All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Johnson & Johnson, Roche and sobi, and supported through educational grants from Bristol Myers Squibb, Incyte and Lilly. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
EHA-SWG 2017 | Rare Lymphomas: Burkitt Lymphoma
On March 10–12 2017, the EHA-SWG meeting on Rare Lymphomas took place in Barcelona, Spain, and was jointly chaired by Prof. Martin Dreyling, from Klinikum der Universität München, Germany, and Prof. Marie-José Kersten, from the Academic Medical Center, Amsterdam, The Netherlands.
On March 11th 2017, M. Chamuleau, from the VU University Medical Center, Amsterdam, The Netherlands, gave a talk on Burkitt Lymphoma (BL) during the “MYC-driven lymphomas” scientific session.
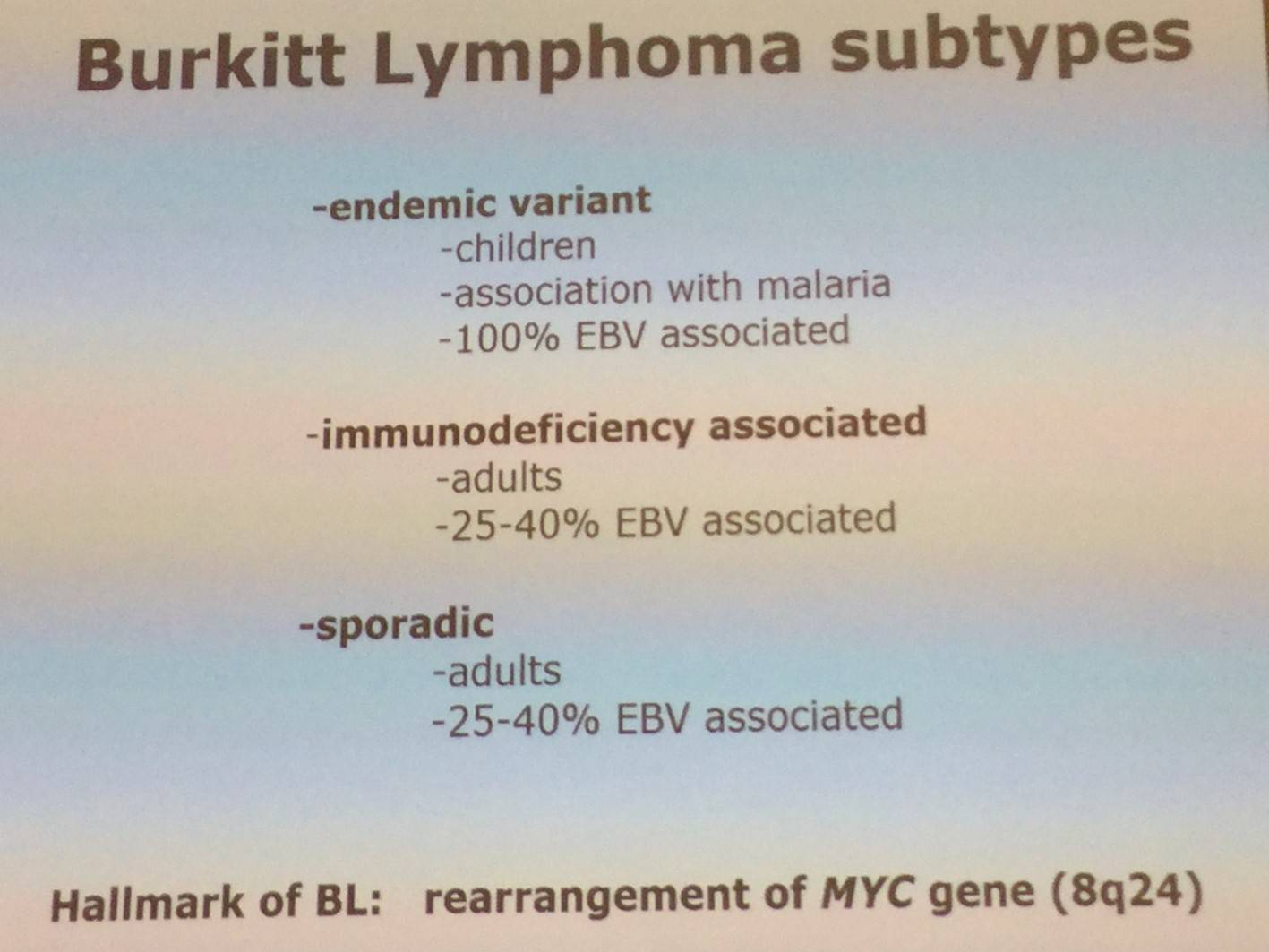
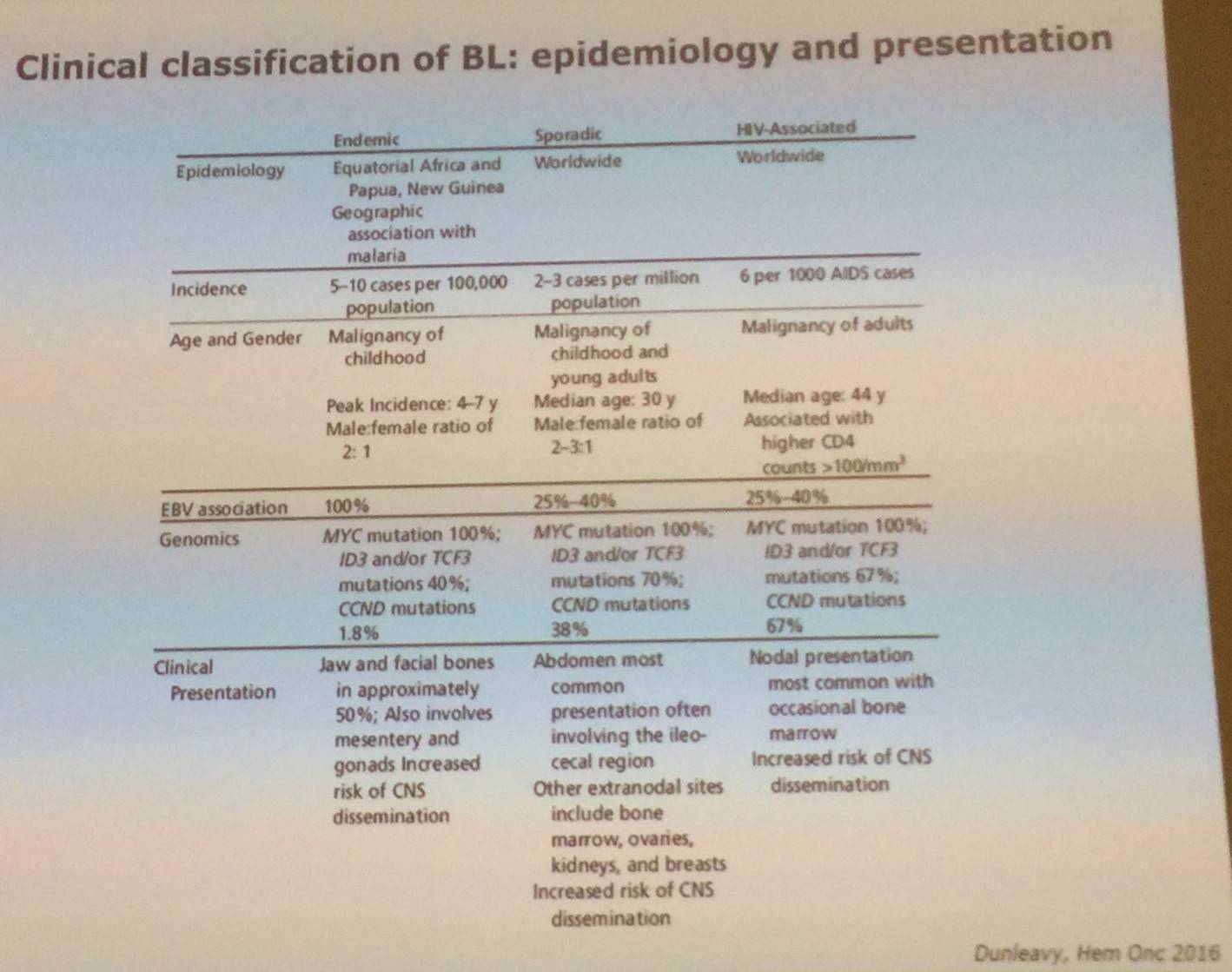
The talk began by explaining that BL is highly aggressive and estimated to account for 1–2% of all NHLs in adults. Incidence is 0.15–0.2 per 100,000 equating to 1,100–1,400 new patients in Europe. The distribution of BL when regarding age is bimodal; an early peak is observed among those aged 0–15 years and a later peak in those 60+ years of age. BL was the first tumor to be associated with a virus (EBV), resulted in the first description of an oncogeneic translocation [t(8;14),MYC], and was the first lymphoma associated with immune deficiency (HIV). BL subtypes were then shared:
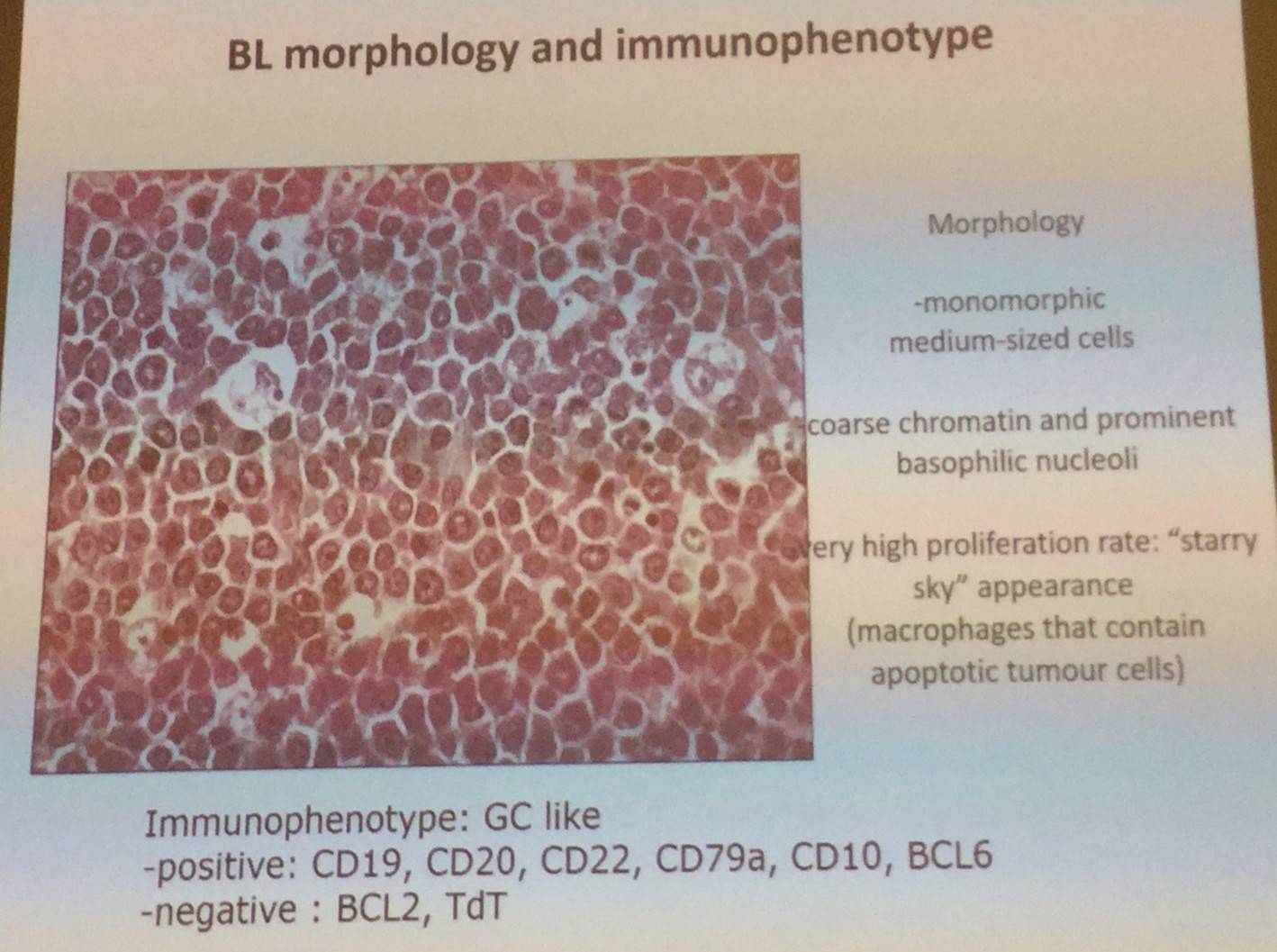
The morphology and immunophenotype of BL were then discussed:
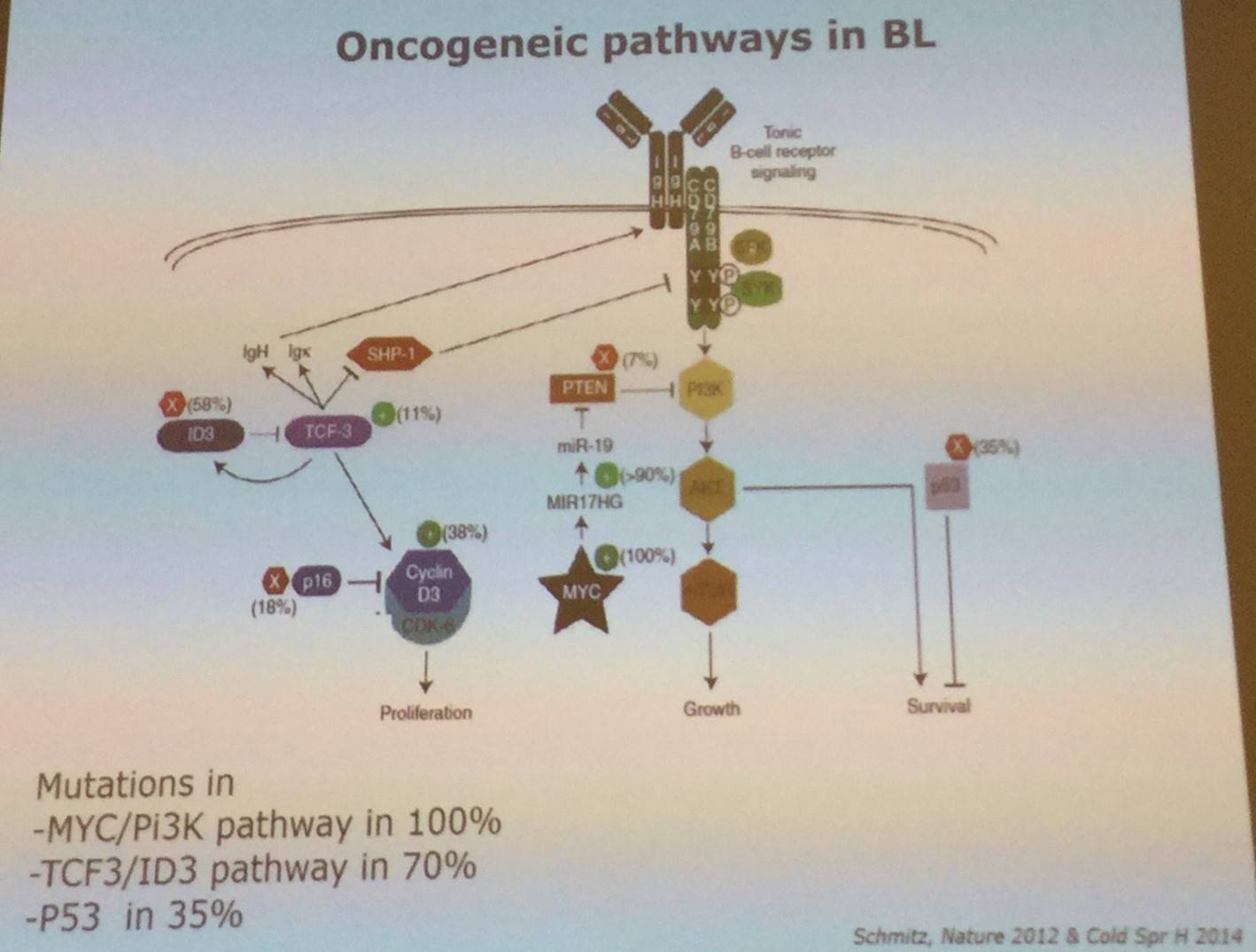
Overexpression of MYC is a hallmark of BL, and is due to a translocation between the MYC/8q24 locus which results in it coming under control of the enhance of the heavy or light immunoglobulin chain, most commonly IgH, [t(8;14)(q24;q32)]. Other common mutations were also presented:
Molecular diagnosis of BL was also covered in the talk; BL is identified by high expression of GCB and MYC related genes, as well as low expression of NFkB and MHC class I related genes.
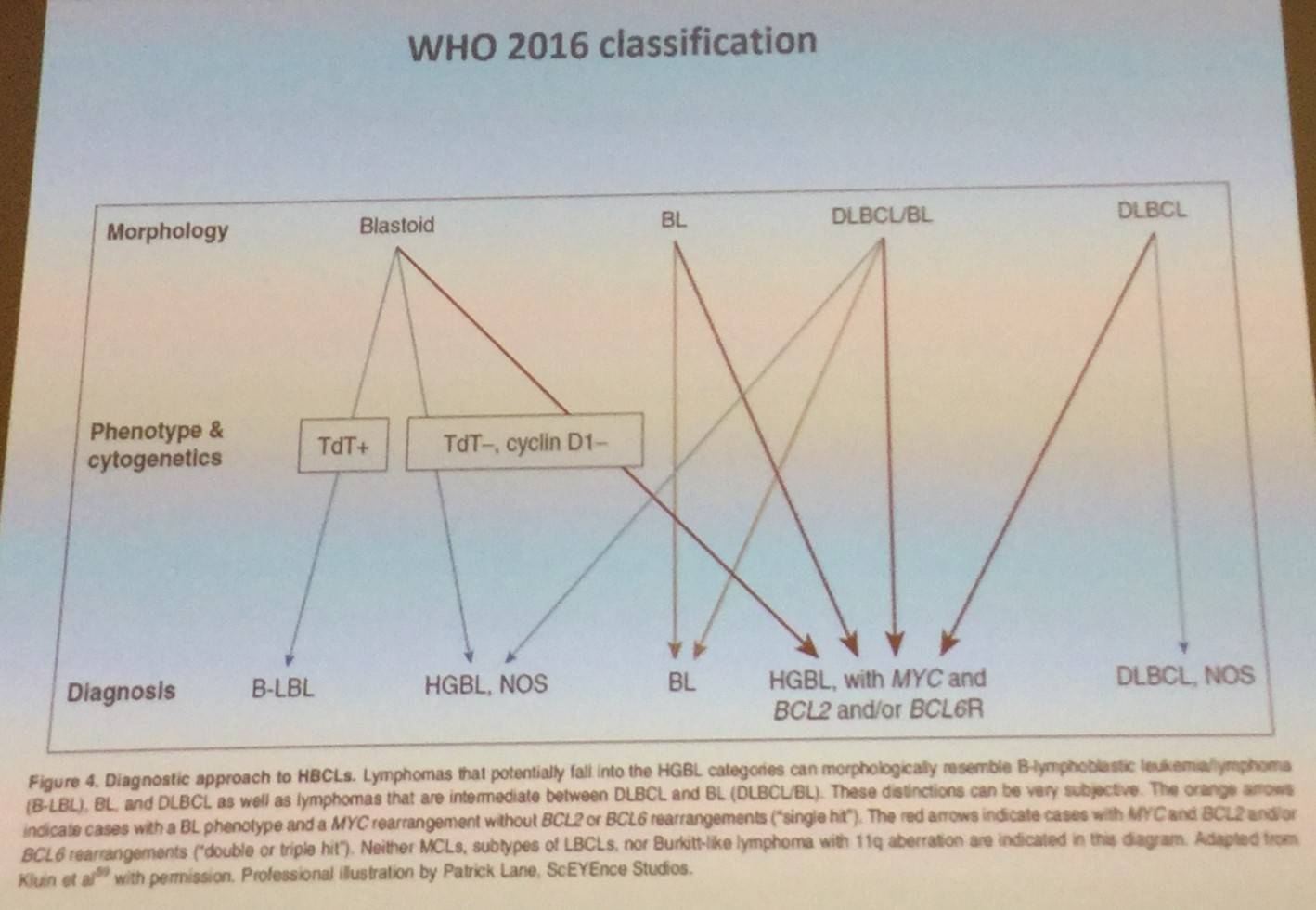
In the WHO classification of 2016, the definition of BL has been further refined by knowledge acquired by next generation sequencing and gene expression profiling.
The talk then discussed BL etiology, which has not yet been entirely unravelled. In HIV associated BL it is though the first hit is HIV infections leading to B-cell activation, aberrant induction of AID which results in MYC translocation. The second hit is EBV which “immortalizes” B-cells. In the endemic variant of BL, the first hit is thought to be EBV infection, and the second hit is Pf infection which results in EBV release and reactivation as plasmodium induces AID and MYC translocation.
The epidemiology and presentation of endemic, sporadic, and HIV-associated BLs were also shared:
Following this, M. Chamuleau discussed the work-up for BL:
- Adequate sample at diagnosis for morphology, phenotype and FISH analysis
- Staging: BM biopsy, liquor analysis, PET-CT scan at diagnosis and end-of-treatment, potentially CT mid-treatment, and no scans in follow-up
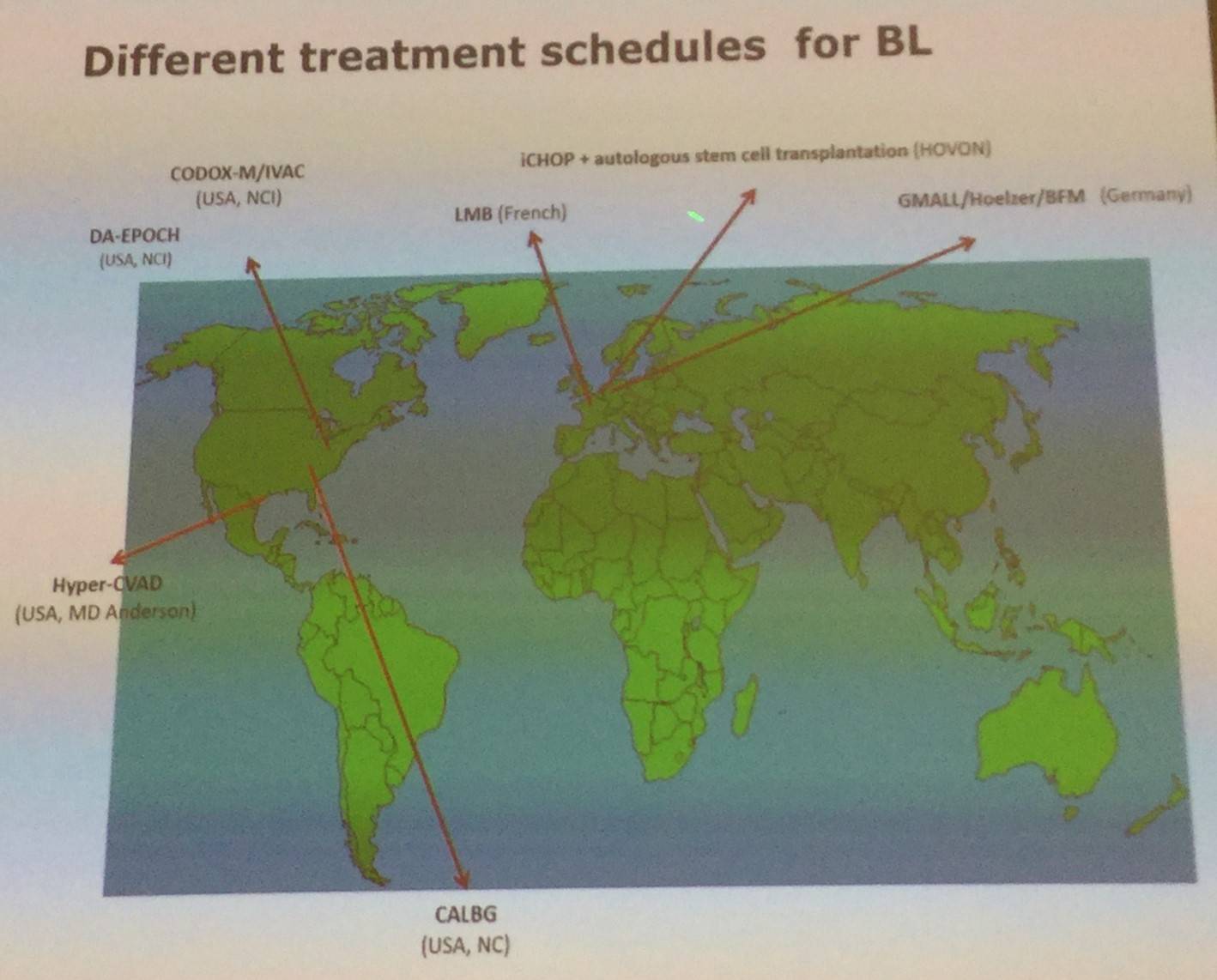
In terms of therapy for BL, prompt aggressive treatment with high dose intensive chemotherapy schemes and adequate supportive care results in OS rates for BL patients of 70% at 5 years. It has been found that results with CHOP are inadequate, and rituximab should be added.
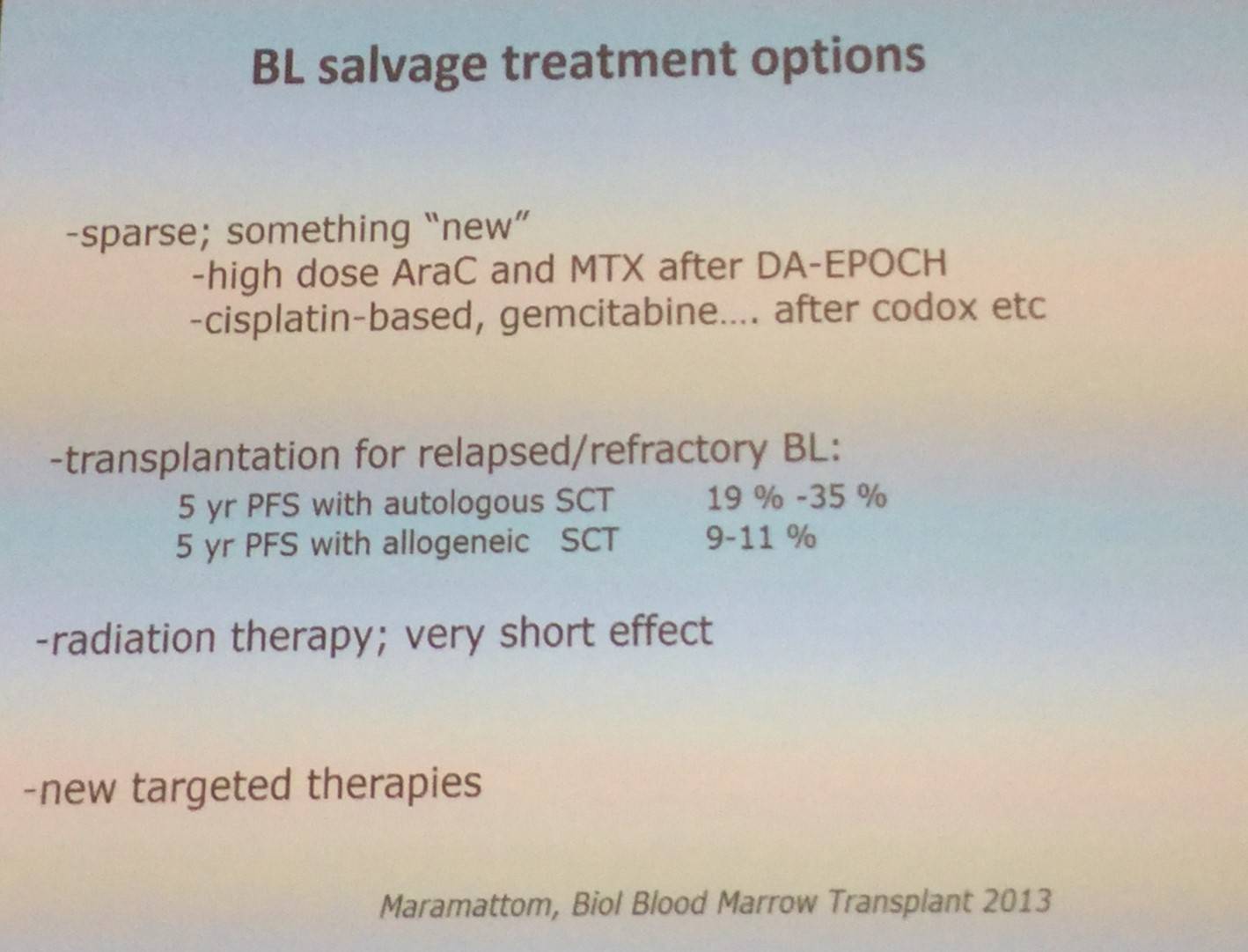
However, primary refractory disease and relapsed disease are chemotherapy resistant and outcome of patients is dismal, and there are few salvage treatment options available.
New targeted therapies are entering the clinic for BL, including SYK kinase inhibitors (e.g. dasatinib, fostamatinib), PI3K inhibitors, and BET bromodomain inhibitors (e.g. JQ-1).
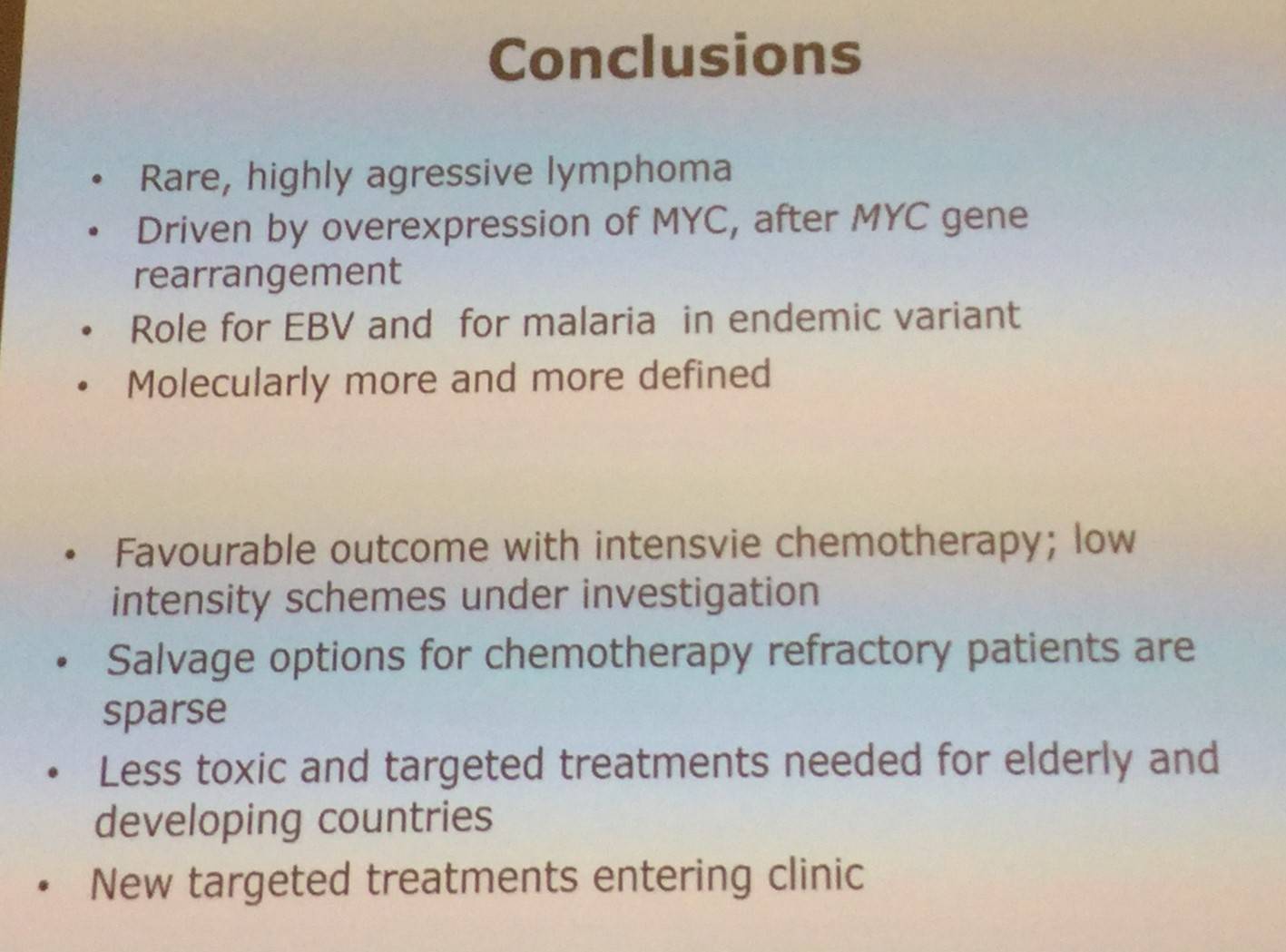
M. Chamuleau concluded the talk with a succinct summary slide:
References
Your opinion matters
In your experience, when do most CRS/ICANS events occur after lisocabtagene maraleucel infusion?