (95% CI, 11.3 months, NA); 12-month PFS was 54.6% (95% CI, 40.9%, 66.4%), and 12-month overall survival (OS) was 94.9% (median OS not reached). Of 37 patients (46%) who discontinued nivolumab, the most common reasons were disease progression (n = 19 [24%]), allogeneic stem cell transplant (n = 7 [9%]) and adverse events (n = 5 [6%]).
Seventy-four patients (93%) had drug-related adverse events (AEs) of any grade. The most common drug-related AEs were fatigue (28%), infusion reaction (20%), arthralgia (15%), and rash (15%). 29% of patients had Grade 3-4 drug-related AEs; the most common were increased lipase (8%), neutropenia (5%), and increased aspartate aminotransferase (4%). The most common serious AEs were pyrexia, pneumonia, tumor progression, arrhythmia, infusion reaction, and meningitis (≤4% each).
Conclusions: In this report with extended 12-month follow-up, longer remissions are noted following nivolumab monotherapy in relapsed cHL, including durable PRs in heavily pretreated patients. Nivolumab has an acceptable safety profile, similar to previously reported. Primary results following nivolumab monotherapy in BV-naïve patients with cHL who progressed after ASCT (Cohort 205A) will also be presented at the meeting.
Study funding: Study funded by Bristol-Myers Squibb. Professional writing assistance was provided by K. Jesien of Caudex and funded by Bristol-Myers Squibb.

References
Your opinion matters
In your experience, when do most CRS/ICANS events occur after lisocabtagene maraleucel infusion?