All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma & CLL Hub is an independent medical education platform, sponsored by AbbVie, BeOne Medicines, Miltenyi Biomedicine, Nurix Therapeutics, Roche, Sobi, and Thermo Fisher Scientific and supported through educational grants from Bristol Myers Squibb, Eli Lilly, and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
Axi-cel vs chemoimmunotherapy in older patients with R/R LBCL
Older patients with relapsed/refractory (R/R) large B-cell lymphoma (LBCL) have poor outcomes with standard salvage chemotherapy and stem cell transplantation.1 Additionally, older patients and/or patients with poor Eastern Cooperative Oncology Group Performance Status (ECOG PS) have limited treatment options. Axicabtagene ciloleucel (axi-cel), an autologous anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, is approved by the U.S. Food and Drug Administration (FDA) as a second-line treatment for patients with LBCL. A post-hoc analysis from the ZUMA-1 trial (NCT02348216) and a survival analysis from the ZUMA-7 trial (NCT03391466) demonstrated the effectiveness of axi-cel in patients aged ≥65 years with R/R LBCL.1
Below, we summarize results from an analysis comparing real-world outcomes of axi-cel vs chemoimmunotherapy (CIT) in patients with R/R LBCL after ≥2 lines of therapy, including patients aged ≥65 years and/or had an ECOG PS of 2, published by Lunning et al.1 in American Journal of Hematology.
Study design and patient population1
- This analysis compared outcomes of 1,146 patients from the Centre for International Blood and Marrow Transplant Research (CIBMTR) observational database treated with axi-cel vs 469 patients who received CIT from the retrospective SCHOLAR-1 study.
- Endpoints included overall response rate, complete response rate, and overall survival (OS).
- Median follow-up was 24.5 months (95% confidence interval [CI], 24.3–24.9) and 59.8 months (95% CI, 52.3–65.0) in the axi-cel and CIT groups, respectively.
Key findings1
Patient characteristics
- Before propensity score matching, patients in the axi-cel group were older, more likely to have ECOG PS <2, and were more heavily pretreated (Table 1).
- After propensity score matching:
- The response rate analysis set included 493 and 289 patients from the axi-cel and CIT groups, respectively.
- The survival analysis set included 659 and 406 patients from the axi-cel and CIT groups, respectively.
Table 1. Patient characteristics*
|
Baseline characteristics, % (unless otherwise specified) |
Axi-cel (n = 1,146) |
CIT (n = 469) |
|
Axi-cel, axicabtagene ciloleucel; CIT, chemoimmunotherapy; ECOG PS, Eastern Cooperative Oncology Group Performance Status. |
||
|
Median age, years (range) |
62.3 (19.6–86.2) |
55.4 (19.8–81.2) |
|
<65 years |
61 |
86 |
|
≥65 years |
39 |
14 |
|
≥70 years |
20 |
6 |
|
ECOG PS |
|
|
|
0–1 |
85 |
63 |
|
≥2 |
4 |
11 |
|
Unknown |
11 |
26 |
|
Prior lines of therapy |
|
|
|
2 |
34 |
96 |
|
≥3 |
66 |
4 |
Efficacy
- The estimated 12-month OS rate was 62% (95% CI, 58–66) and 28% (95% CI, 24–33) in the axi-cel and CIT groups, respectively.
- Median OS was longer in axi-cel vs CIT groups, respectively (hazard ratio [HR], 0.30; 95% CI 0.24–0.37) as well as in the subgroups:
- <65 years: HR, 0.29 (95% CI, 0.22–0.28)
- ≥65 years: HR, 0.32 (95% CI, 0.22–0.48)
- ECOG PS <2: HR, 0.27 (95% CI, 0.20–0.35)
- ECOG PS = 2: HR, 0.72 (95% CI 0.41–1.29).
- The overall response rate and complete response rates were also higher in the axi-cel vs the CIT group (Figure 1).
Figure 1. Response rate analysis showing A ORR and B CR rates in the axi-cel group vs CIT group*
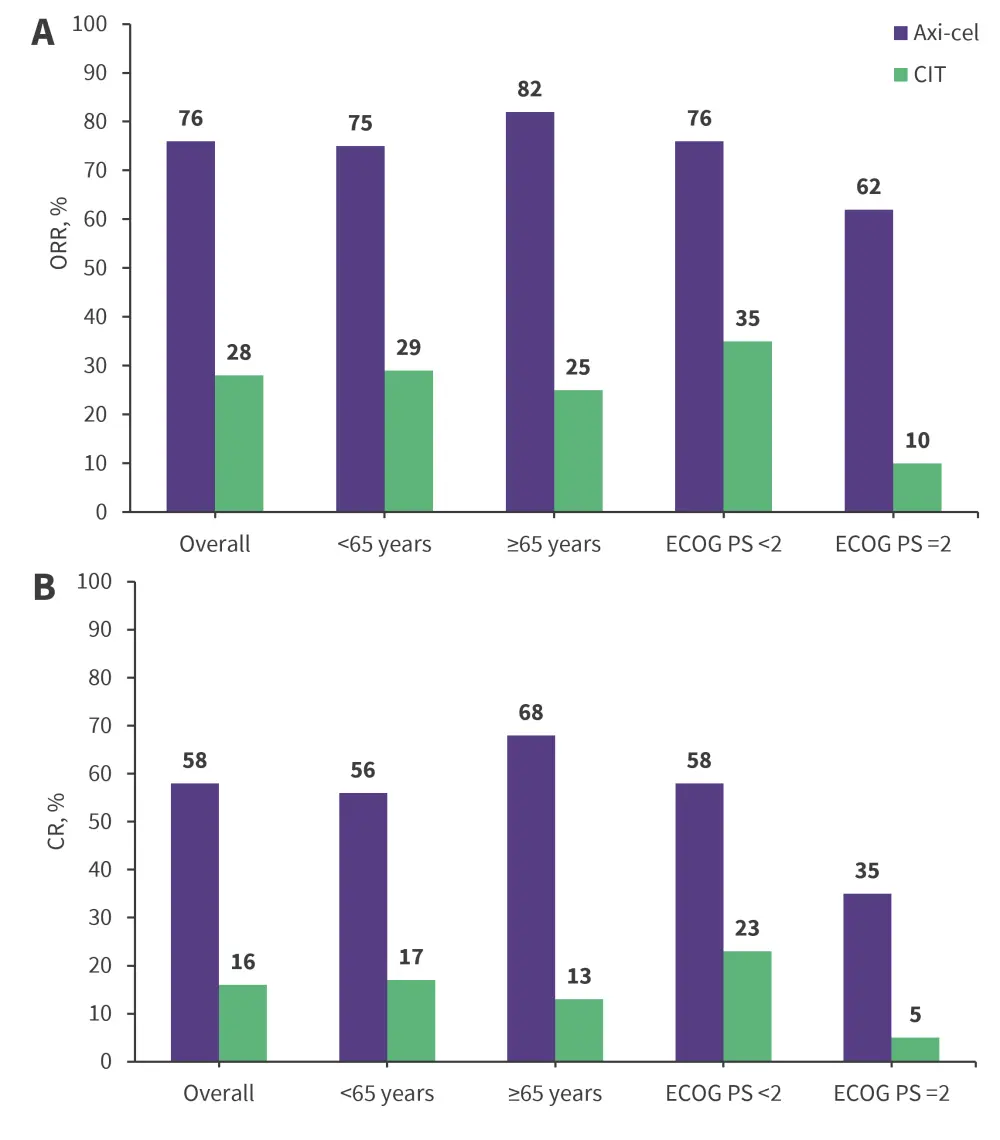
Axi-cel, axicabtagene ciloleucel; CIT, chemoimmunotherapy; CR, complete response; ECOG PS, Eastern Cooperative Oncology Group performance status; ORR, overall response rate.
*Adapted from Lunning, et al.1
| Key learnings |
|
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the primary reason you use bridging therapy in patients with DLBCL awaiting CAR T-cell therapy?



