All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Lymphoma Hub is an independent medical education platform, sponsored by Roche, Sobi, AbbVie, BeOne, Miltenyi Biomedicine, Thermo Fisher, Nurix Therapeutics and Caribou Biosciences and supported through independent educational grants from Incyte, Bristol Myers Squibb, Lilly and Pfizer. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View lymphoma & CLL content recommended for you
Tafasitamab for the treatment of patients with relapsed/refractory diffuse large B-cell lymphoma
Do you know... What is the rationale for combining tafasitamab and lenalidomide for the treatment of R/R DLBCL?
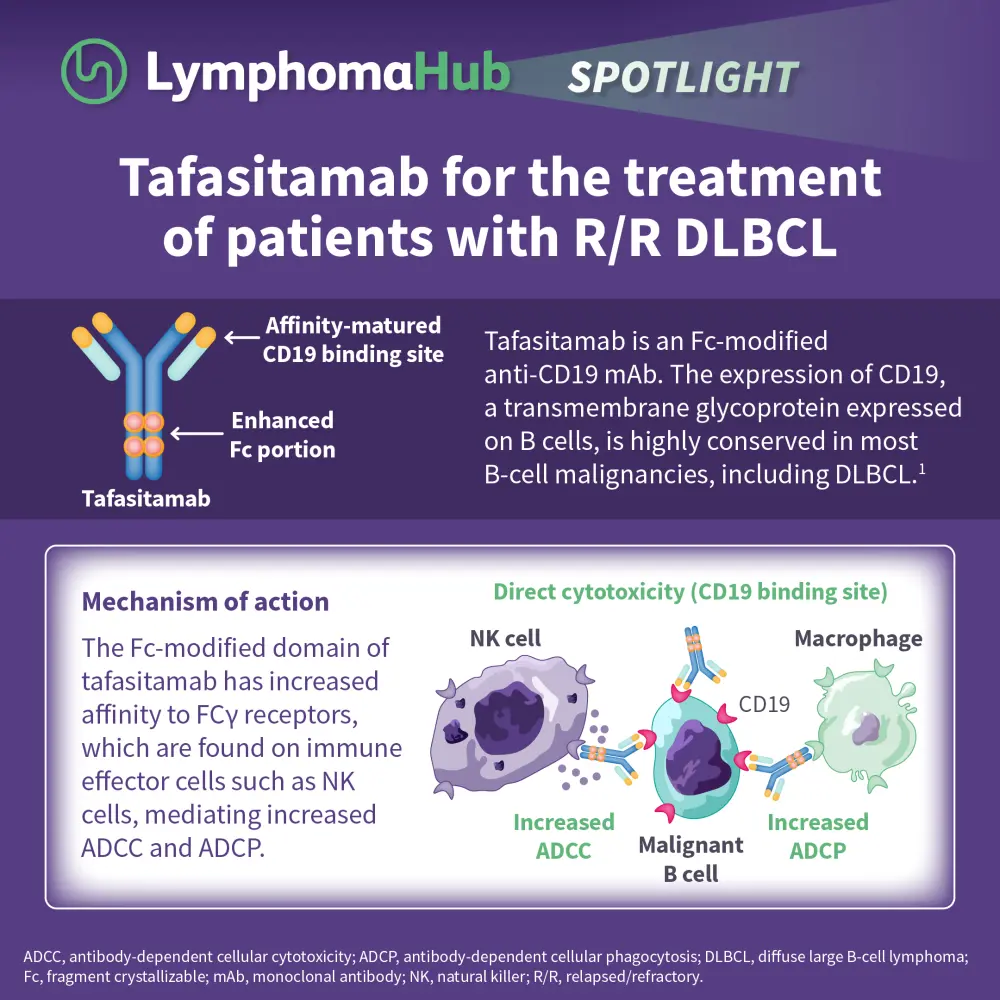
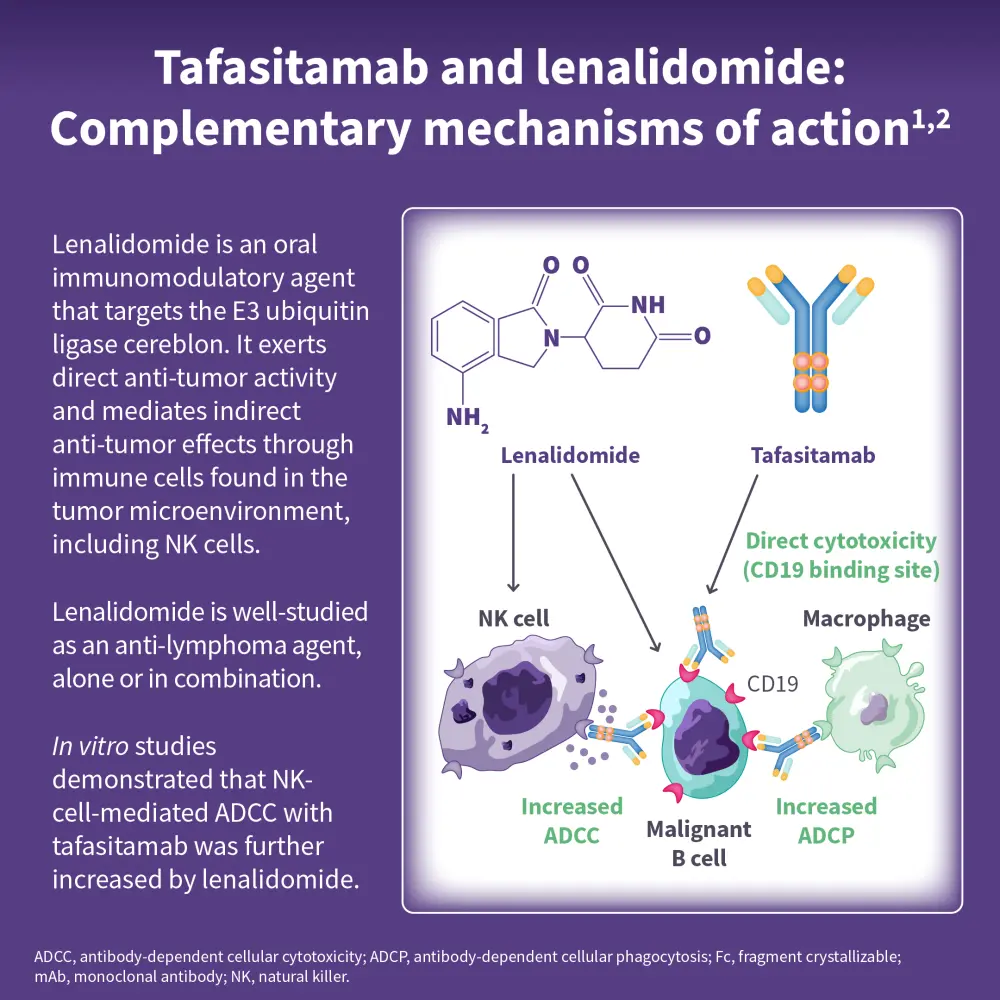
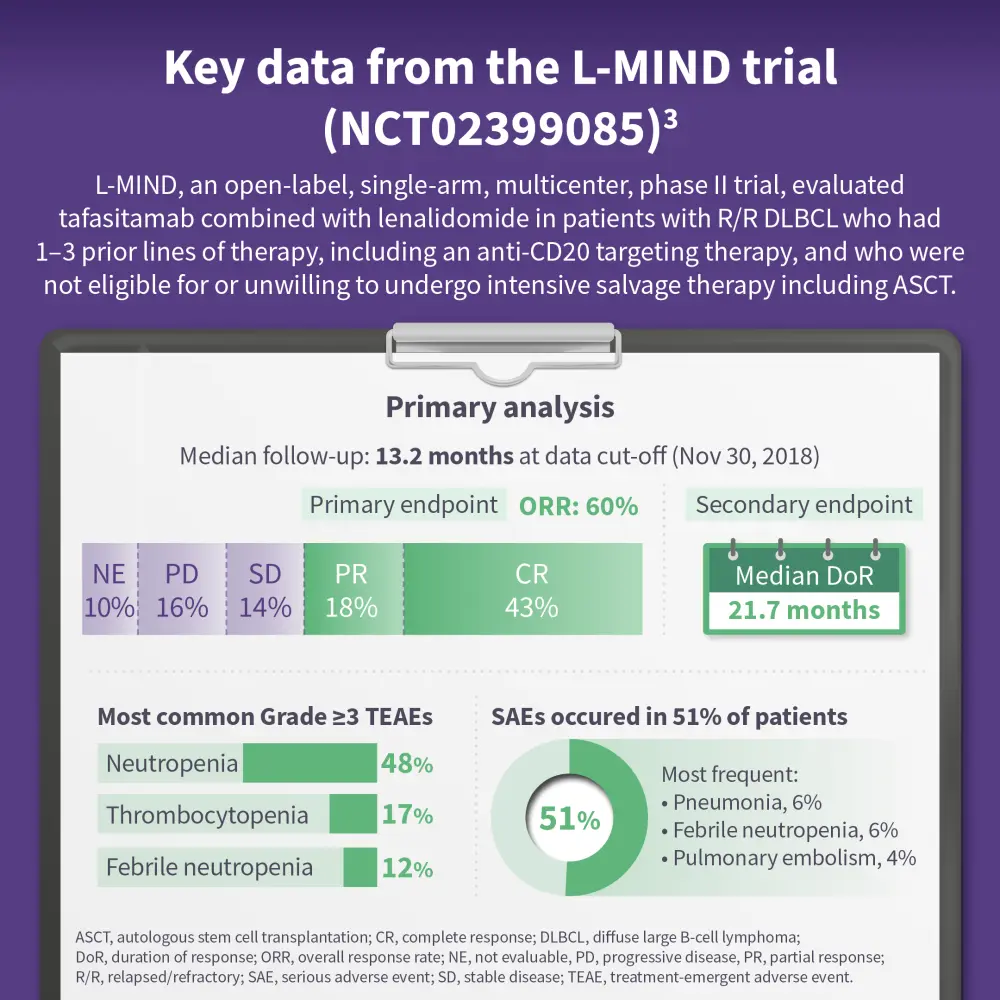
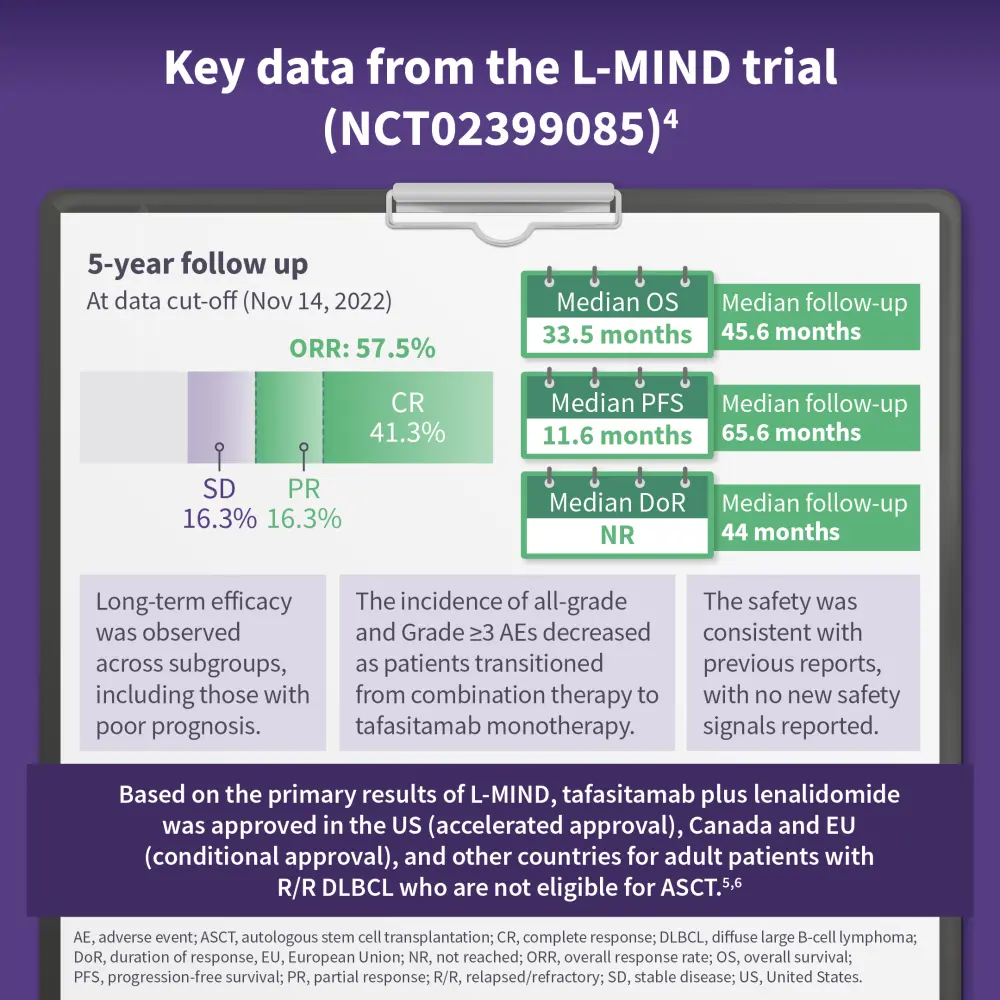
Tafasitamab, an anti-CD19 monoclonal antibody, targets the CD19 protein on B cells, which is prevalent in B-cell malignancies such as diffuse large B-cell lymphoma (DLBCL). By binding to CD19, tafasitamab induces programmed cell death in malignant B cells and improves immune responses through mechanisms such as antibody-dependent cellular cytotoxicity and antibody-dependent cellular phagocytosis. Combining tafasitamab with lenalidomide, an immunomodulatory agent, leverages their complementary actions. Lenalidomide stimulates T cells and natural killer cells, disrupting tumor-promoting pathways and boosting the immune response. In the L-MIND (NCT02399085) trial, tafasitamab demonstrated a 60% overall response rate, with a median duration of response of 21.7 months, supporting its approval as second-line therapy for relapsed/refractory DLBCL in the US and EU for patients ineligible for autologous stem cell transplantation. The ongoing firmMIND (NCT05429268) trial continues to assess the efficacy and safety of tafasitamab plus lenalidomide in relapsed/refractory DLBCL.

This educational resource is independently supported by Incyte. All content is developed by SES in collaboration with an expert steering committee; funders are allowed no influence on the content of this resource.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:


.webp&w=3840&q=75)


