All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
EHA 2017 | Immunotherapy for DLBCL and HL – the rationale, current agents, and is HCT still needed?
On Friday 23rd June, during the 22nd Congress of the European Hematology Association (EHA) in Madrid, Spain, the LH attended the “Immunotherapy in Lymphoma” Educational Session chaired by Andreas Engert, MD, from the University Hospital of Cologne, Germany.
The role of the microenvironment in the pathogenesis of B-Cell Lymphomas
The first talk was given by G. Lenz from the Translational Oncology Department of the University of Münster, Münster, Germany, who discussed the pathogenesis of B-Cell Lymphomas with a particular focus on contributions by the microenvironment.
Diffuse Large B-Cell Lymphoma (DLBCL)
DLBCL represents a heterogeneous diagnostic category with multiply morphologic variants that can be distinguished: Centroblastic, Immunoblastic, Anaplastic Large B-Cell, and Plasmablastic variants. There are also subtypes that are distinguished clinically including Nodal DLBCL, Primary Mediastinal B-Cell Lymphoma (PMBCL; read more here), and Primary Central Nervous System Lymphoma (PCNSL). Moreover, DLBCL demonstrates heterogeneous responses to conventional treatment. It has been found that patients with Germinal Center B-Cell-Like (GCB) DLBCL have higher Progression-Free Survival (PFS) and Overall Survival (OS) compared to patients with Activated B-Cell-Like (ABC) DLBCL (Lenz et al. NEJM. 2008). It was mentioned that the different molecular subtypes of DLBCL are addicted to different oncogenic pathways; this was covered in detail by Riccardo Dalla-Favera, MD, from Columbia University, New York, NY, during ICML 2017; read more here.
Lenz then went on to discuss the different studies which determined the importance of the microenvironment in DLBCL, beginning with a prospective, single-center evaluation of 72 patients with DLBCL between 1987 and 1994. This analysis found that a higher proportion of CD4+ T-cells in pre-treatment tumor biopsies significantly correlated with patient outcome; patients with increased numbers of CD4+ T-cells versus other patients had significantly longer 5-year Failure-Free Survival (FFS; 72% v 43%, respectively; P = 0.04) and 5-year OS (65% v 38%, respectively; P = 0.05). In multivariate analysis, the International Prognostic Index (IPI) score and >20% infiltrating CD4+ T-cells in the pre-treatment biopsy were significant independent predictors of Relapse-Free Survival (RFS) and OS. Overall higher levels of CD4+ cells in the area of DLBCL predicts a more favorable outcome (Ansell et al. JCO. 2001).
More recently, mRNA and antigen expression of different immune cells has been analyzed in pre-treatment tumor samples of patients with high-risk DLBCL from a Nordic phase II study using gene expression microarray and immunohistochemistry. Patients were treated with dose-dense chemoimmunotherapy and CNS prophylaxis. Expression of CD68 and CD68+ macrophage counts were associated with favorable outcome. In patients with high and low CD68 mRNA levels, 5-year PFS rates were 83% and 43%, respectively (P = 0.007), and OS rates were 83% and 64%, respectively. In patients with high and low CD68+ macrophage counts, 5-year PFS rates were 74% and 40%, respectively (P = 0.003), and OS rates were 90% versus 60% (P = 0.009). Low CD68+ macrophage count retained its prognostic impact on OS with age-adjusted IPI (RR, 5.0; 95% CI, 1.024–19.088; P = 0.017). On the other hand, in patients treated with chemotherapy, high CD68+ macrophage count was associated with poor PFS (40% vs. 72%; P = 0.021) and OS (39% vs. 72%; P = 0.015). Overall, these findings indicate that macrophages exhibit a dual, treatment-specific role in DLBCL. For chemoimmunotherapy treated patients, high pre-treatment CD68 mRNA levels and CD68+ macrophage numbers predict a favorable outcome (Riihijärvi et al. Haematologica. 2015).
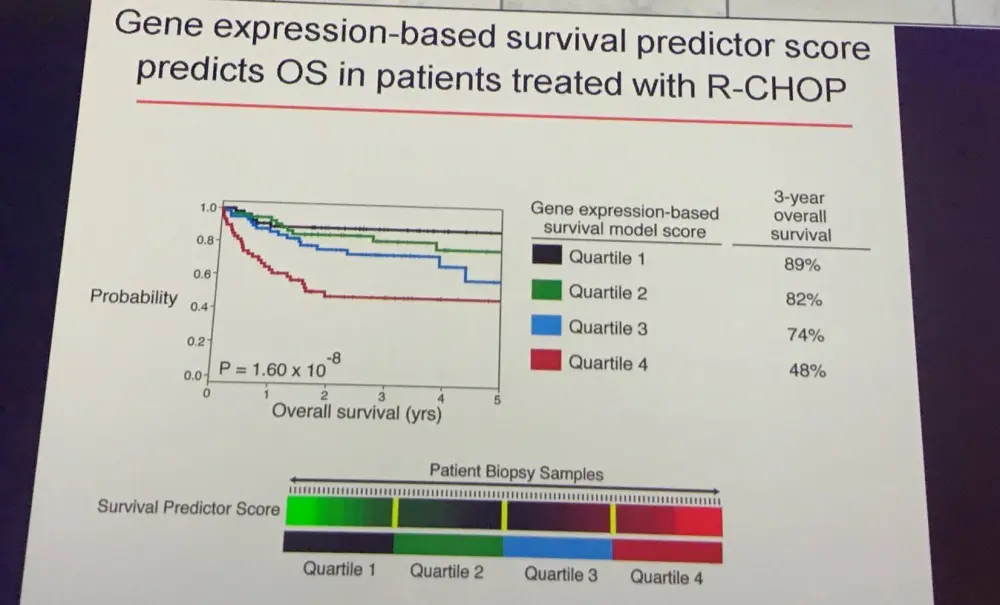
After this, Lenz discussed how different gene expression signatures of the microenvironment influence patient survival. Gene Expression Profiling (GEP) of pre-treatment biopsy samples from patients treated with CHOP or R-CHOP was performed using Affymetrix U133 plus 2.0 microarrays. Cell suspensions from three biopsy specimens were separated by means of flow cytometry into a CD19+ malignant subpopulation and a CD19- non-malignant subpopulation. It was found that GCB signature genes were more highly expressed in malignant compared to non-malignant cells and two other signatures, termed stromal-1 and stromal-2, were more highly expressed in non-malignant cells. Genes of each signature are shown in the table below:
|
Stromal-1 signature |
Stromal-2 signature |
|---|---|
|
Extracellular matrix: fibronectin, osteonectin, various collagen and laminin isoforms, and thrombospondin |
Components of caveolae: CAV1, CAV2, and EHD2 |
|
Modifiers of collagen synthesis: LOXL1 and SERPINH1 |
Regulators of angiogenesis: VEGFR2, GRB10, integrin α9, TEK, ROBO4, ERG |
|
Extracellular matrix remodeling: MMP2, MMP9, MMP14, PLAU, and TIMP2 |
Endothelial genes: EGFL7, MMRN2, GPR116, and SPARCL1 |
|
Connective-tissue growth factor |
Endothelial markers: von Willebrand factor, CD31, PECAM1 |
|
Monocytic lineage: CEBPA, CSF2RA |
Adipocyte genes: ADIPOQ, FABP4, RBP4, and PLIN. |
It was found that high expression of the stromal-1 signature identifies tumors with vigorous extracellular-matrix deposition and infiltration by cells of the monocytic lineage. As the two signatures were synergistic in predicting survival, they were combined into a “stromal score”: high values were associated with poorer outcome. The stromal score was variably present in GCB as well as ABC DLBCL, indicating both stromal signatures represent biologic attributes of the tumor microenvironment that can be gained during pathogenesis. Stromal score also correlates with tumor blood vessel density (Lenz et al. NEJM. 2008).
Next, Lenz discussed genetic aberrations in tumor cells that can influence the response of the immune system. For example, aberrations of B2M and CD58 result in escape from immune-surveillance. The talk focused in detail on the PD-1 cascade, activates regulatory T-cells. The PD-1 receptor and its ligands PD-L1 and PD-L2 function as negative regulators of T-cell activation. PD-L1 and PD-L2 are expressed among others on antigen presenting cells, epithelial cells, endothelial cells, and tumor cells. PD-L1 is expressed in 20–70% of DLBCL cases. Data vary greatly, as different antibody clones and different cut-off values are used for immunohistochemical analysis. So far, it appears that PD-L1 is expressed more highly in ABC DLBCL (Gravelle et al. Oncotarget. 2017). This has clinical implications, as we are beginning to exploit the PD-1 cascade therapeutically with agents such as nivolumab, pembrolizumab, and MEDI4736.
Hodgkin Lymphoma (HL)
Lenz then focused his talk on HL, which is characterized by excellent prognosis and a unique microenvironment; Hodgkin Reed-Sternberg (RS) cells express CD30 and are surrounded by infiltrating cells. Cross-talk occurs between RS cells and cells of the microenvironment. Moreover, activation of oncogenic pathways (such as JAK-STAT, NF-kB, and tyrosine receptor kinase) by signaling factors of the microenvironment (Steidl et al. JCO. 2011). Data suggests that the microenvironment also affects patient survival and genetic aberrations that are frequently present are associated with escape from immune-surveillance.
The talk then focused on how the microenvironment can influence patient survival. In expression-profile studies of diagnostic lymph-node specimens obtained from classical HL (cHL) patients, it was found that overexpression of a macrophage signature was associated with the failure of primary treatment. Using immunohistochemical analysis in an independent set of samples from 166 patients, it was found that increased numbers of CD68+ cells in the diagnostic sample was associated with adverse outcome. Multivariate analysis identified that the number of CD68+ cells was also associated with the outcome of secondary treatment, independently of the IPI score (Steidl et al. NEJM. 2010).
As for DLBCL, Lenz also discussed genetic aberrations in HL tumor cells that can influence the response of the immune system. 9p24 aberrations are frequent events in cHL. By integrating high-resolution copy number data with transcriptional profiles, the immunoregulatory genes PD-L1 and PD-L2 were identified as key targets at the 9p24.1 amplification peak in HL cell lines. These findings were extended using laser-capture micro-dissected primary Hodgkin RS cells and found that the PD-L1/9p24.1 amplification is restricted to nodular sclerosing HL. Furthermore, in cHL the extended 9p24.1 amplification region also included the JAK2 locus. Amplification of JAK2 specifically induced PD-L1 transcription and enhanced sensitivity to JAK2 inhibition. Thus, 9p24.1 amplification is disease-specific and increases both gene dosage of PD-1 ligands and their induction by JAK2, defining the PD-1 pathway and JAK2 as complementary rational therapeutic targets (Green et al. Blood. 2010).
A phase I dose-escalation and expansion cohorts study of PD-1 blockade with nivolumab has been carried out in adult patients with Relapsed/Refractory (R/R) HL. Overall, 22/23 (96%) patients experienced an Adverse Events (AEs) of any grade, and 12 patients (52%) experienced grade 3–4 AEs. Drug-related AEs occurred in 18 (78%) of patients and the most common were rash (22%) and decreased platelet count (17%). Response rate was 87% (95% CI, 66–97), with a Complete Response (CR) achieved in 4 patients (17%), a Partial Response (PR) in 16 patients (70%), and Stable Disease (SD) in 3 patients (13%). The rate of PFS at 24 weeks was 86% (95% CI, 62–95) and median OS was not yet reached. Therefore, nivolumab-mediated PD-1 blockade was shown to be highly effective in patients with HL (Ansell et al. NEJM. 2015).
Conclusion
Lenz concluded this part of the Education session by explaining that the composition of the microenvironment varies substantially between different subtypes of Lymphoma. Various factors of the microenvironment influence patient survival. There is a need for functional models in order to determine why the microenvironment influences patient survival. Additionally, targeting specific components of the microenvironment represents a promising therapeutic approach and combined regimens that target oncogenic mechanisms in malignant cells as well as interactions in the tumor microenvironment may prove synergistic.
Immune checkpoint inhibitors
Anas Younes, MD, from the Memorial Sloan Kettering Cancer Center, New York, US, gave the second talk during this education session.
Hodgkin Lymphoma (HL)
He began with a summary of phase I and II studies of PD-1 blocking antibodies in relapsed HL, which has found that these agents have high single-agent activity:
|
Drug |
Phase |
Dose/schedule |
N |
% ORR |
% CR |
ORR in BV treated HL |
Ref |
|
Pembrolizumab (humanized IgG4) |
I |
10mg/kg IV Q 2 wks |
29 |
66% |
21% |
66% (n=19) |
Armand et al. JCO. 2016 |
|
Pembrolizumab (humanized IgG4) |
II |
200mg IV Q 3 wks |
60 |
67% |
21% |
- |
Moskowitz et al. ASH. 2016 |
|
Nivlolumab (Fully humanized IgG4) |
I |
3mg/kg IV Q 2 wks |
23 |
87% |
17% |
70% (n=16) |
Ansell et al. NEJM. 2015 |
|
Nivlolumab (Fully humanized IgG4) |
II |
3mg/kg IV Q 2 wks |
63 |
68% |
22% |
- |
Timmerman et al. ASH. 2016 |
Younes first looked at nivolumab in detail, which was approved by the U.S. Food and Drug Administration in May last year for patients with relapsed HL, by discussing final results after extended follow-up of the phase II CheckMate 205 trial (NCT02181738).
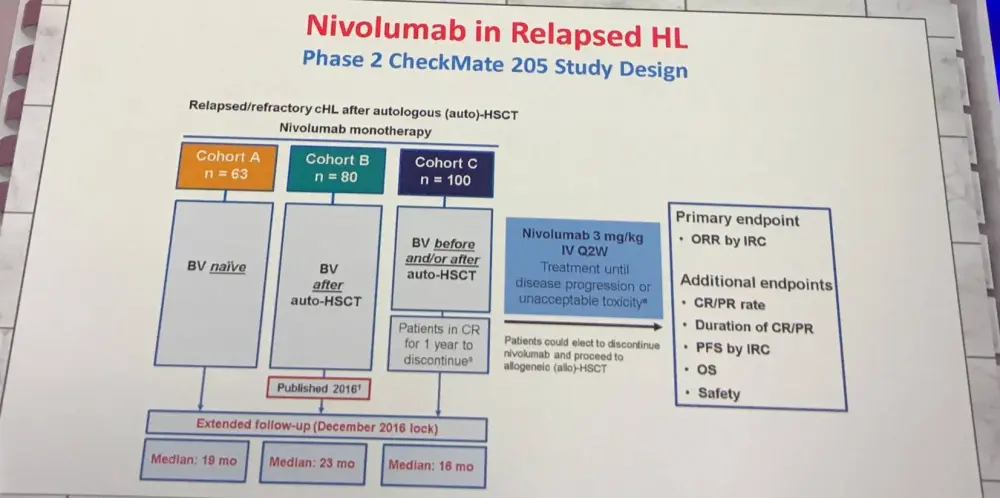
The trial included adult patients with recurrent cHL who had failed to respond to Autologous Stem Cell Transplant (ASCT) and had either relapsed or failed to respond to brentuximab vedotin (BV). Overall, 80 patients were enrolled from 34 different centers and were treated with IV nivolumab at a dose of 3mg/kg every 2 weeks until progression, death, unacceptable toxicity, or withdrawal from study. After a median follow-up of 8.9 months (range, 1.8–11.7), 53/80 (66.3%; 95% CI, 54.8–76.4) patients achieved an Independent Radiologic Review Committee (IRRC)-assessed objective response. All but one responder had a reduction of ≥50% from baseline in tumor burden. Median PFS was 10.0months (95% CI, 8.41–NA) and PFS rate at 6 months was 76.9% (95% CI, 65.0–85.0%). Median OS was not reached and OS rate at 6 months was 98.7% (95% CI, 91.0–100%). The most common drug-related grade 3–4 AEs were neutropenia (5% patients) and increased lipase concentrations (5%). The most common Serious Adverse Event (SAE) of any grade was pyrexia (4%). Three patients died during the study; none of these deaths were attributed to treatment (Younes et al. Lancet Oncol. 2016). Full results after extended follow-up of the CheckMate 205 trial were presented at ICML 2017:
|
|
BV naïve (Cohort A; n=63) |
BV after ASCT (Cohort B; n=80) |
BV before and/or after ASCT (Cohort C; n=100) |
Overall (n=243) |
|
|---|---|---|---|---|---|
|
Objective response per IRC, % (95% CI) |
65 (52–77) |
68 (56–78) |
73 (63–81) |
69 (63–75) |
|
|
Best overall response per IRC, % |
CR |
29 |
13 |
12 |
16 |
|
PR |
37 |
55 |
61 |
53 |
|
|
SD |
24 |
21 |
15 |
19 |
|
|
PD |
11 |
8 |
10 |
9 |
|
|
Unable to determine |
0 |
4 |
2 |
2 |
|
Per investigator assessment, one-third of patients achieved CR and 39% achieved PR. In post-hoc analyses, responses were similar regardless of BV treatment sequence. Median PFS for all 243 patients was 15 months (11–19). In those that achieved CR, PR, and SD it was 22 months, 15 months, and 11 months, respectively (Fanale et al. Hematol Oncol. 2017).
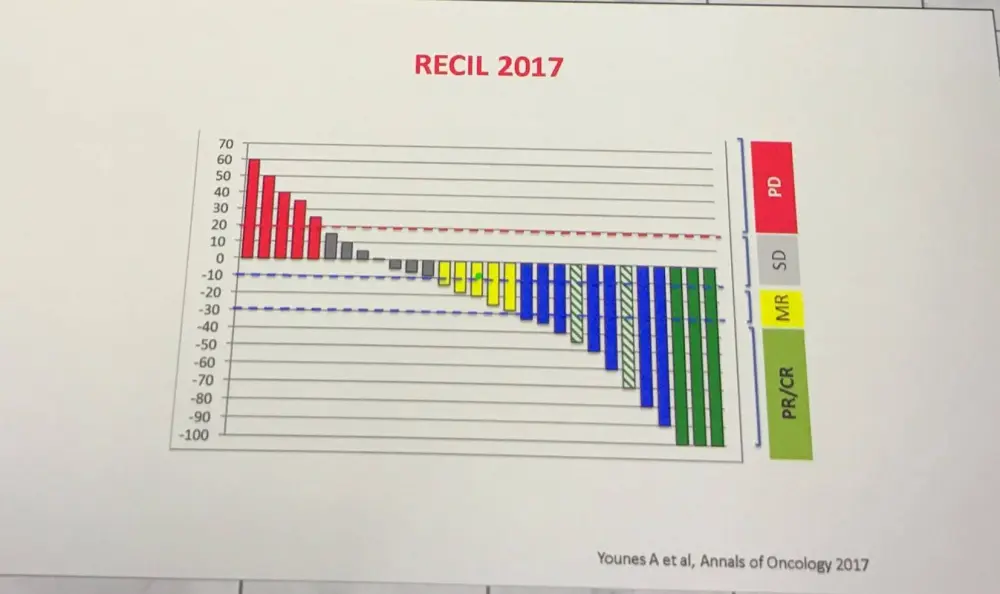
After this, Younes very briefly covered the International Working Group consensus response evaluation criteria in Lymphoma (RECIL 2017), which found with the exception of a CR, the depth of response has no impact on PFS. A new category of response has been defined, termed “Minor Response”.
Following on from this, the potential of combining nivolumab (240mg) with BV (1.8mg/kg) for patients with R/R HL has been explored in a phase I/II trial; interim results of which were presented at ICML 2017. In patients who responded (PR/CR), stem cell collection occurred with BEAM ASCT consolidation. Non-responders, received chemotherapy salvage before undergoing stem cell collection occurred with BEAM ASCT consolidation. Overall objective response rate was 85% with a CR rate of 63% and a PR rate of 22%.
The talk then moved on from nivolumab to focus on pembrolizumab in more detail. The KEYNOTE-087 single-arm, phase II study of pembrolizumab included 120 R/R HL patients in three cohorts. Patients received 200mg of pembrolizumab once every 3 weeks. At the time of analysis, patients received a median of 13 treatment cycles. Response by blinded independent central review is presented in the table below:
|
|
Post-ASCT and BV (Cohort 1; n=69) |
Post-chemo and BV but not eligible for ASCT (Cohort 2; n=81) |
Post-ASCT but no BV (Cohort 3; n=60) |
|---|---|---|---|
|
ORR, % (95% CI) |
72.5 (60.4–82.5) |
65.4 (54.0–75.7) |
66.7 (53.3–78.3) |
|
CR, % (95% CI) |
21.7 (12.7–33.3) |
22.2 (13.7–32.8) |
21.7 (12.1–34.2) |
|
PR, % (95% CI) |
50.7 (38.4–63.0) |
43.2 (32.2–54.7) |
45.0 (32.1–58.4) |
|
SD, % (95% CI) |
18.8 (10.4–30.1) |
11.1 (5.2–20.0) |
21.7 (12.1–34.2) |
|
PD, % (95% CI) |
4.3 (0.9–12.2) |
21.0 (12.7–31.5) |
11.7 (4.8–22.6) |
|
Unable to determine, % (95% CI) |
4.3 (0.9–12.2) |
2.5 (0.3–8.6) |
0 |
Pembrolizumab was found to achieve high response rates and displayed an acceptable safety profile in patients with R/R HL, and presents as a potential alternative treatment option for the disease (Chen et al. JCO. 2017).
In March of this year, pembrolizumab was approved by the U.S. FDA for the treatment of adult and pediatric patients with refractory cHL, or those who have relapsed after ≥3 previous lines of therapy; read more here.
Following this, Younes covered other agents for the treatment of HL, first focusing on PD-L1 specific agents, such as avelumab. This agent has achieved a best Overall Response Rate (ORR) of 20.0% in post-ASCT patients and 62.5% in post-allogeneic SCT (allo-SCT) patients.
Histone Deacetylase (HDAC) inhibitors have also been explored. In a phase II trial, panobinostat resulted in 71% of relapsed HL patients experiencing tumor reduction (Younes et al. JCO. 2012). Panobinostat has been found to downregulate PD-1 on T-cells of patients with relapsed HL in vitro (Oki et al. Blood Cancer J. 2014).
Entinostat, a synthetic benzamide derivative that binds and inhibits HDAC, was assessed for the treatment of R/R HL in the ENGAGE-501 phase II study (NCT00866333). Overall, 49 patients were enrolled: 33 were assigned to Schedule A (10 or 15 mg oral entinostat once every other week) and 16 patients to Schedule B (15 mg oral entinostat once weekly in 3 of 4 weeks). The median number of previous therapies patients had received was 3 (range, 1–10), with 80% of the patients receiving a previous SCT and 8% of patients receiving prior BV. ORR was 12% while the disease control rate (CR, PR, and SD beyond 6 months) was 24%. Tumor reduction was reported for 58% of evaluable patients. Median PFS was 5.5 months and OS was 25.1 months. Further investigation is required in order to identify predictive biomarkers for treatment response and to develop mechanism-based combination strategies (Batlevi et al. Haematologica. 2017).
Follicular Lymphoma (FL) and DLBCL
Younes then briefly focused on immunotherapy for Non-Hodgkin Lymphoma, starting with a phase Ib study of atezolizumab, a fully humanized monoclonal IgG1 antibody against PD-L1, and obinutuzumab in patients with R/R FL or DLBCL. In patients with FL, 14/23 (61%) achieved a response (PET-CT) at or prior to the end of induction response assessment, as measured by the investigator. Among the 14 responders, a median Duration of Response (DoR) of 15.0 months was reported, with 10 patients still in response at data cut-off. In patients with DLBCL, 4 achieved a response and median DoR was 4.9 months, with 1 patient still in response (Palomba et al. Hematol Oncol. 2017).
Pembrolizumab combined with rituximab has also been investigated in patients with relapsed FL in a phase II, open-label study. Interim results were presented during ICML 2017 (abstract #109) by Loretta J. Nastoupil, MD, from the University of Texas MD Anderson Cancer Center, Houston, TX, US; read more here. ORR was 65% and CR rate was 50%.
Conclusion
Younes concluded his portion of the session by stating that antibodies targeting PD-1 have shown substantial clinical activity in HL, resulting in regulatory approval. Preliminary data indicates that targeting PD-L1 in HL is also a feasible strategy and furthermore PD-L2 may not play a key role in suppressing T-cell function. In FL and DLBCL, targeting PD-1 and PD-L1 has shown modest activity.
Is transplantation in Lymphoma still needed in the era of immunotherapy?
The last presentation in this session was given by A. Sureda from Institut Català d'Oncologia, Hospital Duran i Reynals, Barcelona, Spain.
The use of Hematopoietic SCT (HSCT) for Lymphomas is rising, despite the fact that more effective first-line therapies are available. There have been no prospective trials in any histology in recent years and so clinical practice is based on “old trials”.
Between January 1996 and November 2005, a total of 2,200 patients aged 18 years or older with HL were reported to the EBMT registry as having disease relapse/progression after a first ASCT. Of these, 511 from the EBMT-GITMO databases were reviewed. Treatments administered following ASCT failure included conventional chemotherapy and/or radiotherapy in nearly two-thirds (294) of patients, second ASCT in 8% (35 patients), and allo-SCT in 29% (133 patients). After a median follow-up of 50 months (75% of cases was longer than 34 months), OS at 3 and 5 years was 39.5% (95% CI, 35–44) and 29.7% (95% CI, 25–34). Independent risk factors for OS were early relapse (<6 months) after ASCT, stage IV disease, bulky disease, poor performance status, and age ≥50 years at relapse. For patients with no risk factors, 5-year OS was 62% versus 37% for those having 1 risk factor and 12% for those with ≥2 factors (Martínez et al. Ann of Oncol. 2013).
The phase II HDR-ALLO study was also covered; a prospective clinical trial by GELTAMO and the Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. Ninety-two relapsed HL patients with a HLA-identical sibling, a matched unrelated donor, or a one antigen mismatched, unrelated donor were treated with salvage chemotherapy followed by reduced intensity allo-SCT. Refractory disease was observed in 14 patients and died from PD with a median OS after trial entry of 10 months (range, 6–17). Overall, 78 patients proceeded to allo-SCT (unrelated donors, n=23). Fifty were allografted in CR or PR and 28 in SD. Fludarabine (150mg/m2 IV) and melphalan (140mg/m2 IV) were used as the conditioning regimen. The Non-Relapse Mortality (NRM) rate was 8% at 100 days and 15% at 1 year. Relapse was the major cause of failure. PFS rate was 47% and 18% at 1 year and 4 years from trial entry, respectively. For allografted patients, PFS rate was 48% and 24% at 1 year and 4 years, respectively. Chronic Graft-versus-Host Disease (GvHD) was associated with a lower incidence of relapse. Patients allografted in CR had a significantly better outcome. The OS rate was 71% at 1 year and 43% at 4 years (Sureda et al. Haematologica. 2012).
Unmanipulated Haploidentical (HAPLO) related donor transplant with Reduced Intensity Conditioning (RIC) Post-Transplant Cyclophosphamide (PT-Cy) as GvHD prophylaxis has become a promising rescue strategy for R/R HL. In a multicenter experience using an IV busulfan-based HAPLO-RIC regimen and PT-Cy in 43 advanced HL patients with advanced HL, engraftment occurred in 42 patients (97.5%), with a median time to neutrophil recovery of 18 days and platelet recovery of 26 days. Cumulative incidences of grade 2–4 acute GvHD and chronic GvHD were 39% and 19%, respectively. With a median follow-up of 25.5 months for survivors, 27 patients are alive and 22 were disease free. Cumulative incidences of 1-year NRM and relapse at 2 years were 21% and 24%, respectively. The estimated 2-year Event-Free Survival (EFS) and OS were 48% and 58%, respectively. CR prior to HAPLO-RIC correlated with better EFS (78.5% vs 33.5%; P = 0.015) and OS (86% vs 46%; P = 0.044). These results provide further confirmation of the use of HAPLO-RIC in advanced HL by means of an IV busulfan-based conditioning regimen (Gayoso et al. BMT. 2016).
A phase II study of BV in R/R HL patients after ASCT (n=102) was also discussed (NCT00848926). After a median observation period of around 3 years, median OS was 40.5 months and median PFS was 9.3 months. Improved outcomes were reported observed in patients who achieved CR on BV, with estimated 3-year OS of 73% (95% CI, 57–88%) and PFS of 58% (95% CI, 41–76%) in this group (medians not reached). Moreover, 16/34 (47%) patients who achieved CR, remain progression-free after a median of 53.3 months (range, 29.0–56.2) of observation. Also, 12 of these remain progression-free without consolidative allo-SCT. Patients with younger age, good performance status, and lower disease burden at baseline were more likely to achieve CR; these were favorable prognostic factors for OS. These results indicate that a substantial number of patients who respond to BV can achieve prolonged disease control (Gopal et al. Blood. 2015).
Sureda moved on to discuss checkpoint inhibitors pre-allo-SCT in patients with Lymphoma. In an international retrospective analysis of 39 patients with Lymphoma who received prior PD-1 inhibitor therapy at a median time of 62 days (range, 7–260) before HSCT, median follow-up was 12 months and the 1-year cumulative incidences of grade 2–4 and grade 3–4 acute GvHD were 44% and 23%, respectively. The 1-year incidence of chronic GvHD was 41%. Four treatment-related deaths were reported (hepatic sinusoidal obstruction syndrome n=1; early acute GvHD n=3). Moreover, noninfectious febrile syndrome developed in 7 patients shortly after transplant that needed prolonged courses of steroids. 1-year OS was 89% (95% CI, 74–96) and PFS was 76% (95% CI, 56–87). 1-year cumulative incidences of relapse mortality and NRM were 14% (95% CI, 4–29) and 11% (95% CI, 3–23), respectively. In 17 patients, circulating lymphocyte subsets were analyzed; compared with controls, patients who had received prior PD-1 blockade had significantly decreased PD-1+ T-cells and decreased ratios of T-regulatory cells to conventional CD4 and CD8 T-cells. This data suggests that PD-1 blockade followed by HSCT resulted in low rates of relapse. Although, there appeared to be a higher risk of early immune toxicity, potentially due to the long-lasting immune alterations resulting from previous PD-1 blockade (Merryman et al. Blood. 2017).
Allo-SCT in nivolumab studies was also looked at:
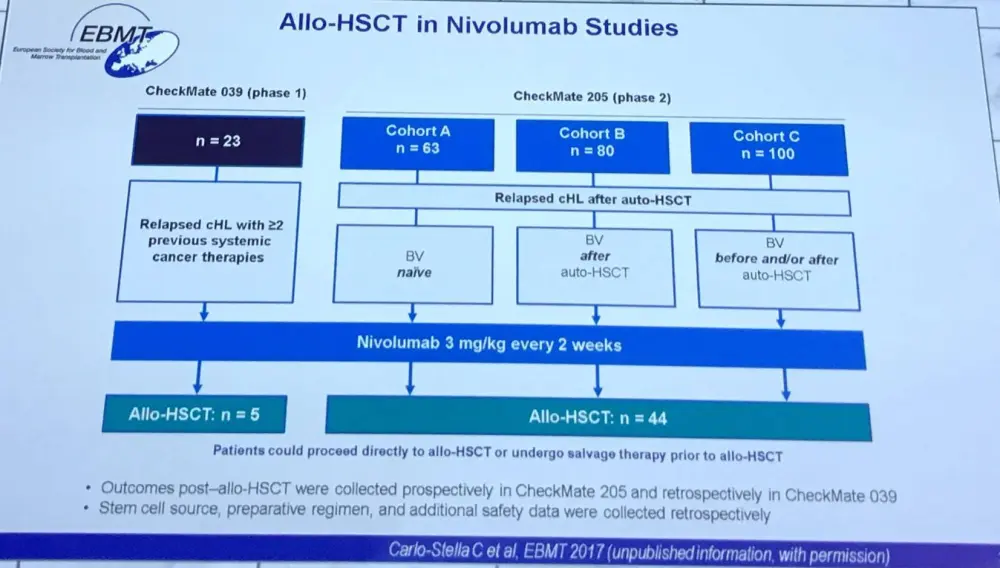
Median time from last nivolumab dose to allo-SCT was 1.5 months (range, 0.4–13.5). Disease status at allo-SCT was not collected in the CheckMate 039 study; in the CheckMate 205 study, 48% of patients were in CR, 43% were in PR, and 9% were NA/unable to determine. Treatment-Related Mortality (TRM) at 6 months was 16% (95% CI, 7–29). Post-allo-SCT disease progression occurred in 3 of 49 patients. At 6 months, the incidence of grade 2–4 acute GvHD was 36% (95% CI, 22–50) and the incidence of grade 3–4 acute GvHD was 25% (95% CI, 12–59). Median time from allo-SCT to grade 2–4 and grade 3–4 acute GvHD was 24 days (range, 1–304). No clear relationship could be established between estimated nivolumab concentrations at allo-SCT and TRM or grade 3–4 GvHD. Median OS was not reached after median follow-up of 5.6 months (range, 0–19) from all-SCT.
Sureda next discussed the use of nivolumab after allo-HCT referring to a retrospective analysis of 20 patients with R/R HL published by Herbaux et al. in Blood earlier this year, which the LH has previously reported on; read more here. Overall, the efficacy of nivolumab was confirmed in patients with R/R HL after allo-SCT. Moreover, nivolumab following allo-HCT displayed a manageable safety profile but required close clinical assessment.
Furthermore, a multicenter retrospective analysis has been carried out on 31 Lymphoma patients receiving anti-PD-1 monoclonal antibodies for relapse post allo-HCT. Of these, 29 (94%) patients had cHL and 27 had one or more salvage therapies post allo-HCT and prior to anti-PD-1. Median follow-up after the first dose of anti-PD-1 was 428 days (range, 133–833). In 30 evaluable patients, ORR was 77% (15 CRs and 8 PRs). At last follow-up, progression had occurred in 11/31 patients and 21/31 (68%) remain alive; 8 (26%) deaths were related to new onset GvHD after anti-PD-1. Treatment-emergent GvHD after initiation of anti-PD-1 therapy was reported in 17 (55%) patients (6 acute, 4 overlap, and 7 chronic). GvHD severity was grade III–IV acute or severe chronic in 9 patients. Only 2/17 patients achieved CR to GvHD therapy and 14/17 required two or more systemic therapies. Overall, PD-1 blockade in relapsed cHL allo-HCT patients demonstrated high efficacy but was often complicated by rapid onset of severe and treatment refractory GvHD (Haverkos et al. Blood. 2017).
In conclusion, Sureda stated that Lymphomas are the second most common indication for ASCT and numbers are continually increasing. Thus far, there have been no significant changes to this with the introduction of immunotherapy. Research has found that checkpoint inhibitors have high efficacy and a tolerable safety profile in patients with R/R HL. Moreover, they can be employed as a “bridge” to allo-SCT and be used to treat patients who experience relapse post-allo-SCT. Currently, the use of checkpoint inhibitors does not seem to increase or alter the toxicities associated with allo-HCT; however, a high incidence of GvHD was found.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?