All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
iwCLL 2017 | RESONATE, RESONATE-2, and HELIOS: risk factors linked to poor outcomes with other therapies may be irrelevant when predicting outcomes with ibrutinib
On 14th May 2017, during iwCLL, the fifth session took place titled “Additional Considerations for the Initial Treatment of CLL.” This session was chaired by Richard Furman (Weill Cornell) and Jae Park (Memorial Sloan Kettering Cancer Center).
Thomas J. Kipps, MD, PhD, from the University of California, San Diego, Moores Cancer Center, California, USA, gave a presentation during this session titled “Outcomes of Ibrutinib-Treated Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Leukemia With High-Risk Prognostic Factors in an Integrated Analysis of 3 Randomized Phase 3 Studies.”
Del(17p), del(11q), and unmutated IGHV are prognostic factors for poor outcomes after chemo-immunotherapy for CLL/SLL patients. In the phase II PCYC-1102/1103 study (newly diagnosed = 31; R/R = 101), multivariate analysis identified del(17p) as an independent prognostic impact for worse PFS or OS.
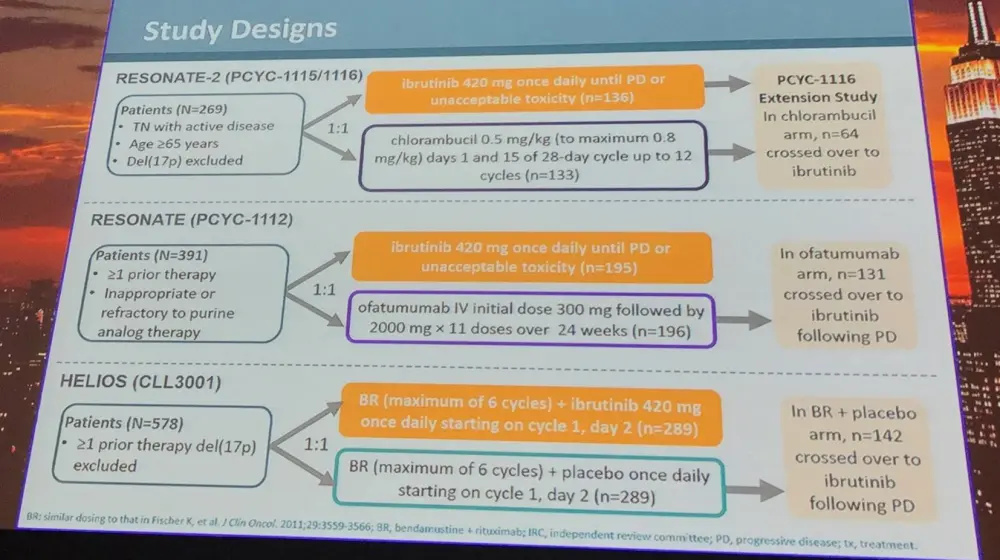
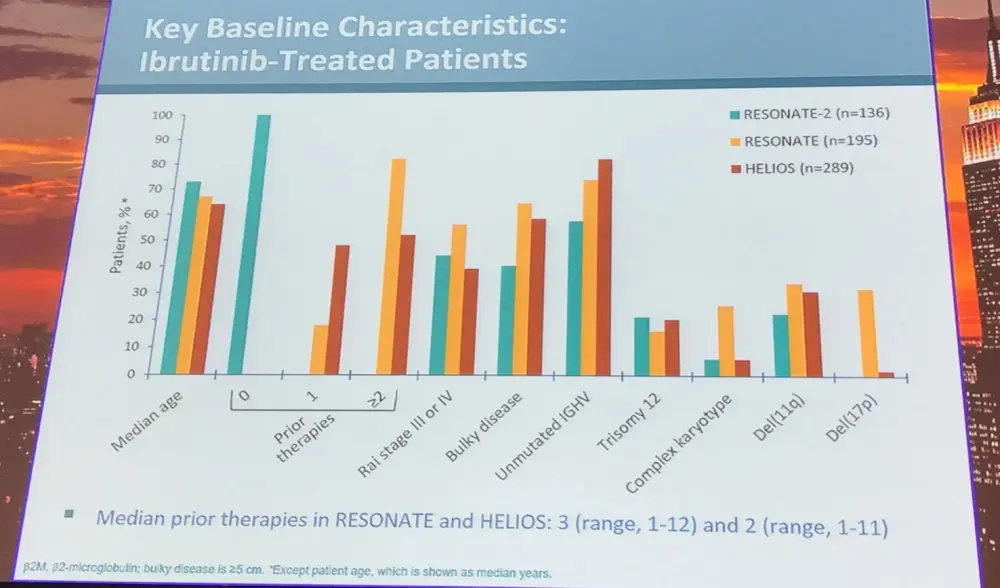
Data from the RESONATE, RESONATE-2, and HELIOS trials were pooled and analyzed based on IGHV mutational status, del(11q), trisomy 12, and complex karyotype. Impact of del(17p) was not assessed for efficacy analyses as patients with this genetic abnormality were excluded from two of the three trials. PFS for comparator patients was also included to provide context. Multivariate analysis was undertaken to determine the risk/prognostic factors associated with PFS.
It was found that, after a median follow-up of 36.4 months (95% CI, 35.8–37.1), PFS at 36 months in ibrutinib-treated patients was 70% for unmutated IGHV compared to 77% for mutated IGHV.
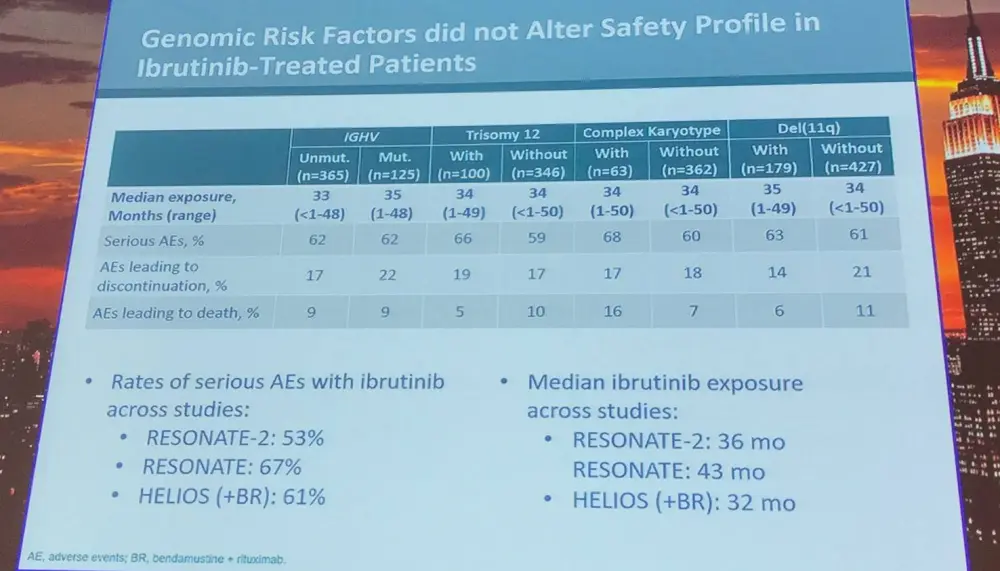
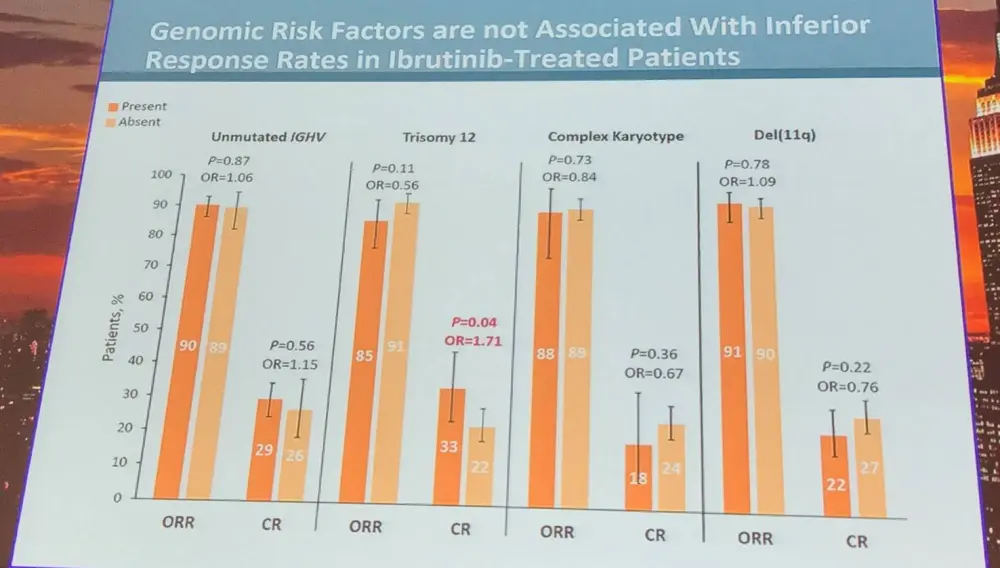
Thomas J. Kipps concluded the talk by stating that ibrutinib-treated patients with trisomy 12 had significantly higher CR rate; however, PFS and OS were similar compared to those without trisomy 12. Unmutated IGHV, del(11q), and complex karyotype were adverse prognostic factors for PFS in comparator-treated patients, but not in those treated with ibrutinib. This integrated analysis found that patients with del(11q) had longer PFS than patients without del(11q). Lastly, results suggest that genomic risk factors associated with poor outcomes with traditional therapies have less relevance with ibrutinib treatment.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?