All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
ASH 2016 | Sequential RCHOP, Radioimmunotherapy and Rituximab Maintenance Improves Early Outcomes in Advanced Stage Follicular Lymphoma: 5 Year Outcomes from SWOG 0801
The 58th Annual Meeting & Exposition of the American Society of Hematology’s (ASH) took place in San Diego, CA, and on December 3rd, Paul M. Barr, M.D., from the Wilmot Cancer Institute, University of Rochester, Rochester, NY, presented data from the Phase-II single arm SWOG 0016 trial into the use of consolidative radioimmunotherapy (RIT) and sequential maintenance rituximab (MR) after chemoimmunotherapy induction in advanced stage FL.
Highlights:
- Pts received R-CHOP (6 cycles, last 2 no R), then iodine-131 tositumomab and subsequent MR for 4 years at 3 month itervals
- 84 pts with treatment naïve stage III/IV or bulky stage II FL received treatment
- FLIPI risk scores: High=42%, Intermediate=40%, Low=18%
- 73 pts completed R-CHOP and iodine-131 tositumomab
- ORR=99%, CR=59pts, PR=23pts
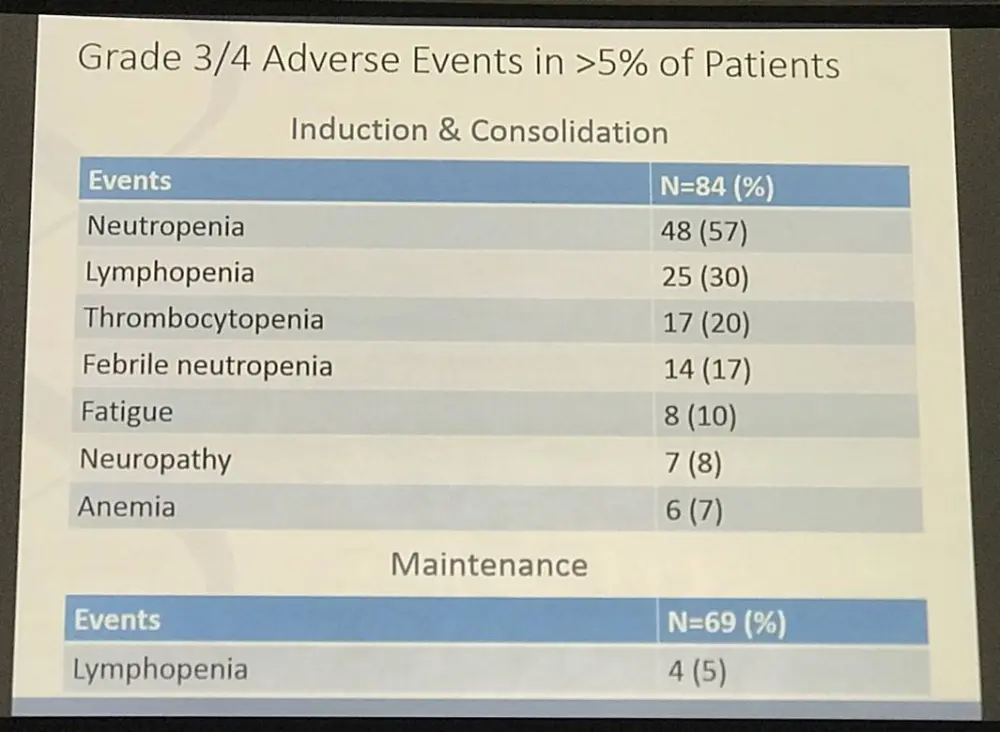
- AEs Grade 3 or higher ≥20% pts were neutropenia (57%), leukopenia (40%), thrombocytopenia (20%)
- 69pts registered for MR, 42pts completed MR at 4 years, 27pts discontinued
- Common discontinuation reasons = infection (8pts), patient preference (8pts).
- AEs Grade 3 or higher ≥5% pts leukopenia (5%)
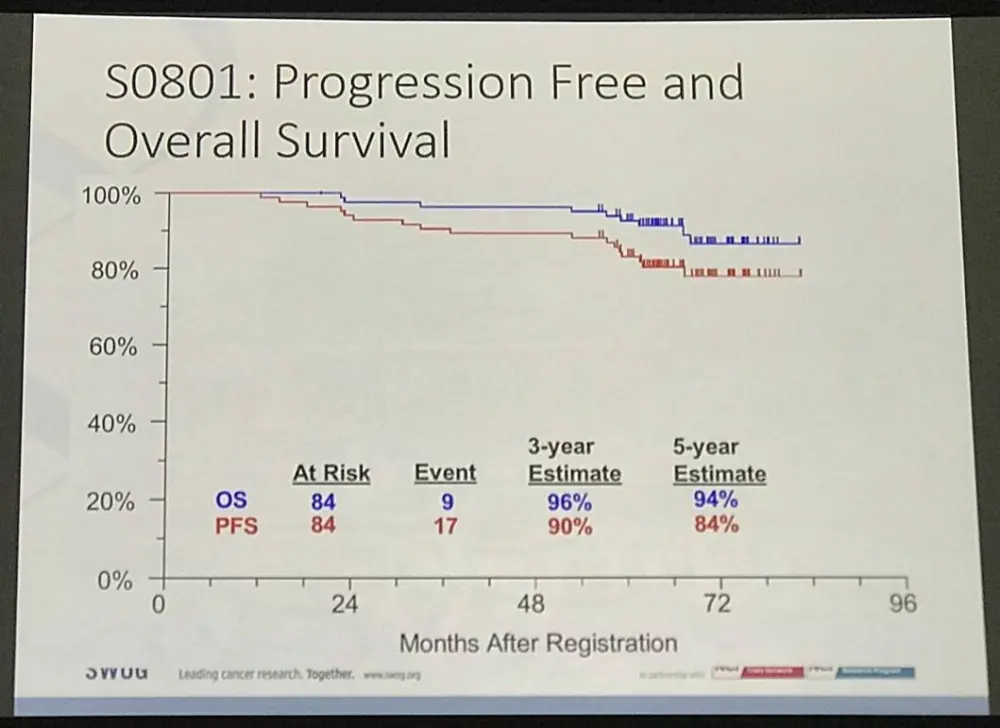
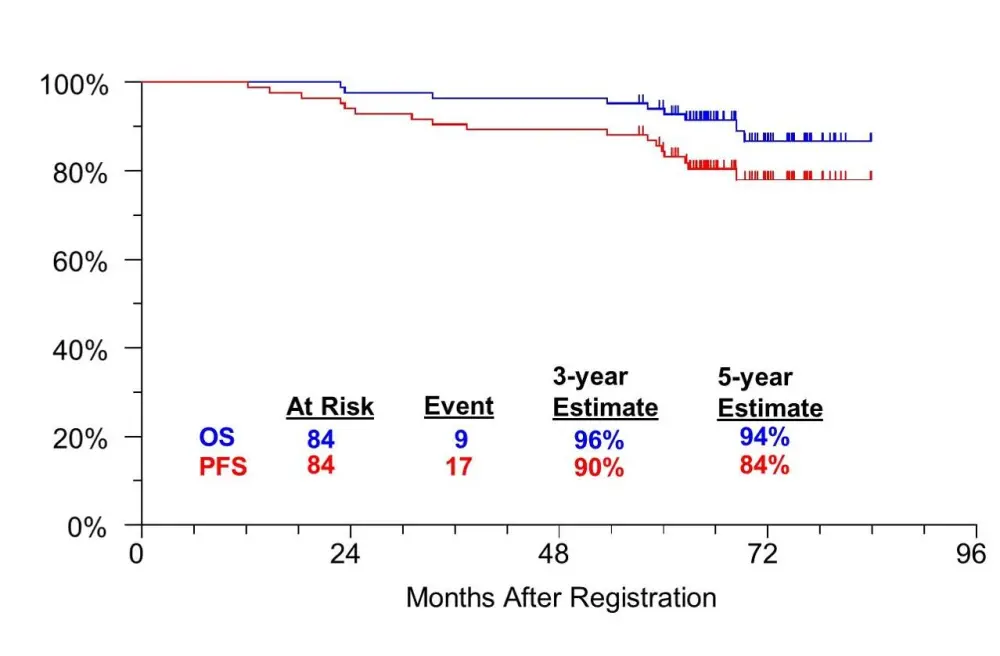
- 3 year PFS = 90%, 5 year PFS = 84%
- 3 year OS = 96%, 5 year OS = 94%
Paul Barr concluded by stating that this strategy of MR after RIT resulted in 2 year PFS of 94%, improving early outcomes, but that MR for 4 years may be unfeasible given the discontinuation rates and that given these results future studies should look at combining strong chemoimmunotherapy with RIT.
Abstract:
Background: Despite an abundance of effective therapeutic options, advanced stage follicular lymphoma (FL) remains incurable. Further, prospective trials consistently demonstrate that 20% of patients relapse within 2 years and ultimately have an inferior survival (Casulo 2015). Maintenace rituximab following chemoimmunotherapy induction is able to delay disease progression but has not demonstrated a benefit in overall survival (Salles 2011). Additionally, radioimmunotherapy (RIT) is one of the most effective single agent options in FL but is not commonly utilized as part of upfront treatment. As such, the role of both remains unclear. Based on results demonstrated with RIT consolidation in SWOG 0016 and the efficacy of rituximab maintenance, SWOG 0801 was designed as a phase 2 single arm trial, conducted to evaluate the utility of consolidative RIT and sequential maintenance rituximab following chemoimmunotherapy induction.
Methods: Eligible patients (pts) with treatment naïve stage III/IV or bulky stage II FL received RCHOP for 6 cycles (without rituximab for the last 2 cycles) followed by iodine-131 tositumomab and subsequent rituximab administered every 3 months for up to 4 years.The primary endpoint was progression-free survival (PFS) at 3 years. Secondary endpoints included 5-year overall survival (OS), overall response rate (ORR), and safety.
Results: Of 87 pts registered to this study, 85 were deemed eligible following central pathologic review. One additional patient withdrew consent and received no treatment on protocol.
Of the 84 evaluable patients, the median age was 52 years (range 29 – 80) ) and 18%, 40%, and 42%had low, intermediate and high risk FLIPI scores, respectively. Seventy-three pts completed RCHOP and I-131 tositumomab. Grade ≥3 AEs occurring ≥5% of pts included neutropenia (57%), leukopenia (40%), thrombocytopenia (20%), febrile neutropenia (17%), fatigue (10%), neuropathy (8%), anemia (7%) and hyperglycemia (5%). Reasons for discontinuation included refusal of tositumumab (6 pts), prolonged myelosuppression (2 pts), ascites (1pt), inability to provide tositumumab (1 pt), and an unrelated lower extremity wound (1 pt). Following induction and RIT, 59 complete responses and 23 partial responses were observed, for a ORR of 99% (95% CI: 93.5%, 99.9%)
Sixty nine eligible patients registered to maintenance therapy with 42 completing the 4 year treatment plan. The only grade ≥3 AE that occurred in ≥5% of pts was leukopenia (5%). Twenty-seven pts discontinued maintenance therapy, including 11 in the first 2 years and 16 in the last 2 years, due to the following reasons: infection (8 pts), patient preference (8 pts), deaths (2 pts), treatment delay (2 pts), secondary solid tumors (2 pts), bowel perforation (1 pt), joint pain (1 pt), hepatic transaminase elevation (1 pt), insurance refusal (1 pt), and dose error (1 pt).
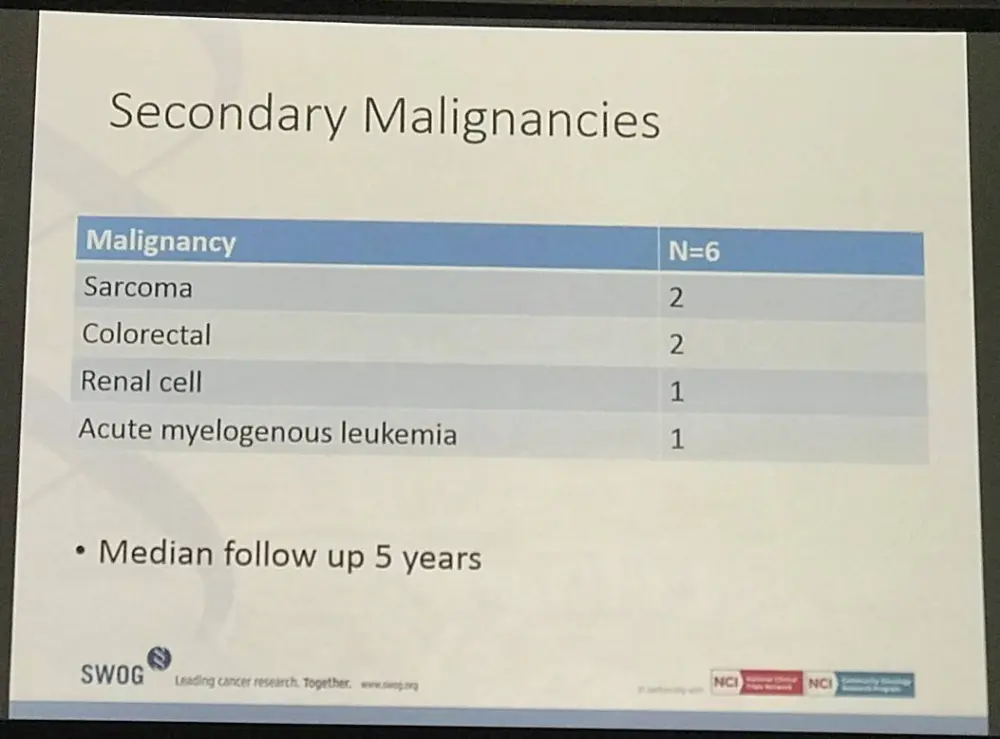
Four additional secondary malignancies were reported following completion of therapy including solid tumors (3 pts) and AML (1 pt). To date, 9 deaths have occurred due to secondary malignancies (3 pts), unknown etiology (3 pts), cardiac arrest (2 pts) and non-alcoholic cirrhosis (1 pt).
After median follow-up of 5.6 years (range 3-7 years), 17 events have occurred including 9 pts experiencing progressive FL resulting in a progression free survival of 90% (95% CI: 81.9%, 95.1%) at 3 years and 84%(95% CI: 74.5%, 90.6%) at 5 years (Figure). Three-year overall survival is 96% (95% CI: 89.3%, 98.8%) and 5-year overall survival is 94% (95% CI: 86.2%, 97.5%).
Conclusions: SWOG 0801 demonstrates near universal responses following chemoimmunotherapy and RIT. This sequential therapeutic strategy appears to improve early outcomes as 94% of pts are without disease progression at 2 years, consistent with the best results ever demonstrated for FL in the National Clinical Trials Network. However, the majority of discontinuations occurred during maintenance suggesting that rituximab over a 4-year span is not feasible for many patients due to cumulative toxicity. Future studies investigating precision strategies in high-risk FL may consider an aggressive chemoimmunotherapy induction and RIT consolidation platform to overcome early FL progression given these promising outcomes.
Support: NIH/NCI grants CA180888, CA180819, and in part by GlaxoSmithKline.
Figure: Progression-Free Survival and Overall Survival
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?