All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
BL-IPI to support risk stratification and targeted novel treatment approaches for Burkitt lymphoma
Burkitt lymphoma (BL) is a highly aggressive B-cell non-Hodgkin lymphoma. BL is curable for most patients with dose-intense multiple drug combination chemotherapy and improvements in supportive care. However, past definitions of low-risk BL have been inconsistent and >85–90% patients fall into the undifferentiated high-risk category. The lack of standardization for risk stratification in BL hinders the evaluation of targeted, individualized treatments based upon patient prognosis.
At the 62nd American Society of Hematology (ASH) Annual Meeting and Exposition held in December 2020, Adam Olszewski, Lifespan Cancer Institute, Providence, US, presented results from a retrospective cohort study that derived and validated a novel prognostic index for BL in geographically diverse patient cohorts.1 The data have subsequently been published in the Journal of Clinical Oncology.2 Adam Olszewski has shared his opinion on the development and validation of the BL International Prognostic Index (BL-IPI) with the Lymphoma Hub. Here we are pleased to summarize the study results.
Study design1,2
- The BL-IPI was developed using retrospective data from 633 patients across 30 institutions in the US (derivation cohort)
- External validation was performed using data from 457 patients across Australia, Canada, Denmark, Norway, and the UK (validation cohort)
- The primary endpoint was progression-free survival (PFS) and the secondary endpoint was overall survival (OS)
Results1,2
Patient baseline characteristics
- The baseline characteristics were similar in both cohorts (Table 1), with a median age of 46–47 years, high proportion of men, and 22–23% human immunodeficiency virus (HIV)-positive individuals. More than 75% patients in both cohorts had advanced stage BL and abnormal lactate dehydrogenase (LDH)
- Central nervous system (CNS) involvement was more frequent in the derivation cohort (19%), compared with the validation cohort (10%)
- PFS and OS at 3 years were higher in the validation cohort than in the derivation cohort, which may be explained by variation in treatment selection, differences in socioeconomic status, and healthcare systems
Table 1. Baseline characteristics1,2
|
CNS, central nervous system; CODOX-M/IVAC ± R, cyclophosphamide, vincristine, doxorubicin, high-dose methotrexate/ifosfamide, etoposide, and high-dose cytarabine with or without rituximab; ECOG, Eastern Cooperative Oncology Group; DA-EPOCH-R, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab; HIV, human immunodeficiency virus; hyperCVAD/MA ± R, cyclophosphamide, vincristine, doxorubicin, and dexamethasone/high-dose methotrexate and cytarabine with or without rituximab; IQR, interquartile range; LDH, lactate dehydrogenase; OS, overall survival; PFS, progression-free survival; PS, performance status; ULN, upper limit of normal. |
||
|
Characteristic |
Derivation cohort (US) |
Validation cohort (international) |
|---|---|---|
|
Age, median (IQR) |
47 (33–59) |
46 (34–59) |
|
≥ 40, n (%) |
401 (63) |
290 (64) |
|
≥ 60, n (%) |
146 (23) |
109 (24) |
|
Male, n (%) |
479 (76) |
351 (77) |
|
HIV-positive, n (%) |
140 (22) |
106 (23) |
|
PS ECOG ≥ 2, n (%) |
141 (22) |
131 (35) |
|
Stage 3 or 4, n (%) |
494 (78) |
363 (79) |
|
> 1 extra nodal site, n (%) |
270 (43) |
247 (54) |
|
CNS involvement, n (%) |
118 (19) |
47 (10) |
|
LDH ratio, median (IQR) |
2.5 (1.1–6.1) |
2.6 (1.1–7.1) |
|
LDH > ULN, n (%) |
465 (74) |
352 (77) |
|
LDH > 3 × ULN, n (%) |
268 (42) |
212 (46) |
|
LDH > 5 × ULN, n (%) |
178 (28) |
152 (33) |
|
Stage 1 or 2 with LDH ≤ ULN, n (%) |
53 (8) |
58 (13) |
|
First-line regimen, n (%) |
||
|
CODOX-M/IVAC ± R |
194 (31) |
298 (65) |
|
HyperCVAD/MA ± R |
195 (31) |
39 (9) |
|
DA-EPOCH-R |
181 (29) |
46 (10) |
|
Other |
63 (10) |
74 (16) |
|
Rituximab use, n (%) |
578 (91) |
432 (95) |
|
Median follow-up, months |
45 |
52 |
|
PFS at 3 years, 95% CI |
65 (61–69) |
75 (70–78) |
|
OS at 3 years, 95% CI |
70 (66–74) |
76 (72–80) |
Development of BP-IPI
- In univariable analysis, the optimal prognostic cutoffs were age ≥ 40 years, LDH > 3 × ULN, hemoglobin < 11.5 g/dL, and albumin < 3.5 g/dL
- The four best performing prognostic factors, each associated with inferior PFS in univariable analysis, that were selected for the multivariable model were age ≥ 40 years, PS ECOG ≥ 2, LDH > 3 × ULN, and CNS involvement (Table 2)
- Each risk factor was assigned equal weight and because PFS and OS were similar across groups with either two, three, or four risk factors, these were combined into one high-risk category. The final BL-IPI comprised of three risk categories: low (no risk factors), intermediate (one risk factor), and high (two to four risk factors) (Figure 1)
- There was significant discrimination of PFS (p < 0.0001) and OS (p < 0.0001) between BL-IPI categories, with 3-year PFS estimates of 92%, 72%, and 53%, and 3-year OS estimates of 96%, 76%, and 59% for low-, intermediate-, and high-risk groups, respectively
- Median PFS was estimable only in the high-risk group (46 months; 95% CI, 19–53).
Table 2. Univariable and multivariable analyses for association between candidate prognostic variables and PFS1,2
|
CI, confidence interval; CNS, central nervous system; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; LDH, lactate dehydrogenase; PS, performance status; ULN, upper limit of normal. |
||||||
|
Variable |
Univariable |
Multivariable |
||||
|---|---|---|---|---|---|---|
|
HR |
95% CI |
P |
HR |
95% CI |
P |
|
|
Age ≥ 40 years |
1.79 |
1.34–2.38 |
< 0.001 |
1.79 |
1.34–2.38 |
< 0.001 |
|
Female |
1.05 |
0.78–1.41 |
0.74 |
|
|
|
|
HIV-positive |
1.15 |
0.85–1.56 |
0.36 |
|
|
|
|
PS ECOG ≥ 2 |
2.22 |
1.69–2.92 |
< 0.001 |
2.22 |
1.69–2.92 |
< 0.001 |
|
No MYC rearrangement |
0.82 |
0.53–1.29 |
0.39 |
|
|
|
|
Stage 3 or 4 |
2.35 |
1.57–3.53 |
< 0.001 |
|
|
|
|
B symptoms |
1.23 |
0.95–1.59 |
0.12 |
|
|
|
|
> 1 extra nodal site |
1.24 |
0.95–1.60 |
0.11 |
|
|
|
|
Marrow involvement |
1.64 |
1.27–2.13 |
< 0.001 |
|
|
|
|
CNS involvement |
2.02 |
1.52–2.69 |
< 0.001 |
2.02 |
1.52–2.69 |
< 0.001 |
|
LDH > 3 × ULN |
2.12 |
1.62–2.77 |
< 0.001 |
2.12 |
1.62–2.77 |
< 0.001 |
|
Hemoglobin < 11.5 g/dL |
1.63 |
1.25–2.12 |
< 0.001 |
|
|
|
|
Albumin < 3.5 g/dL |
1.55 |
1.19–2.03 |
0.001 |
|
|
|
Figure 1. Percentage of patients according to number of risk factors1,2
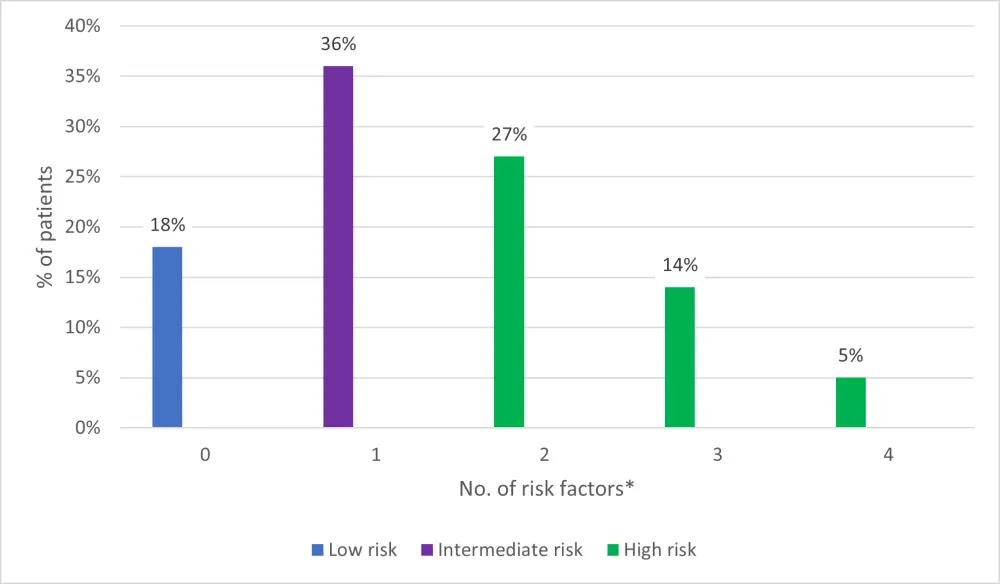
*Risk factors: Age ≥ 40; performance status ≥ 2; LDH > 3 × ULN; and CNS involvement.
Subset analyses
- No significant differences were observed in PFS or OS by LDH or stage of BL
- More than 50% of BP-IPI low-risk patients had either abnormal LDH or advanced stage lymphoma; their outcomes were similar to others in the same group, with 3-year OS rates of > 90%
- In the derivation cohort, BL-IPI was prognostic among patients with MYC rearrangement, among those receiving rituximab, and those with or without HIV infection
- In stage III or IV BL patients historically classified as high risk (78% of the derivation cohort), the BL-IPI further differentiated low-, intermediate-, and high-risk subgroups, with 3-year PFS estimates of 87%, 71%, and 52% (p < 0.001) and OS estimates of 95%, 75%, and 57%, respectively
- Prognostic values were retained by BL-IPI regardless of first line of chemotherapy
Validation
- BL-IPI categories were similar in size for both the validation and derivation cohorts and provided similar discrimination of PFS (p < 0.0001) and OS (p < 0.0001) (Table 3)
- In the validation cohort, BL-IPI remained prognostic in advanced and early-stage BL among patients receiving rituximab, and those receiving CODOX-M/IVAC ± R
Table 3. PFS and OS in derivation and validation cohorts1,2
|
CI, confidence interval; OS, overall survival; PFS, progression-free survival; yr, year. |
||||||
|
|
Derivation cohort |
Validation cohort |
||||
|---|---|---|---|---|---|---|
|
Outcome/ BL-IPI group |
n (%) |
3-yr estimate, % (95% CI) |
HR (95% CI) |
n (%) |
3-yr estimate, % (95% CI) |
HR (95% CI) |
|
PFS |
|
|
|
|
|
|
|
Low |
104 (18) |
92 (84.2–95.8) |
1.0 |
68 (15) |
96 (86.7–98.5) |
1.0 |
|
Intermediate |
206 (36) |
72 (64.8–77.5) |
4.15 (1.99–8.68) |
159 (35) |
82 (75.2–87.5) |
2.63 (1.02–6.81) |
|
High |
260 (45) |
53 (46.7–59.2) |
8.83 (4.32–18.03) |
230 (50) |
63 (56.5–69.2) |
6.17 (2.51–15.22) |
|
OS |
|
|
|
|
|
|
|
Low |
104 (18) |
96 (89.7–98.5) |
1.0 |
68 (15) |
99 (89.9–99.8) |
1.0 |
|
Intermediate |
206 (36) |
76 (69.1–81.4) |
7.06 (2.55–19.53) |
159 (35) |
85 (77.9–89.6) |
2.83 (0.99–8.13) |
|
High |
260 (45) |
59 (52.1–64.7) |
15.12 (5.58–40.99) |
230 (50) |
64 (57.6–70.2) |
7.59 (2.78–20.72) |
Conclusion
The BL-IPI is a novel, simple prognostic index for BL, developed using a real-world US cohort and validated using an international patient population, demonstrating applicability to diverse clinical settings across the world. However, as the study uses retrospective data, the BL-IPI should be interpreted with caution and further validation using clinical trial data would be of value, as well as validation for the endemic BL variant.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?