All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
MRD-guided venetoclax consolidation in CLL: Latest updates from the phase II HOVON 139/GiVe trial
In the past few years, fixed-duration combination strategies for patients with CLL have demonstrated benefit in terms of lower side effects, reduced chances of resistance, and lower costs compared to single-agent treatments. In particular, fixed-duration combination regimens including venetoclax with an anti-CD20 antibody have been investigated in pivotal trials: The MURANO study (NCT02005471) of fixed-duration venetoclax plus rituximab followed by 18 cycles of venetoclax monotherapy reported a 2-year progression-free survival (PFS) of 84.9%; the CLL14 study (NCT02242942), which included fixed-duration venetoclax plus obinutuzumab followed by an additional six cycles of of venetoclax monotherapy, demonstrated a 2-year PFS of 88.2%. Based on the results, these fixed-duration combination regimens have been approved by regulatory bodies. However, an optimal duration treatment for consolidation therapy with venetoclax after fixed-duration venetoclax plus obinutuzumab has not been established. Of note, analysis of the mentioned fixed-duration combination studies showed the predictive value of MRD status as a surrogate marker of PFS and individual treatment sensitivity. Thus, timing of undetectable MRD (uMRD) may potentially inform duration of therapy. The phase II HOVON 139/GiVe trial is the first available study to investigate the efficacy and safety of a predetermined 12-cycle venetoclax consolidation compared to MRD-guided venetoclax consolidation following a fixed-duration combination therapy of venetoclax plus obinutuzumab.
The Lymphoma Hub previously published an article reporting the preliminary results of the HOVON 139/GiVe trial (EudraCT [2015-004985-27]; the Netherlands Trial Register [NTR6043]), presented by Mark-David Levin at the European Hematology Association (EHA)2021 Virtual Congress.1 A recently published article by Kersting, et al., reported the interim study primary endpoint analysis (uMRD in bone marrow and no progressive disease 3 months after end of consolidation treatment), including a median follow-up of 35.2 months.2
The HOVON 139/GiVe study design and patient baseline characteristics2
The ongoing phase II HOVON 139/GiVe trial is a multicenter, open-label, randomized, parallel-group study conducted at 25 hospitals in the Netherlands. Patients ≥18 years old with previously untreated symptomatic CLL considered unfit to receive first-line fludarabine treatment were included in the study. Eligible patients received preinduction therapy with obinutuzumab (two cycles) and fixed-duration induction therapy with obinutuzumab plus venetoclax (12 cycles). Following induction therapy, patients were randomized (1:1) to the following venetoclax consolidation treatment arms (Figure 1):
- Consolidation group: 12 cycles of venetoclax irrespective of MRD status.
- MRD-guided consolidation group: MRD-guided venetoclax (maximum 12 cycles) with treatment limited to patients with detectable MRD in the peripheral blood (PB) after induction.
The study primary endpoint included uMRD in bone marrow and no progressive disease according to the International Workshop on Chronic Lymphocytic Leukemia (IwCLL) criteria at 3 months after end of consolidation.
MRD was assessed at a central laboratory by six-colour flow cytometry using an international standardised approach. MRD was categorized as undetectable (<10-4; <1 CLL cell per 10,000 leukocytes), low positive (≥10-4 and <10-2), and high positive (≥10-2). Safety was assessed in all patients receiving at least one study drug. Interim analysis was performed when the first 30 patients had completed the first three cycles of therapy (February 2018) and reviewed by an independent data monitoring committee. At the data cutoff date of 11 February, 2021, all patients had been off treatment for ≥8 months, with a median follow-up of 35.2 months (IQR, 31.5–41.3).
Figure 1. Study design*
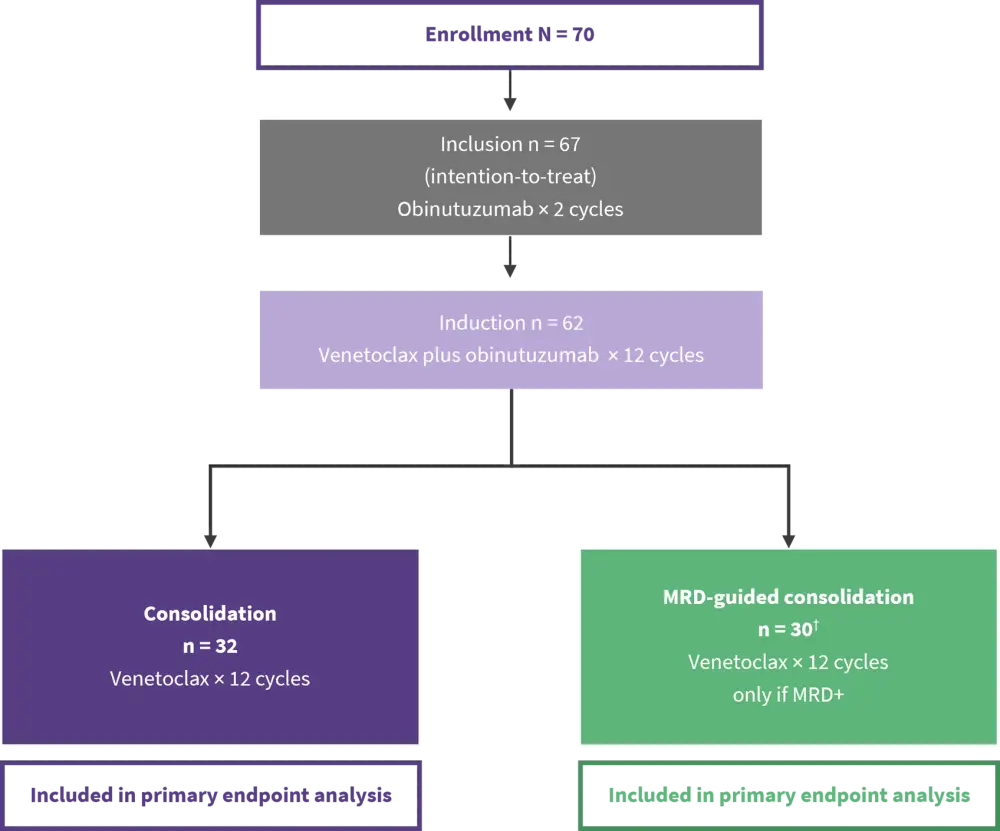
MRD, minimal residual disease.
*Adapted from Kersting, et al.2
†One patient was MRD+ at randomization and received venetoclax consolidation cycles one to three; one patient incorrectly received venetoclax consolidation cycles four to 12.
The study enrolled 70 patients and a total of 67 patients were included (intention-to -treat population). Of these, 62 patients proceeded to randomization: 32 patients were assigned to the consolidation group, 30 patients were assigned to the MRD-guided consolidation group. Of note, within the MRD-guided consolidation group, only one patient presented MRD positivity at randomization and received venetoclax consolidation cycles one to three, subsequently showing uMRD in PB. The remaining 29 patients in this study arm had uMRD at randomization, thus they did not receive venetoclax consolidation, although one patient who presented uMRD at randomization mistakenly received venetoclax consolidation cycles four to 12. Table 1 summarizes patient baseline characteristics.
Table 1. Key patient baseline characteristics in ZUMA-12*
|
Baseline characteristic, n (%) |
N = 40 |
|---|---|
|
DA-EPOCH-R, etoposide phosphate, prednisone, vincristine sulphate (Oncovin), cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), and rituximab; ECOG, Eastern Cooperative Oncology Group; FISH, fluorescence in situ hybridization; IPI, International Prognostic Index; R-CHOP, rituximab, cyclophosphamide, hydroxydaunorubicin hydrochloride (doxorubicin hydrochloride), vincristine (Oncovin) and prednisone. |
|
|
Median age (range), years |
61 (23–86) |
|
≥65 years |
15 (38) |
|
Male |
27 (68) |
|
Disease stage III–IV |
38 (95) |
|
ECOG Performance Status ≥1 |
25 (63) |
|
One prior systemic line |
32 (100) |
|
Double- or triple-hit only |
6 (15) |
|
Double- or triple-hit and IPI ≥3 |
4 (10) |
|
IPI ≥3 only |
20 (50) |
|
Deauville score |
|
|
4 |
19 (48) |
|
5 |
21 (53) |
|
Alterations by FISH |
|
|
MYC |
19 (48) |
|
BCL2 |
15 (38) |
|
BCL6 |
10 (25) |
|
Previous systemic therapy |
|
|
R-CHOP |
19 (48) |
|
DA-EPOCH-R |
18 (45) |
|
Neither R-CHOP nor DA-EPOCH-R |
6 (15) |
Treatment response2
- At 3 months after the last consolidation cycle, 50% (95% CI, 32–68) of patients in the consolidation group and 53% (95% CI, 34–72) of patients in the MRD-guided consolidation group met the primary endpoint of uMRD in bone marrow (BM) and no progressive disease.
- Overall, 94% (63/67) of patients on fixed-duration treatment in the intention-to-treat population had an overall response; 31% (21/67) had a complete response.
- At completion of trial assessment, 41% (13/32) of patients in the consolidation group and 60% (18/30) in the MRD-guided consolidation group showed a complete response; overall response occurred in 78% (25/32) and 97% (29/30) of study groups, respectively.
Figure 2 shows key study outcome measures at primary endpoint analysis.
Figure 2. uMRD, complete response, and overall response at primary endpoint analysis*
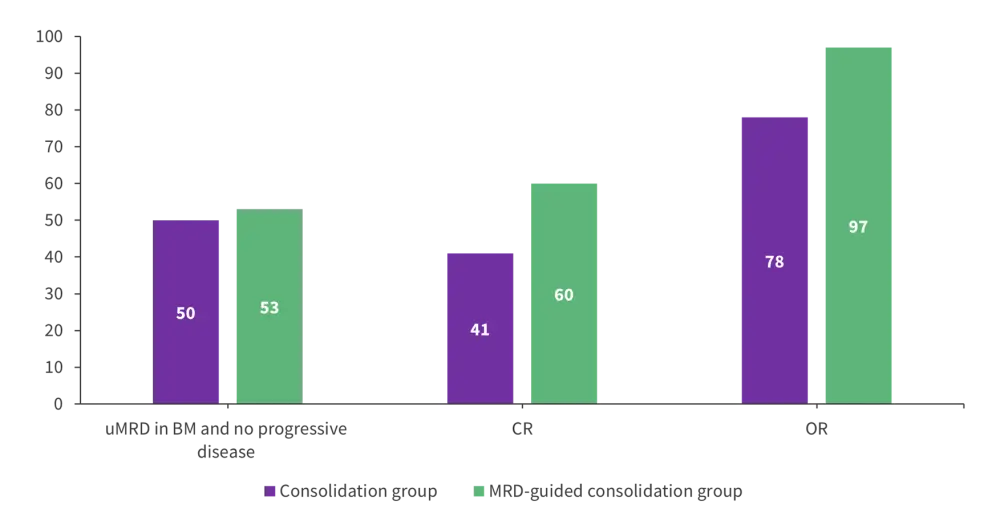
BM, bone marrow; CR, complete response; OR, overall response; uMRD, undetectable minimal residual disease.
*Data from Kersting, et al.2
Detection of MRD2
- In the intention-to-treat population:
- uMRD in PB was reached after cycle six of venetoclax plus obinutuzumab in 84% (56/67) patients and after cycle 12 in 88% (59/67) of patients.
- 79% (53/67) patients reached uMRD in BM after cycle 12 of venetoclax plus obinutuzumab.
- In the consolidation group:
- 84% (27/32) of patients had uMRD in BM at the time of randomization; the proportion decreased to 59% (19/32) 3 months after consolidation cycle 12.
- 94% (30/32) patients presented uMRD in PB at the time of randomization; the percentage decreased to 72% (23/32) 3 months after consolidation cycle 12.
- In the MRD-guided consolidation group:
- 87% (26/30) of patients showed uMRD in BM at the time of randomization; at the end of trial evaluation, the proportion decreased to 57% (17/30).
- 97% (29/30) patients presented uMRD in PB at the time of randomization; the proportion decreased to 57% (17/30) at the end of trial assessment.
Table 2 summarizes MRD dynamics in the two study groups.
Table 2. uMRD in BM and PB in the two study arms*
|
BM, bone marrow; PB, peripheral blood; uMRD, undetectable minimal residual disease. |
||
|
uMRD, %
|
Consolidation group |
MRD-guided consolidation group |
|---|---|---|
|
BM |
|
|
|
At randomization |
84 |
87 |
|
At primary endpoint |
59 |
57 |
|
PB |
|
|
|
At randomization |
94 |
97 |
|
At primary endpoint |
72 |
57 |
Safety analysis2
- Grade 2–4 adverse events were reported by 69% (22/32) of patients in the venetoclax consolidation group and 37% (11/30) in the MRD-guided consolidation group, mainly including infections.
- The most common Grade ≥3 adverse events were infections (6% of patients in the consolidation group and 3% in the MRD-guided consolidation group) and neutropenia (6% of patients in the consolidation group and 7% in the MRD-guided consolidation group).
- No patients developed clinical tumour lysis syndrome.
- No treatment-related deaths were reported in the study.
Conclusion2
This primary endpoint analysis of the HOVON 139/GiVe trial showed that 12 cycles of fixed-duration venetoclax plus obinutuzumab resulted in a high rate of uMRD in previously untreated patients with CLL. Consolidation with 12 cycles of venetoclax did not provide further improvement as loss of MRD response occurred regardless of prolonged venetoclax exposure. The proportion of patients who met the primary endpoint at the completion of trial assessment was similar in the two study groups (50% in the consolidation group vs 53% in the MRD-guided consolidation group). Toxicity of fixed-duration venetoclax plus obinutuzumab therapy was manageable and no treatment-related adverse events were observed. A more comprehensive evaluation of MRD kinetics may be needed to effectively select patients who could benefit from venetoclax consolidation.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In your experience, what is the average time to secure a reimbursed CAR T-cell therapy manufacturing slot for patients with DLBCL (from decision to treatment with a CAR T-cell therapy)?