All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
CD20-directed CAR T-cell therapies in the treatment of relapsed/refractory non-Hodgkin lymphoma: Results from two phase I trials
CD20 is an effective therapeutic target for B-cell non-Hodgkin lymphoma (B-NHL), and the CD20-directed chimeric antigen receptor (CAR) T-cell therapy, C-CAR066, has demonstrated high in vitro and in vivo antitumor activity. C-CAR039 is a novel second generation 4-1BB bispecific CAR T-cell therapy targeting both CD19 and CD20 antigens, and it similarly shows high antitumor activity both in vitro and in vivo. At the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Aibin Liang presented initial findings from two trials, one evaluating C-CAR066 (NCT04036019)1 and the other evaluating C-CAR039 (NCT04317885)2.The key findings are presented here.
Study designs1,2
- A phase I, first-in-human, open-label trial of C-CAR066 was conducted in two sites in China, in patients aged ≥18 years and with relapsed/refractory (R/R) B-NHL after failing CD19 CAR T-cell therapy.
- A phase I, open-label, dose escalation trial of C-CAR039 was conducted in four sites in China, in patients ≥18 years with R/R B-NHL, including diffuse large B-cell lymphoma (DLBCL), follicular lymphoma, and mantle cell lymphoma.
- Patients were given C-CAR066 or C-CAR039 infusion, as shown in Figure 1.
- For both trials, primary endpoints were incidence and severity of treatment emergent adverse events. Secondary endpoints included overall response rate (ORR), duration of response, progression-free survival, and overall survival, and exploratory endpoints were CAR T cell expansion and persistence.
Figure 1. Treatment schema*
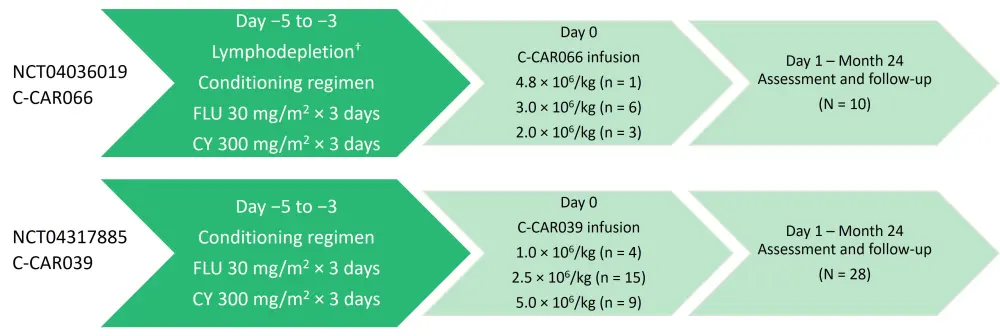
CY, cyclophosphamide; FLU, fludarabine.
*Adapted from Liang, et al.1,2
†Bridging therapy was permitted.
Baseline characteristics
The baseline characteristics for the patients included in the C-CAR0661 and C-CAR0392 trials are presented in Table 1.
Table 1. Baseline characteristics*
|
ASCT, autologous stem cell transplant; BTK, Bruton’s tyrosine kinase; CAR, chimeric antigen receptor; CR, complete response; DLBCL, diffuse large B-cell lymphoma; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance status; FL, follicular lymphoma; IPI, International Prognostic Index; NA, not applicable; NHL, non-Hodgkin lymphoma; NOS, not otherwise specified; PMBCL, primary mediastinal large B-cell lymphoma; PR, partial response; tFL, transformed follicular lymphoma. |
||
|
Characteristic |
C-CAR066 anti-CD20 CAR T-cell therapy |
C-CAR039 anti-CD20/CD19 bispecific CAR T-cell therapy |
|---|---|---|
|
Median age (range), years |
55.5 (41–67) |
55.5 (28–71) |
|
Male sex, % |
50 |
68 |
|
NHL subtype, % |
|
|
|
DLBCL, NOS |
80 |
89 |
|
tFL |
20 |
4 |
|
PMBCL |
0 |
4 |
|
FL |
0 |
4 |
|
ECOG PS, % |
|
|
|
0 |
10 |
64 |
|
1 |
90 |
36 |
|
IPI score 3–4/5, % |
60 |
25 |
|
Ann Arbor stage III/IV, % |
90 |
75 |
|
Double-expressor lymphoma, % |
40 |
29 |
|
Median number of prior lines of therapy (range) |
5 (2–6) |
3 (1–5) |
|
Number of prior lines of therapy, % |
|
|
|
2 |
10 |
4 |
|
3 |
0 |
36 |
|
4 |
30 |
14 |
|
5 |
40 |
25 |
|
6 |
20 |
21 |
|
Prior therapies, % |
|
|
|
ASCT |
20 |
18 |
|
BTK inhibitor |
20 |
29 |
|
Lenalidomide |
60 |
32 |
|
Best response to prior CAR T-cell therapy, % |
|
|
|
CR |
20 |
NA |
|
PR |
80 |
NA |
|
Median DOR of prior CAR T-cell therapy (range) |
2.1 (0.7–12.6) |
NA |
|
Bridging therapy, % |
40 |
18 |
Results
C-CAR066 anti-CD20 CAR T-cell therapy1
Safety
- In total, eight patients (80%) had Grade 1–2 cytokine release syndrome (CRS) and one patient (10%) had Grade 4 CRS. The median days to onset and to resolution of CRS were 2 days (range, 1–9 days) and 4 days (range, 2–17 days), respectively.
- Adverse events (AEs) of Grade ≥3 included neutropenia (80%), anemia (50%), thrombocytopenia (30%), and infections (10%).
- Cytopenias were mostly related to cyclophosphamide/fludarabine lymphodepletion and were reversible.
- No immune effector cell-associated neurotoxicity syndrome (ICANS) occurred in any of the patients.
Efficacy
- Patients demonstrated an ORR of 100% and a complete response rate (CRR) of 70%. The median time to complete response (CR) was 2.7 months (range, 0.9–2.9 months) (Table 2).
- Four patients remained in CR after 10 months.
- C-CAR066 proliferation and expansion in the peripheral blood correlated with B-cell depletion.
Table 2. Response rates*
|
CR, complete response; CRR, complete response rate; DOR, duration of response; NR, not reached; ORR, overall response rate; PRR, partial response rate. |
|
|
Response assessed by investigator |
N = 10 |
|---|---|
|
ORR, % |
100 |
|
CRR |
70 |
|
PRR |
30 |
|
Median time to response, months (range) |
1.0 (0.9–2.7) |
|
Median DOR, months (range) |
NR |
|
Median time to CR, months (range) |
2.7 (0.9–2.9) |
|
Median duration of CR, months (range) |
NR |
|
Median follow-up, months (range) |
4.2 (1.2–11.7) |
C-CAR039 anti-CD20/CD19 bispecific CAR T-cell therapy2
Safety
- In total, 93% of patients developed CRS, although only 4% of patients had Grade ≥3 CRS (Table 3).
- Median days to onset and resolution of CRS were 2.5 days (range, 0–10 days) and 4 days (range, 1–25 days), respectively (Table 3). Shorter duration of CRS onset and longer duration of resolution were noted in higher dose groups.
- ICANS occurred at Grade 1 in two patients; both were in the 5.0 × 106 CAR-T cell/kg dosing group (Table 3). Infections were common (54%), but Grade 3 infection only occurred in one patient.
- Hematologic Grade ≥3 AEs included leukopenia (89%), neutropenia (89%), lymphopenia (96%), anemia (32%), thrombocytopenia (30%), and infection (4%).
- Other Grade ≥3 AEs were infrequent and included hypertriglyceridemia (4%), hypokalemia (4%), increased alanine aminotransferase (7%), and increased aspartate aminotransferase (7%).
Table 3. CRS and ICANS in patients treated with different doses of C-CAR039
|
CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome. *Adapted from Liang et al.2 |
||||
|
Variable |
All |
1.0 × 106/kg |
2.5 × 106/kg |
5.0 × 106/kg |
|---|---|---|---|---|
|
CRS |
||||
|
Median days to onset (range) |
2.5 (0–10) |
7 (2–10) |
3.5 (1–10) |
1 (0–9) |
|
Median days to resolution (range) |
4 (1–25) |
2.5 (1–7) |
4.5 (1–25) |
4 (1–7) |
|
CRS, % |
|
|
|
|
|
Any grade |
93 |
100 |
93 |
89 |
|
Grade ≥3 |
4 |
0 |
7 |
0 |
|
Most common symptoms of any grade, % |
|
|
|
|
|
Pyrexia |
100 |
100 |
100 |
100 |
|
Hypotension |
23 |
25 |
29 |
13 |
|
Hypoxemia |
0 |
0 |
0 |
0 |
|
CRS management, % |
|
|
|
|
|
Tocilizumab alone |
14 |
0 |
13 |
22 |
|
Corticosteroids alone |
4 |
0 |
7 |
0 |
|
Tocilizumab and corticosteroids |
4 |
0 |
7 |
0 |
|
ICANS |
||||
|
Median days to onset (range) |
16 (4–28) |
NA |
NA |
16 (4–28) |
|
Median days to resolution (range) |
31.5 (11–52) |
NA |
NA |
31.5 (11–52) |
|
Neurologic events, % |
|
|
|
|
|
Any grade |
7 |
0 |
0 |
22 |
|
Grade ≥3 |
0 |
0 |
0 |
0 |
|
Most common symptoms of any grade, % |
|
|
|
|
|
Tremor |
100 |
0 |
0 |
100 |
|
Confusion |
0 |
0 |
0 |
0 |
|
ICANS management, % |
|
|
|
|
|
Corticosteroids |
4 |
NA |
NA |
11 |
|
Tocilizumab |
0 |
NA |
NA |
0 |
Efficacy
- A total of 27 patients were evaluable for investigator-assessed efficacy. For the overall patient cohort, CRR was 85% and ORR was 93%. Patients with DLBCL had a 92% ORR and an 83% CRR.
- Median time to first response was 1 month (range, 0.9–1.6 months), and median time to CR was 1 month (range, 0.9-6.0 months).
- CRR was consistent across key subgroups.
- Median follow-up was 7 months (range, 1.9–17.2 months) and the progression-free survival rate at 6 months was 83% (95% confidence interval, 69–100). Median duration of response was not reached.
- C-CAR039 proliferation and expansion in the peripheral blood correlated with B-cell depletion.
Conclusion
The novel anti-CD20 CAR T-cell therapy, C-CAR066, demonstrated a favorable safety profile and encouraging clinical benefit in patients with R/R DLBCL following failure of CD19-directed CAR-T cell therapy. Similarly, the anti-CD20/CD19 bispecific CAR T-cell therapy, C-CAR039, demonstrated a satisfactory safety profile and promising efficacy in patients with R/R B-NHL. However, the findings were limited by a small sample size in both studies. Further evaluation in more patients, with a longer follow-up, to confirm safety, efficacy, and duration of response is underway.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average vein-to-vein time when treating patients with DLBCL with a reimbursed CAR T-cell therapy (from apheresis to infusion)?