All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Caribou Biosciences, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
The effect of lisocabtagene maraleucel vs standard of care on health-related quality of life in patients with R/R LBCL
Do you know... As part of the TRANSFORM study, health-related quality of life was compared in patients receiving lisocabtagene maraleucel (liso-cel) vs standard of care (SOC). Which statement below is correct?
Lisocabtagene maraleucel (liso-cel) is a CD19-directed autologous chimeric antigen receptor (CAR) T‑cell therapy in which CD8+ and CD4+ CAR+ T cells are administered at equal target doses.1 Previously, the Lymphoma Hub reported on the announcement that liso‑cel was granted U.S. Food and Drug Administration (FDA) approval for the second-line treatment of relapsed/refractory (R/R) large B-cell lymphoma (LBCL).
For patients with primary refractory LBCL, or those who progress within 12 months of first-line therapy, the standard of care (SOC) is a multi-agent, platinum-based salvage chemotherapy regimen followed by consolidation with high-dose chemotherapy (HDCT) and autologous stem cell transplantation (ASCT).1 This is problematic in that a significant proportion of patients aren’t eligible or able to tolerate HDCT or ASCT. Encouragingly, in the TRANSFORM study (NCT03575351), liso-cel demonstrated significantly improved efficacy compared to SOC as second-line therapy in patients with R/R LBCL.1 Furthermore, the results of the phase II PILOT study demonstrated the efficacy of liso-cel as a second-line treatment for patients with R/R LBCL who are not intended for HSCT, which was also reported by the Lymphoma Hub.
During the TRANSFORM study, data were collected on health-related quality of life (HRQoL) to compare liso-cel versus SOC from the patient’s perspective. Here, we summarize a study published in Blood Advances by Abramson et al.1 that presented an analysis of these data.
Study design
The phase III TRANSFORM study compared liso‑cel with SOC in patients with LBCL who had primary refractory disease or who had relapsed within 12 months of first-line therapy. Eligible patients were aged 18–75 years, had an Eastern Cooperative Oncology Group performance status ≤1, adequate organ function, and were eligible for HDCT and ASCT.
As shown in Figure 1, patients were randomly allocated to treatment with liso-cel or SOC. For patients randomized to the liso-cel arm, lymphodepletion with fludarabine/cyclophosphamide occurred prior to liso-cel infusion. During the liso-cel manufacturing time, patients could receive bridging therapy with one cycle of a protocol-defined SOC regimen. For patients randomized to the SOC arm, up to three cycles of salvage therapy were administered, and HDCT and ASCT would proceed in patients with an adequate response.
Figure 1. TRANSFORM study design*
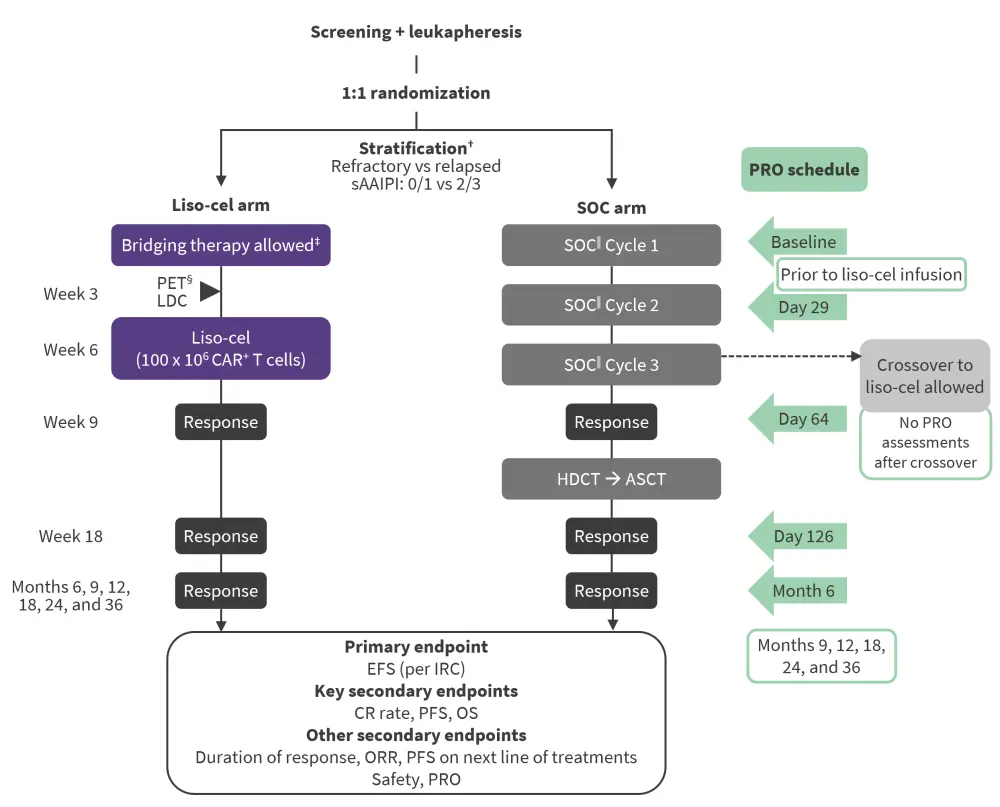
ASCT, autologous stem cell transplantation; CAR, chimeric antigen receptor; CR, complete response; EFS, event-free survival; HDCT, high-dose chemotherapy; IRC, independent review committee; LDC, lymphodepleting chemotherapy; liso-cel, lisocabtagene maraleucel; ORR, objective response rate; OS, overall survival; PET, positron emission tomography; PFS, progression-free survival; PRO, patient-reported outcome; R-DHAP, rituximab, dexamethasone, cytarabine, and cisplatin; R-GDP, rituximab, gemcitabine, dexamethasone, and cisplatin; R-ICE, rituximab, ifosfamide, carboplatin, and etoposide; sAAIPI, secondary age-adjusted International Prognostic Index; SOC, standard of care.
*Adapted from Abramson, et al.1
†Randomization stratification factors included response to first therapy (stable disease, progressive disease, partial response, or CR with relapse before 3 months vs CR with relapse on or after 3 months) and sAAIPI (0/1 vs 2/3).
‡Patients may have received a protocol-defined SOC regimen to stabilize their disease during liso-cel manufacturing.
§Only for patients who received bridging therapy.
‖SOC was defined as physician’s choice of R-DHAP, R-ICE, or R-GDP.
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-30 items (EORTC QLQ-C30) and the Functional Assessment of Cancer Therapy-Lymphoma subscale (FACT-LymS) were used to assess HRQoL. For EORTC QLQ-C30, within-group minimally important differences (MIDs) were used to determine whether a change in the score from baseline was clinically meaningful.
To estimate treatment effects on change scores for FACT-LymS and each of the EORTC QLQ-C30 domains, a mixed-effects regression model for repeated measures (MMRM) analysis was used. This included all data points from baseline to Day 126 and controlled for relevant baseline covariates.
Results
Baseline characteristics
As shown in Table 1, baseline characteristics were generally balanced between the liso-cel and SOC arm.
Table 1. Baseline demographics of the EORTC QLQ-C30 analysis set*
|
ECOG PS, Eastern Cooperative Oncology Group performance status; EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-30 items; IQR, interquartile range; sAAIPI, secondary age-adjusted International Prognostic Index. |
|||
|
Characteristic, % unless otherwise stated |
Liso-cel arm |
SOC arm |
All patients |
|---|---|---|---|
|
Male |
46.8 |
65.1 |
55.6 |
|
Age |
|
|
|
|
Median, years (IQR) |
59 (53–67) |
56 (37–64) |
58 (43–66) |
|
<65 years |
68.1 |
76.7 |
72.2 |
|
65–74 years |
31.9 |
23.3 |
27.8 |
|
Baseline ECOG PS |
|
|
|
|
0 |
44.7 |
58.1 |
51.1 |
|
1 |
53.2 |
41.9 |
47.8 |
|
2 |
2.1 |
0 |
1.1 |
|
sAAIPI |
|
|
|
|
0 or 1 |
57.4 |
60.5 |
58.9 |
|
2 or 3 |
42.6 |
39.5 |
41.1 |
|
Prior response status |
|
|
|
|
Refractory |
78.7 |
72.1 |
75.6 |
|
Relapsed |
21.3 |
27.9 |
24.4 |
|
Median time from initial diagnosis to randomization, months (IQR) |
7.0 (5.9–10.2) |
8.3 (5.9–11.4) |
7.4 (5.9–10.6) |
Baseline EORTC QLQ-C30 scores
At baseline, mean EORTC QLQ-C30 scores in both the liso-cel and SOC arms were generally comparable to a general population with similar age and gender distributions. Differences however were noted for role functioning and social functioning of the EORTC QLQ-C30 in both arms, in which mean scores were considerably worse than the general population.
Changes from baseline for EORTC QLQ-C30 scores
Clinically meaningful worsening of observed mean change scores was seen in the SOC arm in:
- global health status/QoL at Month 6;
- fatigue at Day 29 and Month 6; and
- pain at Month 6.
However, no other meaningful deterioration was seen in other domains of interest in either treatment arm.
As shown in Table 2, clinically meaningful improvements in the liso-cel arm were seen in the cognitive functioning and fatigue domains based on overall least square mean changes. Differences in the emotional functioning domain favored the SOC arm, but in all other domains the differences between treatment arms were minimal and fell within between-group MIDs.
Table 2. Least squares mean changes from baseline to day 126 in liso-cel vs SOC treatment arms*
|
CI, confidence interval; EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-30 items; HRQOL, health-related quality of life; MID, minimally important differences; QoL, quality of life; SOC, standard of care. |
||||
|
EORTC QLQ-C30 domain† |
Least squares mean (95% CI) |
Between-group MID |
||
|---|---|---|---|---|
|
Liso-cel |
SOC |
Difference |
||
|
Global health status/QoL |
3.1 |
<0.1 |
3.0 |
4 |
|
Emotional functioning |
2.2 |
7.0 |
−4.8† |
3 |
|
Cognitive functioning |
−2.2 |
−2.1 |
4.3‡ |
3 |
|
Fatigue |
2.0 |
3.8 |
−5.7‡ |
5 |
Patients with clinically meaningful changes
The proportion of patients with meaningful improvements in global health status/QoL was higher in the liso-cel arm, with also a lower proportion of patients deteriorating in comparison to the SOC arm from Day 126 to Month 6 (Figure 2). At Month 6, a tendency for improved pain scores in the liso-cel arm and deterioration in the SOC arm was noted.
Figure 2. Proportion of patients with clinically meaningful changes in EORTC QLQ-C30 global health/quality of life*
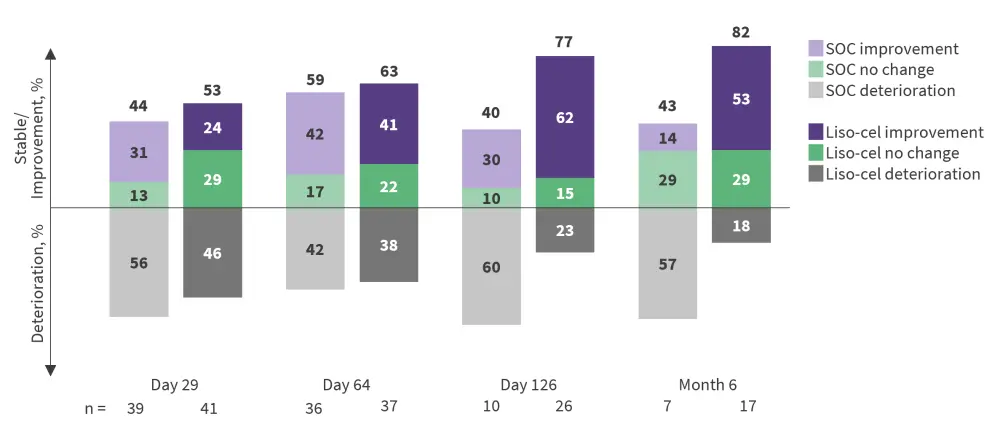
EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-30 items; SOC, standard of care.
*Adapted from Abramson, et al.1
Deterioration and sensitivity analyses
When comparing liso-cel versus SOC in global health status/QoL, time to confirmed deterioration was longer, thus favoring treatment with liso-cel (median, not yet reached by the time of data cutoff in liso-cel arm vs 19.0 weeks in the SOC arm; hazard ratio, 0.47; 95% confidence interval, 0.24–0.94)
Patients in the SOC arm trended towards a lesser risk of deterioration in emotional functioning in comparison to the liso-cel arm.
Sensitivity analyses (based on MMRM overall least squares mean changes estimated using a “while on treatment strategy”) found no clinically meaningful deterioration in any domain in the liso-cel arm relative to the SOC arm. Furthermore, improvements were seen in comparison to the SOC arm in:
- global health status/QoL (4.88; 95% CI, −1.97 to 11.73);
- cognitive functioning (3.73; 95% CI, −1.45 to 8.91); and
- fatigue (−5.01; 95% CI, −12.75 to 2.74).
Conclusion
More favorable HRQoL results were seen with liso-cel compared with SOC in the second-line treatment of R/R LBCL, including for global health status/QoL, cognitive functioning, and fatigue. The authors noted several limitations of their study, including lower-than-expected questionnaire completion rates, although response rates were similar between both study arms, as well as relatively short follow-up periods. Given 50% of patients in the SOC arm crossed over to receive liso‑cel as third-line therapy (at which point HRQoL was no longer assessed), the data in the SOC arm mainly represent patients who responded to treatments well. Despite these limitations, the results of the HRQoL assessments, in combination with superior efficacy results, further support liso-cel as a new SOC in the second-line treatment of patients with R/R LBCL.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
In patients with R/R LBCL who progress after CAR‑T, which of the following data would most strengthen your confidence in considering BV+R2?

