All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, and Thermo Fisher Scientific and supported through independent educational grants from Bristol Myers Squibb, Incyte, Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
Key updates from ASH 2023: Novel treatment options for patients with RR WM
Waldenstrom’s macroglobulinemia (WM) is a disease which presents with a wide variety of clinical sequelae.1 Therefore, the therapeutic landscape is constantly evolving to provide options for patients with relapsed/refractory (R/R) WM.1 The Lymphoma Hub previously reported on the current treatment options and associated factors that influence treatment indications in this setting.
Below, we summarize three key presentations on novel treatment approaches for patients with R/R WM, presented during the 65th American Society of Hematology (ASH) Annual Meeting and Exposition.
Transitioning from ibrutinib to zanubrutinib: LTE1 study from ASPEN trial2
Garcia-Sanz presented results from the LTE1 study (NCT04170283), which is a long-term extension study of the ASPEN study (NCT03053440); this was previously summarized by the Lymphoma Hub. This extension study investigated safety and efficacy outcomes of ibrutinib-tolerant patients from the ASPEN study transitioning from treatment with ibrutinib to zanubrutinib. In total, 47 patients were assessed:
- disease response was maintained or improved in 96% of efficacy evaluable patients;
- best overall response (OR) was unchanged between data in the ASPEN and LTE1 trials (72%) but improved in ten patients; and
- one patient discontinued treatment before assessment.
More ibrutinib-related adverse events occurred in patients in the ASPEN trial compared with zanubrutinib-related adverse events in the LTE1 trial (Figure 1A). There were a total of two deaths due to COVID-19 in the LTE1 trial, with the only Grade ≥3 treatment-emergent adverse events (TEAEs) being infections occurring in ≥2 patients (Figure 1B). There was no recurrence of the majority of ibrutinib TEAEs following the switch to zanubrutinib.
Figure 1. A TEAEs in patients with ≥1 AE from ASPEN and LTE1 and B the most common Grade ≥3 TEAEs in LTE1*
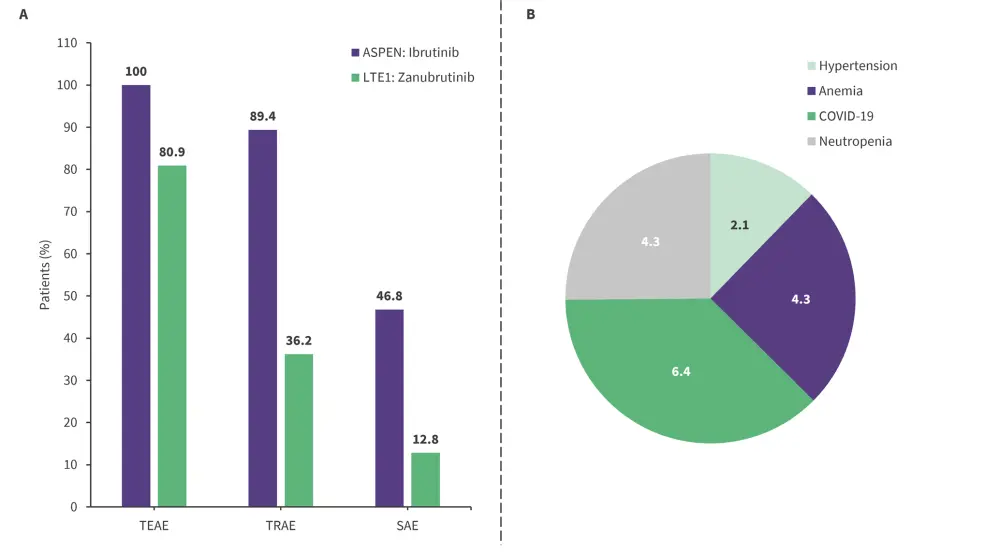
LTE, long-term extension; SAE, serious adverse event; TEAE, treatment-emergent adverse event; TRAE, treatment-related adverse event.
*Adapted from Garcia-Sanz.2
Presenter’s conclusions
Despite being limited by a small sample size, this subpopulation study demonstrated that patients treated with ibrutinib can switch to zanubrutinib therapy without compromising efficacy or safety; in some cases efficacy is improved.2 A longer follow-up study is ongoing to understand this data further.1
Orelabrutinib monotherapy3
Cao summarized follow-up data from a single-arm, multicenter, prospective phase II study (NCT04440059) evaluating efficacy and safety of orelabrutinib in patients with R/R WM. The primary endpoint was major response rate assessed by an independent review committee. In total, 47 patients were assessed. At a median follow-up of 31.9 months:
- The major response rate was 80.9%, with 25.5% of patients achieving a very good partial response in the full analysis set; the OR rate was 91.5%.
- The 36-month progression-free survival (PFS) was 72.1%; however, the median PFS was not reached.
- Specific genotype did not impact PFS, with no significant difference in PFS across MYD88 and CXCR4 genotypes
The safety profile was manageable, with most TEAEs reported being Grade 1 or 2. The most common Grade ≥3 TEAEs (occurring in ≥10% of patients) were neutropenia (10.6%), thrombocytopenia (8.5%), and pneumonia (6.4%); four patients (8.5%) discontinued treatment due to TEAEs.
Presenter’s conclusions3
Long-term follow-up data continues to show that orelabrutinib yields deep and durable responses in patients with R/R WM and has a manageable safety profile, with no new safety signals reported.
CAR T-cell therapy in transformed WM: a DESCAR-T and US collaborative study4
Houot summarized a real-world evidence study that investigated efficacy and safety of chimeric antigen receptor (CAR) T-cell therapy (axicabtagene ciloleucel [axi-cel], n = 13; tisagenlecleucel [tisa-cel], n = 9) in patients aged ≥18 years with transformed WM or lymphoplasmacytic lymphoma from DESCAR-T centers (n = 18) and two US centers (n = 4). The primary endpoint was best complete response (CR). Secondary endpoints included best OR rate, PFS, overall survival, and safety.
- Best CR (according to Lugano 2014 classification) was 86% and higher in patients treated with tisa-cel compared with axi-cel (89% vs 85%, respectively).
- Best OR (according to Lugano 2014 classification) was 95% and higher in patients treated with tisa-cel compared with axi-cel (100% vs 92%, respectively).
- Two patients with CNS involvement achieved CR at 1 month; one patient relapsed at 3 months and the other remains in CR at 12 months
- After 17-month median follow-up, PFS was 70.4% and overall survival was 84.1% at 12 months.
There were no unexpected safety events (Table 1) and there was a total of five deaths, four from lymphoma and one from COVID-19.
Table 1. Grade ≥3 AEs in all patients treated with CAR T-cell therapy*
|
Grade ≥3 AEs, % |
Total |
Axi-cel |
Tisa-cel |
|
AE, adverse event; axi-cel, axicabtagene ciloleucel; CAR, chimeric antigen receptor; CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome; NRM, non-relapse mortality; tisa-cel, tisagenlecleucel. |
|||
|
CRS |
9 |
15 |
0 |
|
ICANS |
9 |
15 |
0 |
|
Infection |
18 |
23 |
11 |
|
Prolonged cytopenia† |
|||
|
Neutropenia |
32 |
23 |
44 |
|
Anemia |
23 |
8 |
44 |
|
Thrombocytopenia |
36 |
31 |
44 |
|
NRM |
5‡ |
0 |
11‡ |
Presenters conclusions4
This study showed that CD19 CAR T-cell therapy is effective in patients with heavily pretreated R/R transformed WM. There were no unexpected toxicities, supporting the use of CAR T-cell therapy in this cohort of patients; longer follow-up studies are required to confirm the durability of its efficacy and safety.
'The International Waldenstrom's Macroglobulinemia Foundation (IWMF) and the Lymphoma Hub are working in collaboration for patients with Waldenstrom's macroglobulinemia. This initiative aims to increase awareness of Waldenstrom's macroglobulinemia among healthcare professionals, patients, caregivers, and the patient advocacy community.
This initiative is funded by Cellectar Biosciences, BeiGene and Eli Lilly. All content is developed independently by SES in collaboration with an expert steering committee; funders are allowed no direct influence on the content of the hub.’
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?

