All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
ICML 2017 | BGB-3111, cerdulatinib, and other inhibitors for aggressive and indolent NHL – Targeting the BCR Pathway Session
“Targeting the BCR Pathway” was a session co-chaired by Prof. John F. Seymour (Peter MacCallum Cancer Center) and Prof. Catherine Thieblemont (Hôpital Saint-Louis), which the LH attended during the 14th International Conference on Malignant Lymphoma (ICML), Lugano, Switzerland.
Abstract 057
The first talk in this session was given by G. Lenz from the University of Münster, Münster, Germany, and conveyed results from an open-label, single-arm, phase II trial (NCT02391116) of copanlisib in patients with Relapsed/Refractory (R/R) Diffuse Large B-Cell Lymphoma (DLBCL).
Lenz began with an overview of DLBCL, a heterogeneous disease with distinct molecular subtypes, and accounts for around 30% of all malignant Lymphomas. The first-line standard of care for DLBCL is R-CHOP chemotherapy; however, approximately one-third of patients will relapse or have refractory disease which carries a poor prognosis and reduced survival. The different molecular subtypes of DLBCL are addicted to different oncogenic pathways; for example, PI3Kα and PI3Kδ are often expressed at high levels in most pre-clinical models of Activated B-Cell (ABC) like DLBCL. Copanlisib, a selective Class I PI3K inhibitor, how shown activity in preclinical models of ABC-DLBCL.
The current phase II trial assessed the treatment effect of copanlisib in R/R DLBCL patients in terms of Cell of Origin (COO) and molecular biomarker profiles.
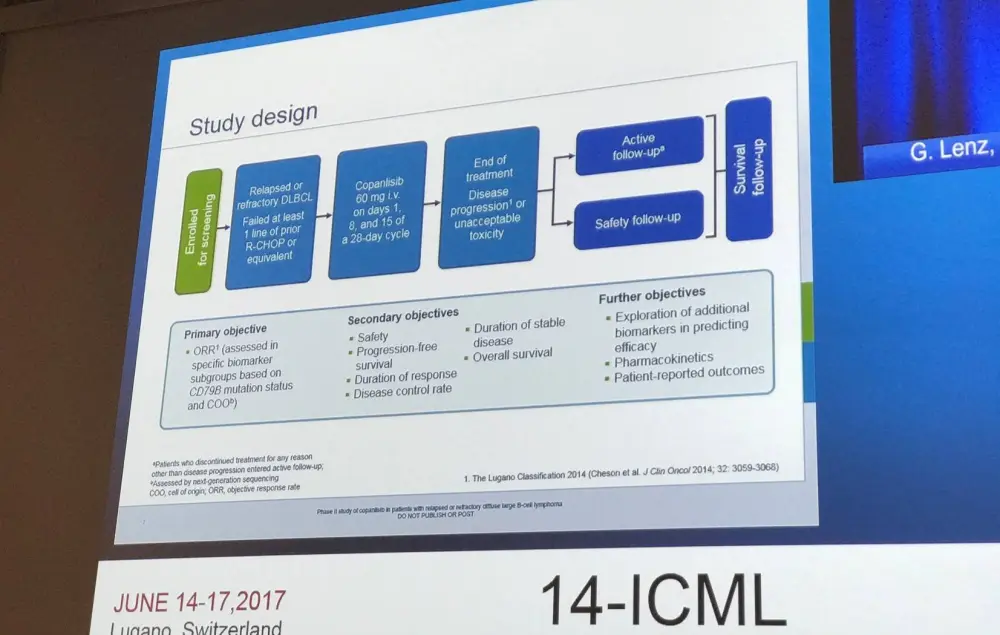
Patients were eligible is they had R/R DLBCL and ≥1 prior lines of therapy. Copanlisib at a dose of 60mg by IV infusion was administered intermittently on days 1, 8, and 15 of a 28-day cycle. Tumor samples were evaluated for COO, CD79B mutations, and more than 400 genes by Next Generation Sequencing (NGS). Objective tumor response rate (ORR) and response by COO and CD79B status were the primary outcome measures of the study.
Of 91 patients enrolled for screening, 24 failed and the remaining 67 patients initiated treatment. The Full-Analysis (FAS) and Per-Protocol Sets (PPS; ≥3 doses, post-baseline scans and COO/CD79B data) included 67 and 40 patients, respectively. The median age of patients was 69 years (range 25–93) and 58% of patients were male. ECOG status 0, 1, and 2 was reported in 22%, 57%, and 21%, respectively. Patients in this cohort were heavily pretreated, with a median of 3 previous lines of treatment (range, 1–13).
In biomarker evaluation of the 67 patients, 67.2% (n=45) had wild-type CD79B, 13.4% (n=9) had mutant CD79B, and 13 patients had missing data. When identifying COO, 44.8% (n=30) were assigned to Germinal Center B-Cell (GCB) like DLBCL, 28.4% (n=19) to ABC-DLBCL, 3 patients were unclassifiable, and 15 patients had missing data. Most patients excluded from the PPS (18/27) did not have CD79B mutation status and COO data available at baseline. In the PPS (n=40), 16 patients had ABC-DLBCL (6 with mutant CD79B), 22 patients had GCB-DLBCL (2 with mutant CD79B), and 2 patients had unclassifiable disease.
The AEs of specific interest that occurred with copanlisib treatment were hypertension (all, 40.3%; grade 3, 32.8%), diarrhea (all, 37.3%; grade 3, 1.5%), and hyperglycemia (all 32.8%; grade 3, 22.4%; grade 4, 9.0%).
ORR in the FAS was 19.4% (13/67) with a CR of 7.5% and a PR of 11.9%. ORR in the PPS was 25.0% (10/40) with a CR and PR of 12.5% each. ORR in patients with mutant CD79B (n=8) and in those harboring the wild-type gene (n=32) was 25.0% in both groups. ORR in patients with ABC-DLBCL (n=16) was 37.5% with a CR of 25.0% and a PR of 12.5%. In patients with GCB-DLBCL, ORR was 13.6% (CR 4.5%; PR 9.1%). In the two patients with unclassifiable disease, one patient achieved a PR and the other experience disease progression.
Exploratory mutation analysis by NGS of 54 patients identified 338 genes: BCL2 (54% of patients), TP53 (41%), BCL6 (30%), MYC (22%), CD79B (19%)/A (6%), MYD88 (19%), TNFAIP3 (17%), CARD11 (13%), and NFKBIA (9%). In patients who had both NGS and response data (n=44), differences in tumor response were identified based on BCL2 (ORR 17% vs. 35% for mutant vs. wild-type), BCL6 (ORR 17% vs. 28%), and MYC (ORR 13% vs. 28%) mutation status.
Lenz concluded the study by stating that copanlisib achieved encouraging responses with a manageable toxicity. Median PFS was 8.1 months in responders versus 1.8 months in non-responders. Copanlisib was particularly effective in ABC-DLBCL, achieving a higher ORR than patients with GCB-DLBCL. No difference was found in ORR between patients with mutant and wild-type CD79B.
Abstract 058
Pier Luigi Zinzani, MD, PhD, from the University of Bologna, Bologna, Italy, gave the second talk in this session, which focused on the phase II DYNAMO study (NCT01882803) of duvelisib in patients with double-refractory indolent Non-Hodgkin Lymphoma (iNHL).
Duvelisib is an oral, dual inhibitor of PI3Kδ and PI3Kγ and therefore not only targets malignant B-cells, but their supportive microenvironment as well. A phase I study in advanced B- and T-cell lymphomas has demonstrated that duvelisib has robust clinical activity.
The DYNAMO trial enrolled patients with either of three iNHL disease subtypes: Follicular Lymphoma (FL; n=83), Small Lymphocytic Lymphoma (SLL; n=28), or Marginal Zone Lymphoma (MZL; n=18). Patients were double-refractory to rituximab, either as a single-agent or in combination, and to chemotherapy/radioimmunotherapy.
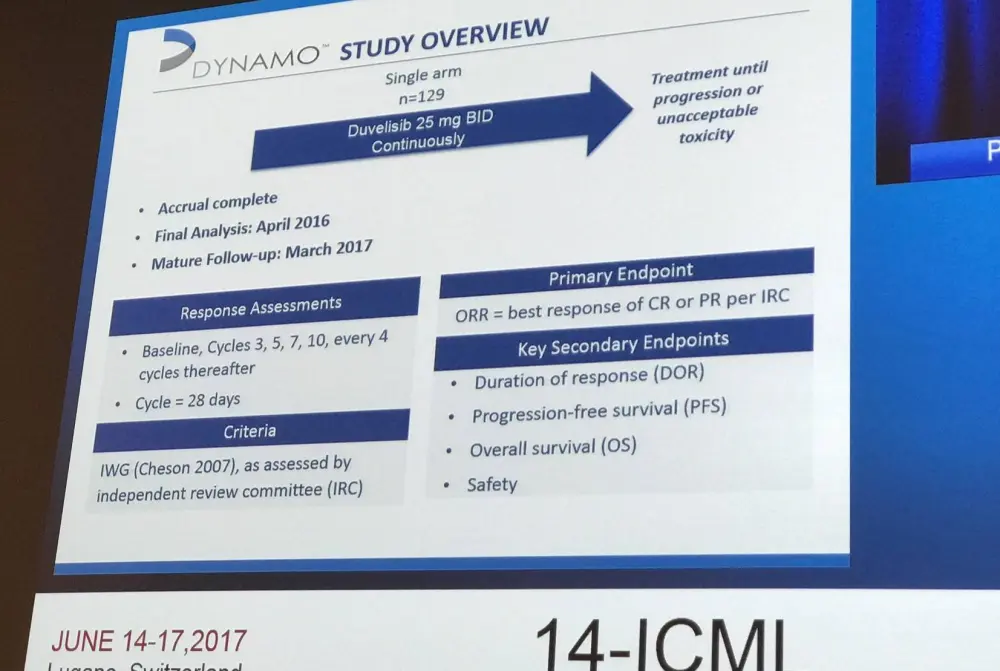
The 129 patients have been recruited from multiple centers from the US (n=46) and Canada (n=9), as well as Western (n=42) and Eastern (n=32) Europe. All patients had a median age of 65 years (range, 30–90), with a median of 3 (range, 1–18) prior anti-cancer regimens, and a median time since completion of last therapy of 4 months (range, 0–121). Overall, 96% of patients were refractory to their last therapy, and 77% were refractory to at least two therapies.
ORR per Independent Review Committee (IRC) and Investigator (Inv) assessment were presented by Zinzani for the overall cohort, as well as the individual iNHL subtypes:
|
|
Overall (n=129) |
FL (n=83) |
SLL (n=28) |
MZL (n=18) |
|
|---|---|---|---|---|---|
|
ORR per IRC |
47% |
43% |
68% |
33% |
|
|
|
CR |
1% |
1% |
0 |
0 |
|
|
PR |
47% |
42% |
68% |
33% |
|
ORR per Inv |
60% |
53% |
86% |
50% |
|
|
|
CR |
3% |
2% |
4% |
6% |
|
|
PR |
57% |
51% |
82% |
44% |
A rapid time to response was observed, the median time being 2 months (range, 1.4–12). The median time on duvelisib was 7 months (range, 0.4–35). Median DoR for all patients was 9.9 moths (95% CI, 4.5–10.3) and in terms of the individual subtypes: FL = 7.9 months, SLL = 10.1 months; and MZL = 8.3 months. Median PFS for all patients was 9.0 months (range, 6.7–11.8), for FL patients was 8.3 months, for SLL patients was 11.7 months, and for MZL patients was 14.3 months. Median OS for the whole group was 27.8 months (95% CI, 20.8–NE).
The most common all grade hematologic AEs were neutropenia (33%), anemia (25%), and thrombocytopenia (23%). All grade non-hematologic AEs included diarrhea (475), nausea (30%), cough (28%), fatigue (28%), pyrexia (25%), rash (19%), vomiting (19%), and peripheral edema (17%). It was emphasized that there were few discontinuations due to severe AEs of interest such as pneumonitis, colitis, rash, and transaminitis. Serious opportunistic infections occurred in less than 4% of patients and included one PCP, two CMV, and two fungal pneumonia infections. Six deaths were attributed to treatment (colitis n=1; toxic epidermal necrolysis/sepsis syndrome n=1; drug reaction/eosinophilia/systemic symptoms n=1; pneumonitis/pneumonia n=1; viral infection n=1; and septic shock n=1).
Zinzani concluded by stating that monotherapy with duvelisib demonstrated clinical activity in patients with double-refractory iNHL, achieving ORRs of 47% and 60% per IRC and Inv assessment. The majority of patients (88%) had tumor reduction and responses were durable (median of 10 months). Moreover, duvelisib was found to have a manageable toxicity profile. In long-term follow-up (median 18 months), duvelisib remains well tolerated. Therefore, duvelisib presents as an important alternative treatment option in double-refractory iNHL patients who have limited therapy choices.
Abstract 059
Judith Trotman from Concord Repatriation General Hospital, Concord, Australia, presented the next abstract on BGB-3111 in patients with Waldenström Macroglobulinemia (WM).
Bruton’s Tyrosine Kinase (BTK) is a crucial player in B-Cell Receptor signaling; it is constitutively activated in WM and contributes to cell survival. Ibrutinib, the first-in-class BTK inhibitor, has demonstrated activity in WM: major response rate of 73% (including a 16% Very Good Partial Response [VGPR] rate) and a 3-year EFS of 68%. However, ibrutinib is associated with a range of AEs including bruising/easy bleeding, diarrhea, and cardiac arrhythmias.
BGB-3111 is a potent, specific BTK inhibitor that has been designed to minimize off-target inhibition of TEC- and EGFR-family kinases. Presented during this talk were updated safety and efficacy results from a cohort of WM patients treated with BGB-3111 in an ongoing open-label, multicenter, dose-finding, phase I study.
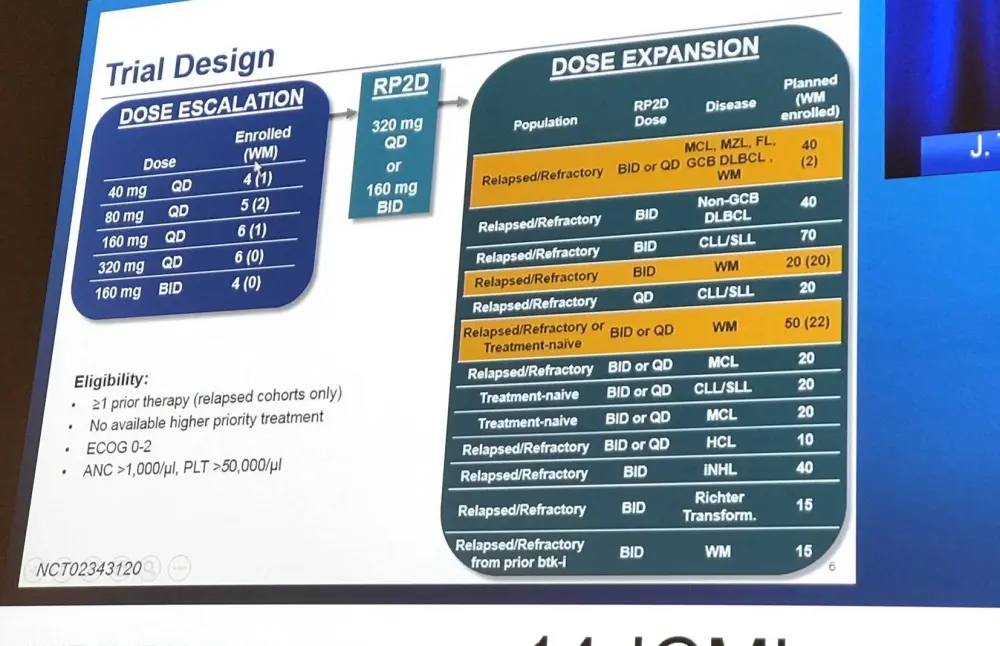
As of March 31st 2017, 48 patients with WM (10 Newly Diagnosed [ND]; 38 R/R) had been enrolled (safety population) and 42 of these (9 ND; 33 R/R) were eligible as part of the efficacy population. The median age of these patients is 66 years (range, 44–87) and they have a median of 1 prior therapy (range, 1–8). Overall, 4 patients are off-study due to Progressive Disease (PD; n=1) and AE (n=3), and 44 patients remain on study treatment (one of these patients has PD but remains on study drug due to clinical benefit).
The grade 3–4 AEs that occurred with BGB-3111 were anemia (8%), neutropenia (8%), diarrhea (2%), serious hemorrhage (2%) and headache (2%). At least one SAE occurred in 38% of patients and 6% of patients experienced events that resulted in treatment discontinuation. All grade atrial fibrillation was reported in 3 patients (6%), none grade 3–4.
Median follow-up was 12.3 months (4.4–30.5) and ORR was 90%, with a VGPR of 43% (18/41), PR of 33% (14/42), major response rate of 14% (6/42), and SD of 10% (4/42). Median IgM was reduced by 81.3% (32.7g/L to 6.1g/L) and median hemoglobin increased from 104.5g/L to 142g/L. Lymphadenopathy assessed by CT was reduced by a median of 45.5% (n=16; range, 18.2–81.4%). 12-month PFS was 91.7%.
Trotman concluded the talk by stating that BGB-3111 appears well tolerated and highly active in patients with WM. Currently, a phase III trial comparing BGB-3111 to ibrutinib in WM is ongoing; information on this trial was presented at 14-ICML by Christian Buske during the “Ongoing Trials” Focus On Session (abstract #OT06), which the LH also attended – read more here.
Abstract 060
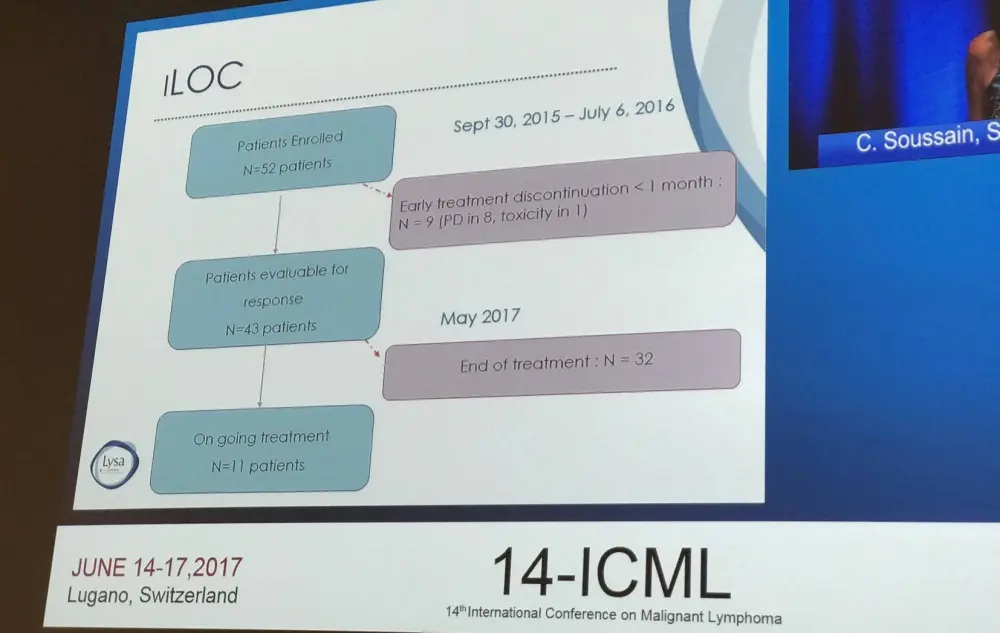
Primary endpoint results from the phase II iLOC study (NCT02542514) of ibrutinib in Primary CNS (PCNSL) and Primary Vitreo-Retinal Lymphoma (PVRL) was the topic of the next talk given by Carole Soussain, MD, PhD, from Institut Curie, Saint-Cloud, France.
Primary CNS Lymphoma (PCNSL) is a DLBCL, primarily of ABC subtype, with a constitutive activation of the NF-kB pathway and mutations in MYD88 and CD79B. Ibrutinib has shown significant therapeutic activity in R/R non-CNS non-GCB DLBCL.
The iLOC study is a prospective, multicenter phase II trial eligible for immune-competent patients older than 18 years with R/R PCNSL or PVRL of DLBCL type. Patients received 560mg oral ibrutinib daily until disease progression or unacceptable toxicity. During the first 4 weeks, additional corticosteroids treatment was permitted in the event of a threatening or symptomatic edema. The primary outcome measure of the iLOC study was Disease Control (DC) rate (CR + CRu + PR + SD) after two months of treatment. Patients were evaluable for response if they received ≥90% of the planned dose for the first month of treatment.
Patients had a median age of 70 years (range, 52–81) and 60% (n=26) had received 2 or more prior anti-cancer therapies. Previous ASCT had taken place in 4 patients and 1 patient had received whole-brain radiotherapy. The majority of patients had relapsed disease (70%) with the remaining 30% having refractory disease. Corticosteroids were administered to 14 patients during the first cycle.
DC at 2 cycles of therapy was 70% (30/43) and ORR was 60% (26/43). CR/CRu was 23.2% (10 patients), PR was 37.2% (16 patients), SD was 9.3% (4 patients), and PD was 30.2% (13 patients). Of patients who achieved CR, and PR, 10/10 and 12/16 had not received corticosteroids. In an unplanned Intention to Treat analysis (n=52) of DC at 2 cycles, DC was found to be 58% (30/52) and ORR was 50% (26/52).
When looking at DC at 2 cycles according to site of disease:
- Brain/spinal cord involvement at baseline (n=29)
- DC = 55% (16/29)
- CR = 4; PR = 10 including 5 nearly CR; SD = 2; PD = 13
- ORR = 48% (14/29)
- Intra-Ocular involvement at baseline (n=19)
- DC = 84% (16/19)
- CR = 10; PR = 4; SD = 2; ND = 1; inconclusive = 2
- ORR = 74% (14/19)
- Cerebrospinal Fluid involvement at baseline (n=4)
- CR = 3
Median follow-up was 9.2 months and the median number of cycles administered was 6. In 21 patients, treatment duration was longer than 6 months and in 11 patients this was 11 months or longer. Thirty-two patients discontinued treatment due to PD (n=25), toxicity of treatment (n=2), and other reasons (n=4).
Grade 3 AEs occurred in 16 patients (30.2%), grade 4 in five patients (9.4%), and grade 5 in four patients (7.5%). The most common AEs (>5% of patients) were infection (13.5%), general disorders (9.6%), blood and lymphatic system disorders (7.7%), nervous system disorders (7.7%), cardia disorders (5.8%), gastrointestinal disorders (5.8%), and vascular disorders (5.8%). SAEs of special interest included: ventricular hemorrhage (n=2), hyphema (n=1), atrial fibrillation (n=2), and two cases of pulmonary aspergillosis.
Soussain concluded the talk by stating that ibrutinib had manageable toxicity in patients with R/R PCNSL and PVRL and should be considered as an alternative option in selected patients at relapse. Furthermore, the benefit of combining ibrutinib with chemotherapy at relapse and in first-line treatment of PCNSL should be investigated.
Abstract 061
The penultimate talk in this session was given by Jason B. Kaplan, MD, from Northwestern University, Chicago, IL, US, and conveyed updated results from a phase I study of TAK-659 in R/R Lymphoma.
Spleen Tyrosine Kinase (SYK) is a crucial player in immune signaling in cancer, and regulates signaling through immune receptors such as BCRs and Fc receptors, proteins associated with EBV transformation, and cell-cell / cell-matrix interactions. Activated SYK expression is high in B-cell malignancies, myeloid tumors, and EBV-associated hematologic and solid tumors. It has been found that when SYK is inhibited, changes in immune cell population occur (regulatory T-cell, B-cell, MDSC, and TAMs).
TAK-659 is a selective, reversible inhibitor of SYK/FLT-3 activity, resulting in inhibition of cell proliferation in vitro and dose-dependent tumor growth inhibition in DLBCL xenograft models.
During this talk, Kaplan presented updated data for the Lymphoma population from the dose-escalation and expansion cohorts of a phase I study.
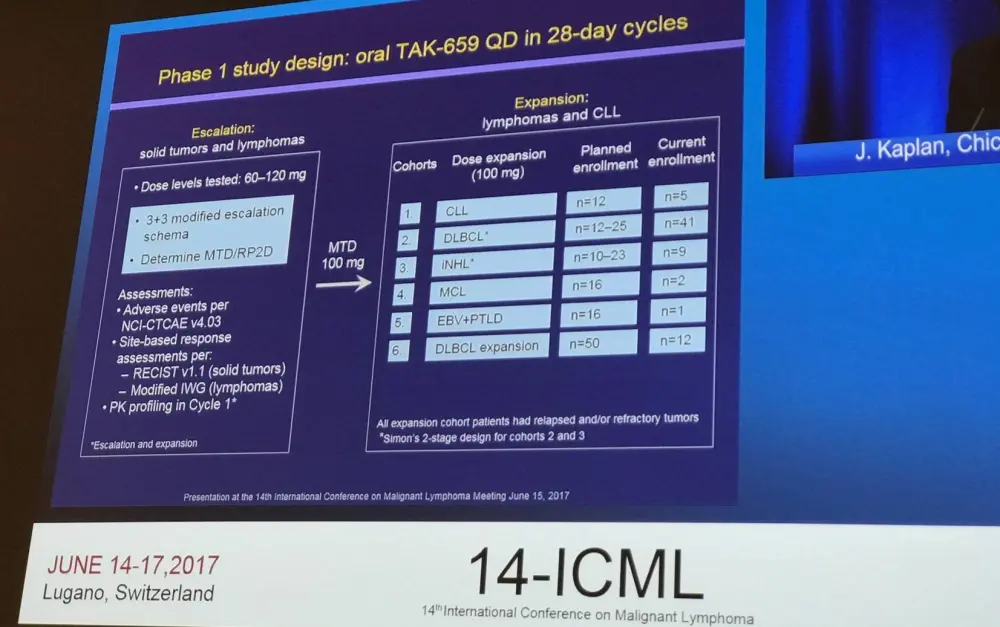
Adult patients with R/R Lymphoma were administered oral TAK-659 60–120 mg (escalation) or 100mg (expansion; including DLBCL, CLL, iNHL, MCL, and PTLD) QD in 28-day cycles. Eighty-seven patients were enrolled and had a median age of 65 years (range, 23–84), 68 patients were male. Patients had received a median of 3 (range, 1–9) previous therapies.
Of the 87 patients, 80 (92%) experienced an AE. The incidence of grade ≥3 AEs was 71% and SAEs occurred in 25%. SAEs that occurred in more than one patient included pyrexia (n=7; 8%), pneumonia (n=6; 7%), and pneumonitis (n=3; 3%). AEs resulting in treatment discontinuation were reported in 12 patients (14%0. There were 27 on study deaths, and 3 were attributed to treatment (multi-organ failure/sepsis cycle 1 day 22; respiratory failure/sepsis cycle 2 day 36; disseminated varicella infection cycle 3 day 46).
|
Patients n (%) |
DLBCL (n=45) |
iNHL (n=10) |
CLL (n=4) |
MCL (n=2) |
|---|---|---|---|---|
|
CR |
8 (18) |
1 (10) |
0 |
0 |
|
ORR |
12 (27) |
7 (70) |
2 (50) |
1 (50) |
Media treatment duration in all 87 patients was 43 days (1–987); in responders (n=22) and non-responders (n=65), this was 213 and 33 days, respectively. Median time to response in responders was 55 days (range, 27–168) and median DoR was 157.5 days (1–905).
Kaplan concluded by stating that the data to date indicates that TAK-659 is generally well tolerated. Anti-tumor activity was observed in patients with DLBCL and appears to be durable independent of COO classification of disease history (de novo versus transformed). Anti-tumor activity was also reported in patients with other histologies (such as iNHL, MCL, and CLL), as well as in patients who had received ibrutinib or idelalisib previously. Enrolment of patients with DLBCL, iNHL, CLL, MCL, and PTLD is ongoing (planned target of 152 patients); safety and efficacy will be further evaluated.
Abstract 062
Paul A. Hamlin, MD, from the Memorial Sloan Kettering Cancer Center, New York, NY, US, gave the last talk of the session, which focused on phase II results of cerdulatinib in patients with R/R B-cell malignancies.
SYK and JAK co-operate in order to control B-cell activation and appear to contribute to B-cell malignancies. Cerdulatinib, an orally available, ATP-competitive inhibitor of SYK, JAK1, JAK3, and Tyk2, has been shown to induce apoptosis in primary CLL cells (resulting in down-regulation of MCL1 and BCLXL), cells from ibrutinib-resistant CLL patients, and primary DLBCL and DLBCL cell lines with BCR pathway mutations resistant to ibrutinib. Therefore, SYK/JAK inhibition may potentially be a novel strategy to control B-cell malignancies.
The current phase II study is enrolling R/R patients (including patients who failed or were intolerant to BCR pathway or BCL2 inhibitors) with FL/iNHL, CLL/SLL, PTCL, and DLBCL/aggressive NHL; target accrual is 20–40 patients in each cohort. Patients enrolled so far have a median age of 70 years (range, 45–93) and a median number of 3 previous lines of therapy (range, 1–7). Eight patients (17%) have refractory disease and 12 patients (26%) achieved less than a PR to their last therapy.
Hamlin outlined the best overall response findings in a table:
|
Response |
CLL/SLL |
FL |
Other iNHL |
PTCL |
aNHL |
Total |
|---|---|---|---|---|---|---|
|
N |
18 |
9 |
7 |
1 |
5 |
40 |
|
CR |
0 |
0 |
0 |
1 |
0 |
1 |
|
PR |
12 |
5 |
1 |
0 |
1 |
19 |
|
ORR |
67% |
56% |
14% |
100% |
20% |
50% |
|
SD |
1 (7%) |
3 (33%) |
2 (40%) |
0 |
1 (20%) |
7 (18%) |
|
PD |
2 |
0 |
4 |
0 |
2 |
8 |
|
NE/safety |
3 |
1 |
0 |
0 |
1 |
5 |
Following this, the therapy-related AEs so far reported in four or more patients (n=47) were presented:
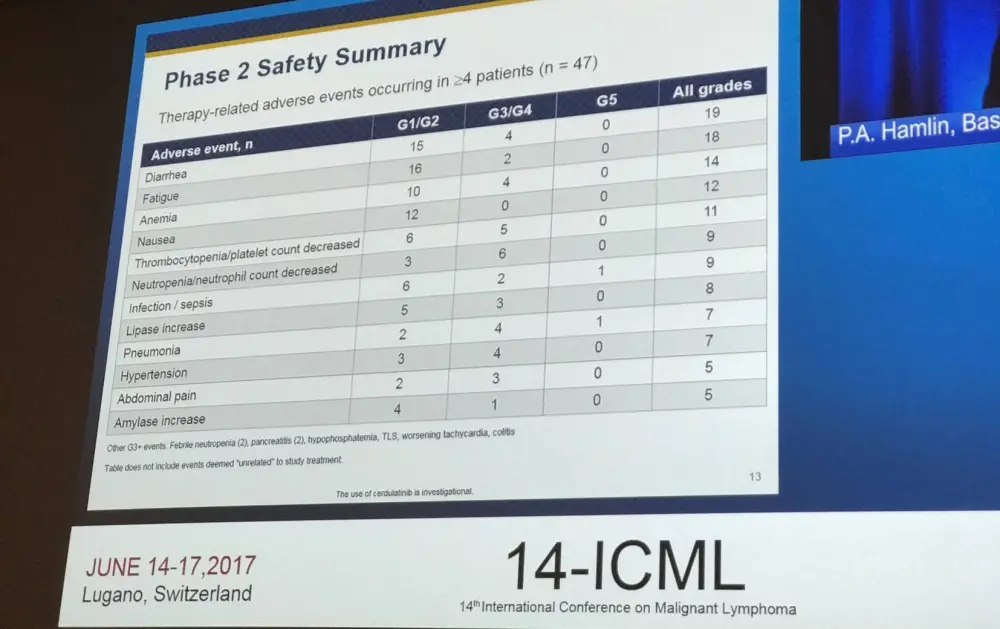
Two grade 5 events were reported at 35mg BID (sepsis, pneumonia). Both were PK outliers (>3 times target PK range). Dose reductions were required in around 50% of patients. Dose was reduced to 30mg BID, resulting in a reduction in PK variability and improved safety profile, while maintaining efficacy.
Hamlin concluded by stating that the results so far in this phase II study indicate that cerdulatinib has consistent activity in R/R CLL, SLL, and FL. Moreover, responses have been seen to improve over time; 7/9 patients with increased reduction at second or third re-scan. Evidence of apoptosis (Annexin V+) was observed in 11/14 CLL patients, 9 of whom achieved PR. It also became apparent that 30mg plus PK monitoring strategy maintained efficacy and improved safety/tolerability profile and resulted in a tighter PK range compared to 35mg BID.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?