All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Caribou Biosciences, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
Factors associated with long-term outcomes of CD19 CAR T-cell therapy for R/R CLL
While CD19-targeted chimeric antigen receptor (CAR)-modified T-cell therapy has shown high response rates in patients with relapsed/refractory (R/R) chronic lymphocytic leukemia (CLL), there is limited research on the factors associated with duration of response (DOR).
The Lymphoma Hub has previously reported on a phase I/II clinical trial (NCT01865617) demonstrating high rates of durable responses with CD19 CAR T-cell therapy combined with ibrutinib. Below, we summarize a recent publication by Liang et al. published in Blood Advances that provides an update on this phase I/II clinical trial, including >6 years of median follow-up.
Study design1
Patients with R/R CLL and/or Richter transformation were enrolled and received either JCAR014 without concurrent ibrutinib (n = 30) or with concurrent ibrutinib (n = 19).
Patients received sequential or concurrent LD chemotherapy with cyclophosphamide (Cy) and fludarabine (Flu), Cy alone, or Flu alone. Following LD chemotherapy, an infusion of 2 × 105, 2 × 106, or 2 × 107 CD19 CAR T cells per kilogram of body mass was given. In the concurrent ibrutinib cohort, patients received ibrutinib (420 mg, daily) starting ≥2 weeks before leukapheresis up to ≥3 months after CAR T-cell infusion.
Results1
Overall, 49 patients were enrolled with a median age of 61 years, and most patients had intolerance to, and/or progression on, ibrutinib (Table 1).
Table 1. Key baseline characteristics*
|
BM, bone marrow; CLL, chronic lymphocytic leukemia; CAR, chimeric antigen receptor; Cy, cyclophosphamide; ECOG PS, Eastern Cooperative Oncology Group Performance Status; Flu, fludarabine; IHC, immunohistochemistry; LD, lymphodepletion; MFC, multiparameter flow cytometry; WBC, white blood cell. |
|
|
Characteristic, % (unless otherwise specified) |
N = 49 |
|---|---|
|
Median age, years |
61.0 |
|
Sex |
|
|
Female |
33.0 |
|
Male |
67.0 |
|
ECOG PS score |
|
|
0 |
49.0 |
|
1 |
51.0 |
|
Prior history of or current Richter transformation |
18.0 |
|
Median number of prior therapies |
5.0 |
|
Prior fludarabine |
29.0 |
|
Prior bendamustine |
51.0 |
|
Prior venetoclax |
39.0 |
|
High-risk cytogenetics† |
94.0 |
|
Intolerance to and/or progression on ibrutinib |
96.0 |
|
Median absolute lymphocyte count, 109/L |
1.8 |
|
Median absolute CD4+ T-cell count, cells per μL |
547.3 |
|
Median absolute CD8+ T-cell count, cells per μL |
350.4 |
|
Median CLL cell in the blood by MFC, % of WBCs‡ |
22.3 |
|
Marrow CLL burden |
|
|
Median CLL cells in the BM by IHC§ |
60.0 |
|
Median CLL cells in BM by MFC |
49.4 |
|
Bulky disease| |
27.0 |
|
LD regimen |
|
|
Concurrent Cy/Flu¶ |
55.0 |
|
Sequential Cy/Flu** |
39.0 |
|
Cy 2 g/m2 × 1 day |
2.0 |
|
Flu 25 mg/m2 × 3 days |
4.0 |
|
CAR T-cell dose level |
|
|
2 × 105 cells per kg |
10.0 |
|
2 × 106 cells per kg††,‡‡ |
88.0 |
|
2 × 107 cells per kg |
2.0 |
Long-term outcomes
Overall, 47 patients were evaluable for response (two patients died before response assessment due to Grade 5 cytokine release syndrome and neurotoxicity [n = 1] and presumed ibrutinib-related cardiac arrhythmia [n = 1]).
The median follow-up was 79.6 months, and the median DOR was 18.9 months; the 6-year DOR was 26.4%. The progression-free survival (PFS) and overall survival (OS) rates for all patients who received CAR T-cell therapy are shown in Figure 1.
Figure 1. A Median and B 6-year PFS and OS rates for all patients who received CAR T-cell therapy*
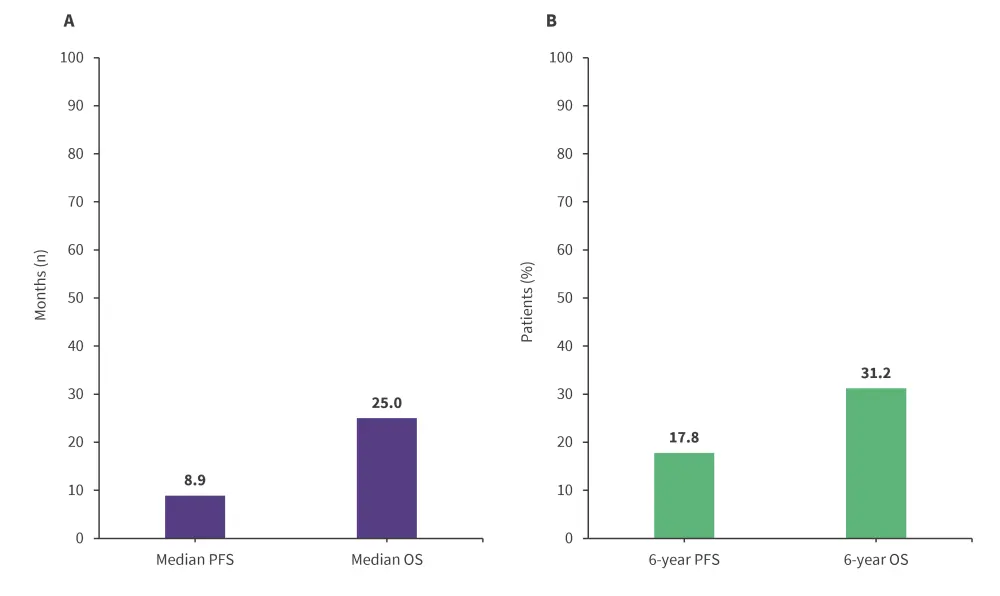
OS, overall survival; PFS, progression-free survival.
*Data from Liang, et al.1
One patient each with current Richter transformation experienced complete response (CR) and CR with incomplete hematologic recovery but relapsed 9.8 and 3.0 months after CAR T-cell infusion, respectively.
Predictors of PFS, DOR, and OS
Univariate Cox regression analyses were carried out to identify predictors of PFS, DOR, and OS (Figure 2).
Figure 1. Predictors of PFS, DOR, and OS*
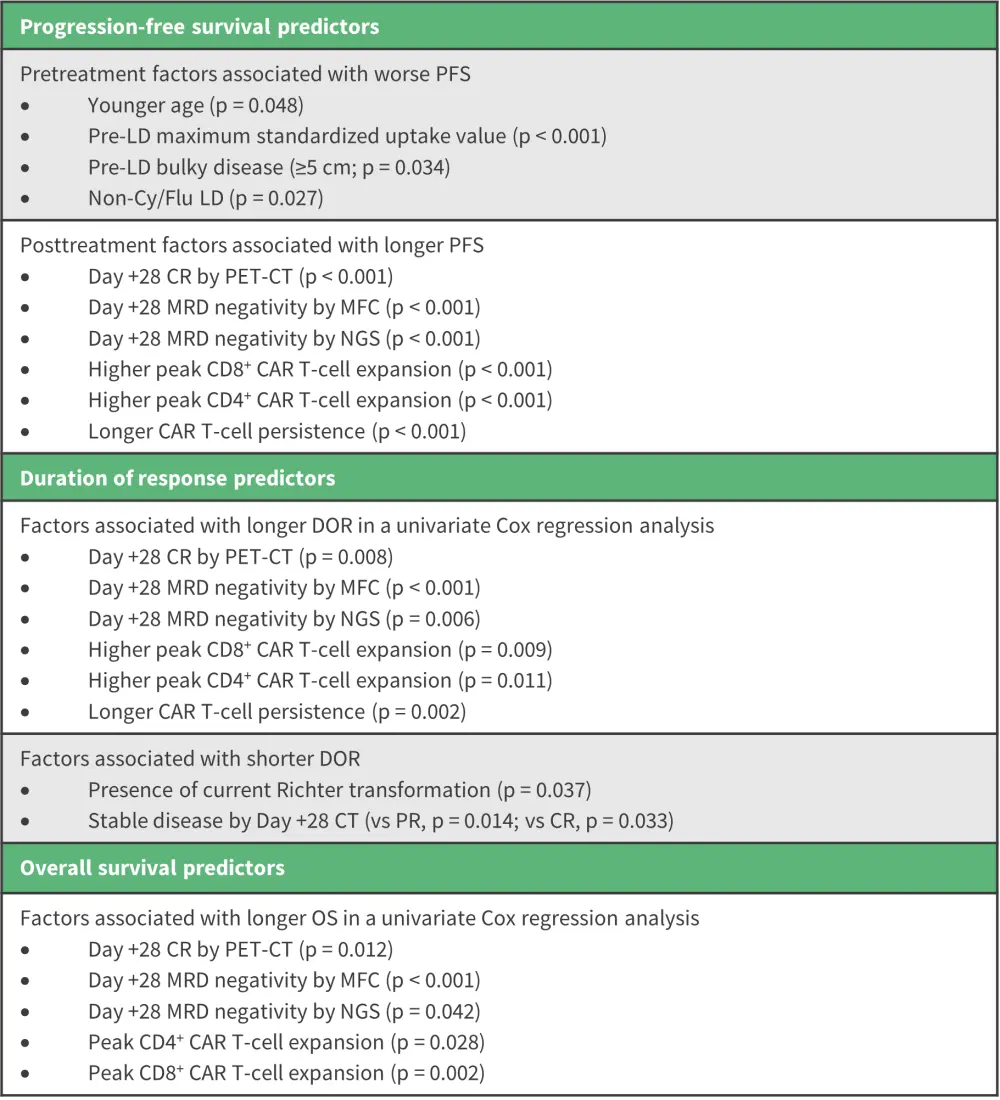
CAR, chimeric antigen receptor; CR, complete response; DOR, duration of response; LD, lymphodepletion; MFC, multiparameter flow cytometry; MRD, measurable residual disease; NGS, next-generation sequencing; OS, overall survival; PET-CT, positron emission tomography-computed tomography; PFS, progression-free survival.
*Data from Liang, et al.1
An association between higher pre-LD, Day +0, and peak serum levels of several cytokines with shorter PFS was observed during an exploratory analysis.
Factors associated with shorter OS included Eastern Cooperative Oncology Group Performance Status of 1, maximum standardized uptake values, and bulky disease.
Conclusion
This 6-year follow-up update demonstrated durable responses in patients with high-risk R/R CLL and MRD-negative response after CD19 CAR T-cell therapy. Predictors of long-term outcomes were also identified, including both pretreatment and posttreatment variables that were strongly associated with PFS. Day +28 CR by positron emission tomography-computed tomography, Day +28 MRD negativity by MFC, Day +28 MRD negativity by next-generation sequencing, higher peak CD8+ CAR T-cell expansion, higher peak CD4+ CAR T-cell expansion, and longer CAR T-cell persistence were associated with longer PFS.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?
