All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Primary analysis of phase I/II of the ZUMA-6 trial – axicabtagene ciloleucel plus atezolizumab for patients with refractory DLBCL
The anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, axicabtagene ciloleucel (axi-cel), was approved in the US and Europe for the treatment of adult patients with relapsed/refractory (R/R) large B-cell lymphoma (LBCL) following two or more prior lines of therapy.1 The approvals were based on the results from the ZUMA-1 study, and the long-term results can be found on the Lymphoma Hub here.
The programmed death receptor 1 (PD-1) and its ligand (PD-L1) immune checkpoint axis is imperative for physiological immune regulation but is dysregulated in a number of cancers, resulting in decreased immune-mediated tumor destruction.2 Upregulation of PD-1 on CAR T-cells and PD-L1 on tumor cells has been observed following CAR T-cell infusion, which may jeopardize treatment effectiveness.3
The phase I/II of the ZUMA-6 (NCT02926833) study is currently investigating the safety and efficacy of axi-cel in combination with the humanized, anti-PD-L1 monoclonal antibody, atezolizumab (atezo), for the treatment of adult patients with R/R diffuse LBCL (DLBCL). The study aims to evaluate the hypothesis that immune checkpoint blockade may augment CAR T-cell activity.3
At the 2020 American Association for Cancer Research (AACR) virtual annual meeting, Caron Jacobson presented the results from the phase II portion of the ZUMA-6 study – below is a summary.3
ZUMA-6
- Data cutoff: February 21, 2019
- Median follow-up: 10.2 months
- Primary endpoints: Dose-limiting toxicities (DLTs; phase I) and complete response rate (phase II)
Patient eligibility
- R/R disease was defined as no response to the last chemotherapy or relapse ≤ 12 months following autologous stem cell transplant (auto-SCT)
- Prior therapy must have included an anti-CD20 monoclonal antibody and anthracycline
- Patients with DLBCL were screened, and those that met the inclusion criteria were enrolled at the time of T-cell collection
Phase I
- The phase I (n = 12) portion was a 3 × 3 design dose schedule finding study (Figure 1)
- Each patient received four fixed doses of atezo, one every 21 days, which differed by the time of the first atezo dose, with respect to axi-cel infusion
- No DLTs were observed in the first three patients in Cohorts 1 and 2
- One DLT was observed in the first three patients of Cohort 3 due to prolonged cytopenia
- Three more patients were enrolled, and no DLTs were observed
Phase II
- The dosing schedule employed in the Cohort 3 of phase I (Figure 1) was taken forward to the phase II dose schedule expansion, which enrolled a further 22 patients
- The total number of patients receiving the recommended phase II dosing schedule: 28
Figure 1. Study design for phase I/II portions of the ZUMA-6 study3
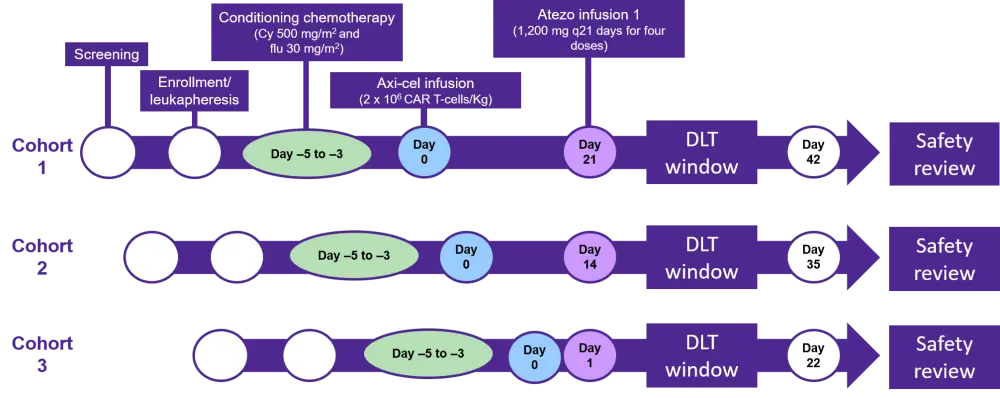
Atezo, atezolizumab; axi-cel, axicabtagene ciloleucel; Cy, cyclophosphamide; DLT, dose limiting toxicity; flu, fludarabine
Results
Results presented represent the phase I Cohort 3 and phase II portions of this study, unless stated otherwise.
Patient characteristics
- All patients enrolled across the study (N = 34) received axi-cel and ≥ one dose of atezo
- Ten patients did not receive all four doses of atezo, for reasons including
- disease progression (n = 3)
- adverse events (AEs; n = 6)
- death (n = 1)
- Patient characteristics are presented in Table 1
Table1. Baseline patient characteristics and tumor PD-L1 expression3
|
ECOG, Eastern Cooperative Oncology Group; IPI, International Prognostic Index *H = intensity score multiplied by the % of cells that were positive for each level. Four patients had missing data; †+1, +2, and +3 refer to weak, moderate, and strong staining for PD-L1 using the VENTANA PD-L1 assay. Four patients had missing data |
|
|
Characteristic |
Phase I Cohort 3 + phase II (n = 28) |
|
Median age, years (range) |
58 (42 – 71) |
|
Male, % |
57 |
|
ECOG performance status, % 0 1 |
61 39 |
|
Disease stage, % II III or IV |
21 79 |
|
IPI score, % 0 – 2 3 – 4 |
54 46 |
|
Prior therapies, % ≥ 2 ≥ 3 |
86 50 |
|
Primary refractory disease, % |
14 |
|
PD-L1 expression Median baseline tumor cell PD-L1 H score (range)* PD-L1 immune infiltrate intensity score,† % +1 +2 +3 |
40 (0 – 240)
25 25 39 |
AEs
- The most common Grade ≥ 3 treatment-emergent AEs (TEAEs) were cytopenias, electrolyte abnormalities and encephalopathy
- Grade ≥ 3 AEs were associated with axi-cel, atezo or both in 39%, 14% and 25% of patients, respectively
- One Grade 5 AE, not believed to be treatment-related, was observed on day +22 following axi-cel infusion, resulting in multiorgan failure and death
- Cytokine release syndrome (CRS) was experienced in 96% of patients with Grade 3 CRS observed in 4% of patients. None of the patients experienced Grade 4 or 5 CRS
- median time to onset of CRS was 2 days (1–13) with a median duration of 7 days (1–92)
- all events were resolved by the data cutoff
- Neurotoxicity was experienced in 68% of patients with Grade 3 or 4 neurotoxicity observed in 29% of patients. None of the patients experienced Grade 5 neurotoxicity
- median time to onset of neurotoxicity was 6 days (1–23) with a median duration of 9 days (2–60)
- two patients had ongoing events at the data cutoff: one patient with Grade 1 tremor and one patient with hypoesthesia
Efficacy
- Patient outcomes to axi-cel + atezo are presented in Figure 2 and Table 2
- The median duration of response (DOR), progression-free survival (PFS) and overall survival (OS) were not reached (Table 2)
- Four patients demonstrated late conversions as follows:
- Partial response – complete response (n = 3)
- Stable disease – complete response (n = 1)
Figure 2. Patient response rates3
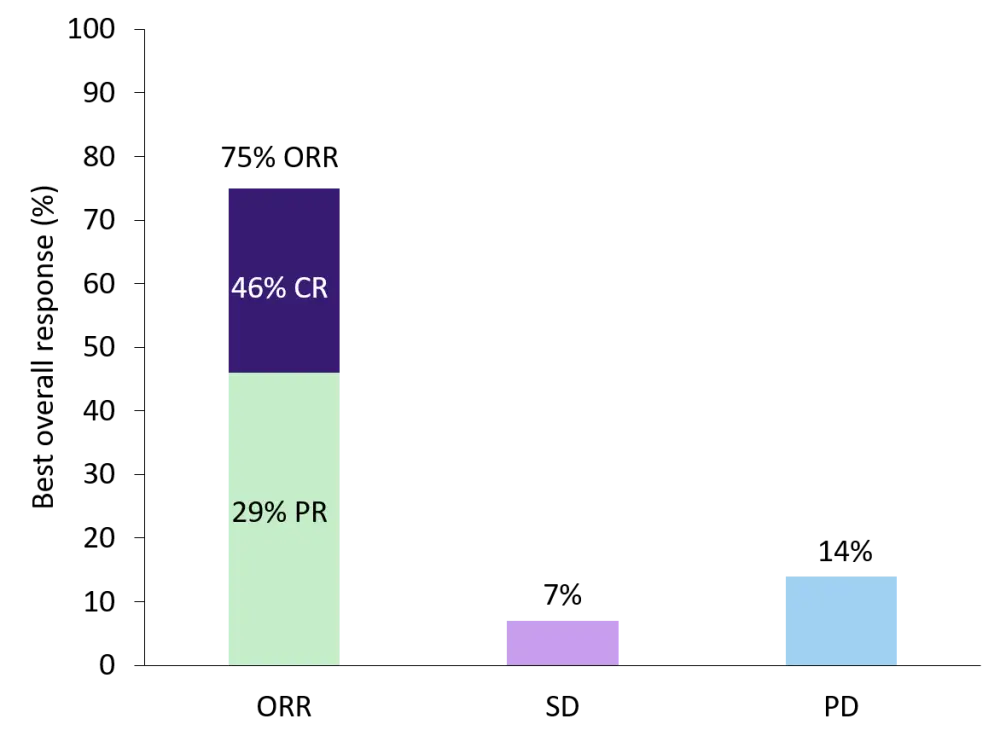
CR, complete response; ORR, overall response rate; PD, progressive disease; PR, partial response; SD, stable disease
Table 2. Patient outcomes3
|
CI, confidence interval; DOR, duration of response; NE, not evaluable; NR, not reached; OS, overall survival; PFS, progression-free survival *February 21, 2019 |
|
|
|
Phase I Cohort 3 + phase II (n = 28) |
|
Patients with ongoing response at cutoff*, % |
46 |
|
DOR Median, months 95% CI 6-month estimate, % |
NR 1.8 – NE 62 |
|
PFS Median, months 95% CI 6-month estimate, % |
NR 3.1 – NE 50 |
|
OS Median, months 95% CI 6-month estimate, % |
NR 12 – NE 71 |
Conclusions
The administration of atezo following axi-cel demonstrated, with a manageable safety profile, that it was consistent with that reported in the ZUMA-1 study. Although there has been no statistical comparison between patient outcomes in the ZUMA-6 vs ZUMA-1 studies, the combination of axi-cel with atezo demonstrated similar clinical efficacy to axi-cel alone. Similarly, the pharmacokinetic and pharmacodynamic profiles of axi-cel when administered with atezo were comparable to when the CAR T-cell therapy is administered alone. The timing of atezo administration with respect to CAR T-cell treatment is thought to impact CAR T-cell persistence and requires further investigation. A range of techniques are being employed to further define immune cell subsets and study the tumor microenvironment to better understand the anti-tumor immune response of axi-cel. Furthermore, enhanced knowledge of such parameters may prove prognostically valuable in deciding which patients could benefit from immune-checkpoint blockade alongside CAR T-cell therapy.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content